Symptomatic Os Vesalianum Pedis in Young Adult A Case Report
Os vesalianum pedis is a rare accessory foot ossicle, which is located proximal to the base of the fifth metatarsal bone. This anatomic variant is usually asymptomatic and detected incidentally on routine foot radiographs. However, it can be an infrequent cause of lateral foot pain and rarely become symptomatic following traumatic injuries to the ankle or foot. To date, there are few reported cases of symptomatic os vesalianum pedis described in the literature and most of them were treated surgically. We report a case of symptomatic os vesalianum pedis in a young adult female, which was misdiagnosed initially and managed conservatively with physiotherapy. Patient’s symptoms regressed completely after a few sessions of physiotherapy and didn’t require surgical intervention. We intended to publish this case to increase the awareness of this rare entity among radiologists and clinicians.
Introduction
Anatomic variations are common in the foot and ankle, including accessory ossicle, bipartition and coalition [1]. The reported incidence of the most common accessory ossicles of the foot in descending order is accessory navicular (11.7%), os peroneum (4.7%), os trigonum (2.3%), os supranaviculare (1.6%), os supratalare (0.2%), and os intermetatarseum (0.2%) [2]. Os Vesalianum Pedis (OVP) is a rare accessory ossicle of the foot with reported incidence ranging between 0.1% and 0.5%, but some series reported a prevalence as high as 6% [3]. It is named after its illustrator, Andreas Vesalius, who first defined this variation in his illustrated anatomy book ‘De Humani Corporis Fabrica’ published in the 16th century [4].
OVP is located proximal to the base of the fifth metatarsal bone within peroneus brevis tendon [5]. Similar to other accessory ossicles in the foot, OVP is typically asymptomatic and found incidentally on routine radiographs or after an acute injury to the foot [6]. However, in a few reported cases, it can be the cause of lateral foot pain [1]. Even though OVP is described as bilateral by some authors [6], a review study including more than 1500 bilateral foot radiographs did not find any case with bilateral os vesalianum pedis [7].
29-year-old female with no significant prior medical or surgical history. She presented to the emergency department in our hospital with one-year history of on and off lateral right foot pain, which has progressed over the past two months. She did not report a history of trauma or intense athletic activities. The patient localized the pain to the base of the fifth metatarsal bone and described both mechanical and inflammatory pain findings. On physical examination, the ankle-foot alignment was maintained with normal range of motion, no pain on resisted plantar flexion or eversion, and there was no skin ecchymosis.
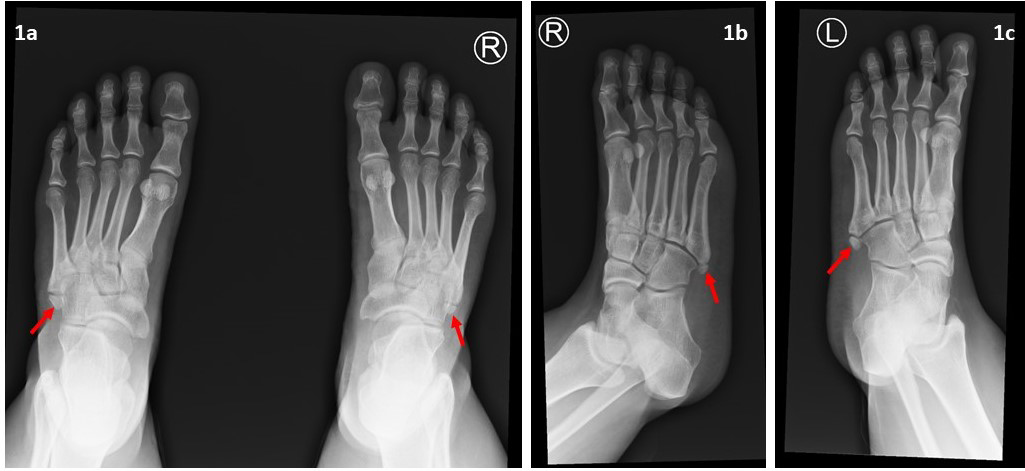
Bilateral foot radiograph was requested at that time and was interpreted initially as bilateral unfused apophysis (Figure 1). The patient was discharged home on oral analgesia and given an appointment to the orthopedic clinic after three weeks. During this time, the patient continues to complain of lateral right foot pain, which has not improved by analgesics. MRI of the ankle and foot was requested by the orthopedic surgeon to assess ligamentous injuries.
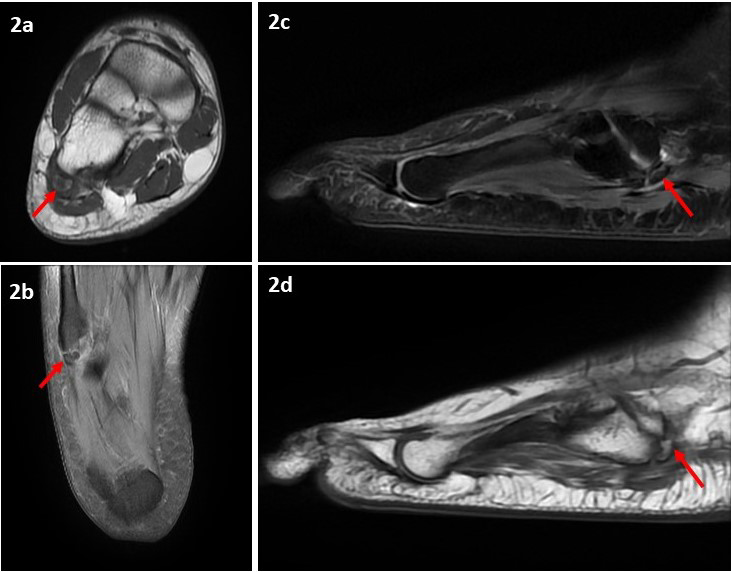
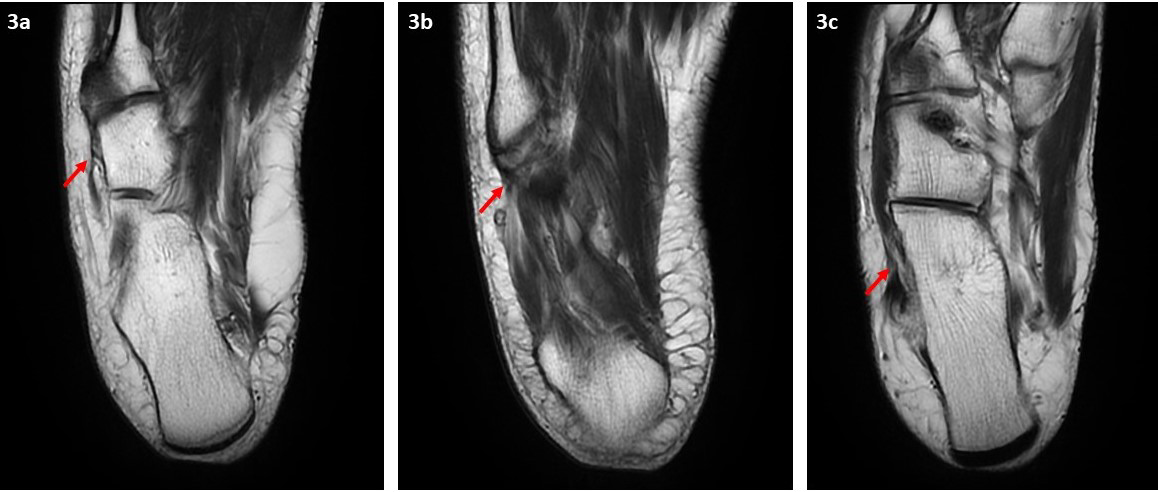
MRI of the right ankle (Figure 2) and foot (Figure 3) confirmed the diagnosis of OVP and demonstrated the presence of peroneus brevis tendinosis secondary to chronic mechanical stress. The patient received multiple sessions of physiotherapy; each is two weeks apart and was symptoms free after the fifth session.
Discussion
Few theories exist about the exact origin of OVP. The first theory suggests the OVP is unfused apophysis which in normal circumstances, closes at the age of 12 years for girls and 14 years for boys [8]. The second theory proposes that OVP is caused by pseudarthrosis of avulsion fracture of fifth metatarsal tuberosity. However, the third and most widely accepted theory is that OVP is a true sesamoid bone as manifested by the presence of an articular cartilage [6].
Although Symptomatic OVP usually presents with lateral foot pain localized at the fifth metatarsal base, the presence of OVP does not merely indicate that it will be symptomatic [6]. There are numerous cases of asymptomatic OVP, which were detected incidentally. It is not exactly known which factors are responsible for initiating the pain in symptomatic cases [9]. In this presented case, the patient had no antecedent traumatic event and did not report any intense athletic activity. On the contrary, in the previously reported symptomatic OVP in the literature, initiation of symptoms was either after an acute traumatic event or related to repetitive microtrauma [6]. More logically, pain is attributed to the chronic inflammation caused by synchondrosis joint instability after repeated microtrauma or acute trauma triggering the pain. This is explained by the presence of chronic tendinosis of the peroneus brevis muscle in the majority of the reported cases.
Numerous different entities which have similar radiographic appearance can be confused with OVP. However, when given an attentive look, OVP has some distinct characteristics that help in prompt diagnosis. OVP is usually separated from the fifth metatarsal base by a synchondrosis joint line having a constant width that follows an oblique course with the long axis of the fifth metatarsal bone. The ossicle is oval in shape and surrounded by cortical bone. However, the most remarkable radiographic feature of OVP is that it articulates with the cuboid bone [3]. In the context of trauma, OVP may be misdiagnosed as a fifth metatarsal base avulsion fracture. This can be differentiated by the lack of cortical bone in the avulsed fragment and the sharp edges of the fracture line [6]. Os peroneum, an accessory ossicle of the foot which is close to the base of the fifth metatarsal bone, should be kept in mind in the differential diagnosis as well. It is embedded in the tendon of the peroneus longus muscle and can be mixed with OVP in oblique foot radiographs. However, os peroneum has bean-shape and is smaller than OVP [5]. In skeletally immature patients, normal fifth metatarsal apophysis is located in the planter aspect of the fifth metatarsal tuberosity. It appears as small shell-shaped bone parallel to the fifth metatarsal shaft [4]. In skeletally mature patients and in the absence of acute traumatic events, unfused apophysis can be confused with OVP, as in our case.
Foot radiograph alone is considered diagnostic for OVP, but in some cases MRI of the foot is requested to assess the adjacent tendons for the presence of tear or chronic tendinosis. Scintigraphy is reported to be sensitive but not specific in differentiating between symptomatic versus asymptomatic OVP [5].
Initial treatment of symptomatic OVP should start with rest, limited weight-bearing, stretching exercises, analgesics like nonsteroidal anti-inflammatory drugs (NSAIDs) and casting [9]. If these measures fail, surgical options should be considered. Surgical options include excision of OVP without disruption of peroneus brevis tendon insertion, osteosynthesis as well as bone grafting [10]. Above all, it is crucial to ensure that OVP is the cause of the lateral foot pain in order to avoid unnecessary treatment.
Conclusion
OVP is a rare accessory ossicle of the foot that can be perceived as numerous pathologies at the fifth metatarsal base, including fracture. A high index of suspicion is needed in order to reach the correct diagnosis and avoid unnecessary treatment. We intended to publish this case to increase the awareness of this rare entity among radiologists and clinicians.
Declaration
Consent for Publication
Informed consent was obtained from the subject for this case report and all imaging studies. Proof of consent can be provided on request.
Funding
This case report received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Competing Interests
The authors declare that they have no conflict of interest.
References
-
Coskun N, Yuksel M, Cevener M, Arican RY, Ozdemir H, et al. (2009) Incidence of accessory ossicles and sesamoid bones in the feet: a radiographic study of the Turkish subjects. Surg Radiol Anat 31(1): 19-24.
-
Cilli F, Akçaoğlu M (2005) The incidence of accessory bones of the foot and their clinical significance. Acta Orthop Traumatol Turc 39: 243-246.
-
Tsuruta T, Shiokawa Y, Kato A, Matsumoto T, Yamazoe Y, et al. (1981) Radiological study of the accessory skeletal elements in the foot and ankle (author’s transl). Nihon Seikeigeka Gakkai Zasshi 55(4): 357-370.
-
Aykanat F, Vincenten C, Cankus MC, Kose O, Sindel M (2019) Lateral foot pain due to os vesalianum pedis in a young football player; a case report and review of the current literature. Skeletal Radiol 48(11): 1821-1828.
-
Dorrestijn O, Brouwer RW (2011) Bilateral symptomatic os vesalianum pedis: a case report. J Foot Ankle Surg 50(4): 473-475.
-
Mousafeiris VK, Papaioannou I, Kalyva N, Arachoviti C, Repantis T (2021) Os vesalianum pedis in a young adult: a case report and literature review. Cureus 13(5): 14896.
-
Correia MDC, Lopes TR (2022) Knowing Your Accessory Foot Ossicles and Avoiding Misdiagnoses: A Case Report of Painful Os Vesalianum Pedis. Cureus 14(7).
-
Canale ST, Williams KD (1992) Iselin’s disease. J Pediatr Orthop 12(1): 90-93.
-
Kose O (2009) Os vesalianum pedis misdiagnosed as fifth metatarsal avulsion fracture. Emerg Med Australas 21(5): 426.
-
Boya H, Ozcan O, Tandoğan R, Günal I, Araç S (2005) Os vesalianum pedis. J Am Podiatr Med Assoc 95(6): 583- 585.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage