Spontaneous Rupture of the Fornix Following an Obstructive Distal Lithiasis of the Ureterovesical Junction A Case Report and Literature Review
Spontaneous rupture of the fornix is a rare urological pathology. The urinary tract obstruction is the most frequent etiology. We report here a case with short review of spontaneous rupture of the fornix due to distal lithiasis of the left ureter. The patient was 26 years old, with no particular pathological medical or surgical history, admitted for sudden and intense left low back pain, suffered from the past five days and increasing in intensity with onset of fever. The patient consulted a general practitioner on local clinic where an infectious assessment was requested before the prescription of anti-inflammatory and board spectrum antibiotic to decapitate a probable urinary tract infection. The pain did not disappear under the treatment. The decision was then to refer the patient for urology specialized care. Spontaneous rupture of the fornix is rare but must always be taken into account in the differential diagnosis of pathologies occurring in a febrile patient or presenting with an acute abdomen after episodes of acute low back pain. The often non-specific clinical symptoms will regress after the rupture except in certain cases like ours. The diagnosis is guided by the interrogation, suspected on ultrasound, and confirmed by computed tomography. With a low pressure system by urinary diversion and antibiotic treatment in some cases, the result is excellent. Endoscopic drainage for a better urinary diversion contributes to a good evolution of the patients.
Introduction
Spontaneous rupture of the upper excretory tract is a rare complication of obstructive uropathy. The most often etiology is urinary tract obstruction especially by urinary lithiasis. However, other causes of obstruction exist such as posterior urethral valves, prostatic hyperplasia, sometimes urethral stenosis, renal trauma, pelvic neoplasms, pregnancy, abdominal aortic aneurysm and retroperitoneal fibrosis.
Some studies show that etiology in many cases remains unclear. In patients with acute colic, infusion excretory urography carries a substantial risk of fornix’s rupture due to the osmotic diuresis created by the contrast medium. Continuously increasing pressure can lead to distension, followed by rupture of the renal pelvis and extravasation of urine into the perirenal area. The renal pelvic calyx system is unable to withstand the increased internal pressure and ruptures at the point where the tissue is weakest. As flank pain is the most typical symptom of urinary obstruction, the typical clinical sign of forniceal rupture is sudden diminution of pain due to the reduction of stasis and pressure. It was different in our case where the pain persisted until the patient‘s intervention time in emergency. We report here a case of spontaneous rupture of the fornix due to a distal lithiasis of the left ureter with the aim to make note and share with other clinicians the possibility of persisting pain in rupture of fornix with possible imaging manifestations revealing this pathology and short review the possible etiologies.
Case Presentation
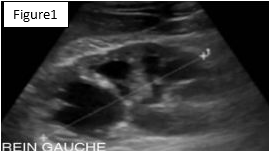
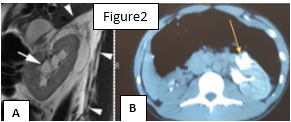
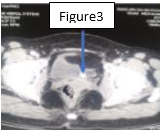
The patient was a 26 years old man, driver living in Casablanca, with no particular pathological medical or surgical history and no family history. The patient was presented to the urology emergency service for left low back pain for five days ago. According to the interview, the patient had suffered from sudden, intense, grinding-type left low back pain, radiating to the iliac fossa and external genitalia that increases in intensity with onset of fever. The patient consulted a general practitioner where an infectious assessment was requested before the prescription of anti- inflammatory and board spectrum antibiotic to decapitate a probable urinary tract infection. The symptoms did not disappear even if the treatment was initiated. The decision was then to refer the patient for specialized care. General physical examination was carried out and noted a performance status at 2, a fever at 38.2°Celcius, a heart rate at 88 beats per minute and a blood pressure at 112/71 mmHg. No macroscopic hematuria, dysuria or burning during urination reported but the urine dipstick was positive. A physical abdominal and genitourinary examination found tenderness of the left lumbar and iliac fossa. There were no palpable abdominal mass or signs of inflammation of the external genitalia. The rectal examination noted normal prostate without pain. The major timepoint includes consultation at the local clinic , request of infectious assessment and prescription of anti-inflammatory based on profenid 100mg once a day with ciprofloxacin 500mg twice a day by the general practitioner five days before being addressed to our emergency service. Biologic result revealed an inflammatory syndrome (hyperleucocytosis at 12000 elements/mm3 with granulocyte predominance, a sedimentation rate at 70mm on the 1st hour, a C-reactive protein at 103ng/ml), normal renal function with plasma creatinine at 8.3mg/l, serum potassium at 4.2 mmol/l, urea at 0.37g/l and cytobacteriological examination of the urine was sterile. The urinary tract radiography without preparation showed no abnormality; ultrasound of the urinary tract noted left uretero-hydronephrosis with perirenal fluid collection and fat infiltration (Figure 1). The computed tomography of the urinary tract had confirmed the presence of uretero- hydronephrosis with urinoma (Figure 2A), contrast medium extravasation related to a rupture of the left kidney fornix (Figure 2B), and a distal lithiasis of the left ureter (distal lithiasis of ureterovesical junction with 4mm in diameter) (Figure 3). According to imaging results, the persistence of left low back pain and the hydronephrosis collection given the confirmed fornix rupture on computed tomography make this case particular from other cases already reported. Our emergency management was the endoscopic rise of double J stent for urinary drainage after proximal urine sampling and then initiation of probabilistic antibiotic therapy. This led to clinical and biological improvement.
Discussion
Spontaneous rupture of the fornix is a rare but often urological emergency that may be accompanied by loss or impairment of renal function. In current practice, many clinicians have little experience of the particular clinical situation of this pathology, and making the correct diagnosis is often complicated by the fact that the clinical signs and especially the pain will improve abruptly and disappear after rupture of the fornix and the resulting lack of urinary stasis. This fits with our case where the left lumbar pain which according to the interview was intense five days before but was persistent on admission associated to a left lumbar tenderness on palpation with onset of fever. The other particular symptoms that could sign the rupture of the fornix such as acute abdomen in case of urinoma, hemodynamic instability, hematuria, digestive disorders such as nausea and vomiting were not present in our case. Faced with the difficult clinical diagnosis, imaging takes place to make clear the diagnosis and to identify the cause. If nephrosonography findings do not match clinical symptoms, further diagnostic examination by computed tomography is necessary [1]. Thus in our case, the urinary tract radiography without preparation showed no abnormality. This may be the fact that according to etiology, some lithiasis is radiolucent. The ultrasound of the urinary tract noted left ureterohydronephrosis with fluid collection and an infiltration of perirenal fat. No lithiasis was noted on the ultrasound. This would be due to the fact that small stones are not commonly seen on ultrasound. Also, ultrasound cannot explore the entire ureteral path except in case of major dilation but the average potion is never well explored by ultrasound. The uro-cumputed tomography confirmed the presence of ureterohydronephrosis with urinoma, contrast medium extravasation related to rupture of the left kidney fornix and retromeatic lithiasis of the left ureter. It is possible that a urinary tract infection could cause perinephric failure on Computed tomography, and that this could be mistaken for forniceal rupture [2]. However, the urine culture was sterile in our patient. The persistence of the ureterohydronephrosis or stasis after fornix’s rupture constitute the particularity in our case. Other stadies reported absence of urinary stasis in case of fornix’s rupture [3]. The persistence of the ureterohydronephrosis in our case could be due to the fact that the lithiasis was in distal portion. In our case, an obstructive lithiasis of the ureterovesical junction was the etiology of the rupture of the fornix. Thus, in other studies reported previously, distal ureteral lithiasis were the most identified causes of obstruction leading to rupture of the fornix [4, 5, 6]. This agrees with our case and a possible explanation for these findings is the way of selection, in which stones are more likely to pass distally to the vesicoureteral junction where they eventually become obstructive [7]. However, other obstructive or compressive etiologies exist and may involve different levels of the ureter as described in other studies. These etiologies include obstruction following pregnancy [8, 9], existence of posterior urethral valves [10], obstruction by ureteropelvic junction syndrome [11], extrinsic vascular compression, trauma, iatrogenic causes [12] and sometimes the existence of an obstacle under the bladder [13]. In such situations, emergency intervention to remove the obstacle is sometimes essential. Percutaneous nephrostomy tube or retrograde ureteral stent is the most used method of drainage. Several factors can influence this decision of intervention and include the alteration vital signs of the patient, the febrile state or presence of the signs of the infection, the patient’s discomfort such as severe pain, acute abdomen, nausea or vomiting [12]. In our case, fever pain with biological symptoms of infection were present and motivated intervention. As noted in the study of Nedjim SA, et al. [14], the primary objective of the treatment is to reduce the pressure in the upper urinary tract. Our emergency management was the endoscopic rise of double J stent for urinary drainage after proximal urine sampling and then initiation of probabilistic antibiotic therapy rest and monitoring during hospitalization. The placement of a retrograde ureteral stent is preferable to the placement of a nephrostomy probe since the placement of a percutaneous nephrostomy probe is technically delicate [15]. As proved in several studies, rapid drainage of urine on the affected side area is essential for the further course of the disease [16, 17]. The ultimate evolution was favorable marked by the amendment of the fever and clinical signs, the regression of the inflammatory syndrome. As indicated in the literature [18, 19], Control with imaging was done and no signs of ureterohydronephrosis or major urinoma were observed on Computed Tomography and ultrasonography performed after a follow-up period of 5 days after intervention. This led to confirm the good clinical and biological evolution of the patient and the patient was discharged 10 days after this intervention. Laser ureteroscopy with fragmentation of the lithiasis was done one month after discharge.
Conclusions
Spontaneous rupture of the fornix is rare but should always be considered in the differential diagnosis to patient with an acute abdomen. Fever and inflammatory syndrome may follow acute low back pain. Symptoms will improve with conservative management. Faced with the paucity of specific clinical signs, the diagnosis is guided by questioning or interview, suspected on ultrasound and confirmed by computed tomography. Spontaneous rupture of the fornix may potentially benefit from urinary diversion with broad- spectrum antibiotic and clinicobiological monitoring and consider follow-up imaging later. This establishment of a low pressure system by drainage with antibiotic treatment offers excellent results. Endoscopic treatment for a better clearing or urinary diversion contributes to a good evolution of the patients and placement of a retrograde ureteral stent is preferable since the placement of a percutaneous nephrostomy probe is technically delicate.
Declarations
Consent for Publication
Consent was obtained from the patient for publication of this case.
Competing Interest
There is no competing of interest.
Funding
There is no funding or financial support for the conduct of the research.
Acknowledgment
At the end of this work, we would like to express our sincerely thanks to all the people who contributed to its writing especially to the following authors: At the end of this work, we would like to sincerely thank all the people who contributed to its writing, To Dr. Ndayishimiye from department of radiology department for your confirming images.
References
-
You JS, Chung YE, Lee JY, Lee HJ, Chung TN, et al. (2012) The spontaneous rupture of the renal fornix caused by obstructive nephropathy. J Emerg Med 43(3): 488-489.
-
Breun H, Csapo Z, Sigel A (1989) Fornix Rupture, Überprüfung der Pathophysiologie und der Klinik. Urologe 28: 329-333.
-
Gershman B, Kulkarni N, Sahani DV, Eisner BH (2011) Causes of renal forniceal rupture. BJU International 108(11): 1909-1912.
-
Pais JMJ, Agudo VPC, Moldes MR, Breijo SM, Abad VC, et al. (2007) Lithiasic obstructive uropathy with fornix rupture. Actas Urol Esp 31(10): 1199.
-
Fukatsu T, Tajima K, Saitou K (2001) Rupture of renal pelvis due to urolithiasis: report of two cases. Hinyokika Kiyo 47(1): 39-42.
-
Koktener A, Unal D, Dilmen G, Koc A (2007) Spontaneous rupture of the renal pelvis caused by calculus: a case report. J Emerg Med 33(2): 127-129.
-
Eisner BH, Pedro R, Namasivayam S, Kambadakone A, Sahan DV, et al. (2008) Differences in stone size and ureteral dilation between obstructing proximal and distal ureteral calculi. Urology 72(3): 517-520.
-
Quinn AD, Kusuda L, Amar AD, Das S (1988) Percutaneous nephrostomy for treatment of hydronephrosis of pregnancy. J Urol 139(5): 1037-1038.
-
Satoh S, Okuma A, Fujita Y, Tamaka M, Nakano H (2002) Spontaneous rupture of the renal pelvis during pregnancy: a case report and review of the literature. Am J Perinatol 19(4): 189-195.
-
Ahmed S, Borghol M, Hugosson C (1997) Urinoma and urinary ascites secondary to calyceal perforation in neonatal posterior urethral valves. Br J Urol 79(6): 991- 992.
-
Hirselj DA, Zmaj PM, Firlit CF (2009) Occult ureteropelvic junction obstruction presenting as anuria and urinary ascites in an infant with antenatal unilateral hydronephrosis. J Pediatr Urol 5(5): 405-407.
-
Bannowsky A (2008) Iatrogenic fornix rupture caused during retrograde manipulation of the ureter: a case report. Cases J 1(1): 320.
-
Singh I, Joshi M, Mehrotra G (2009) Spontaneous renal forniceal rupture due to advanced cervical carcinoma with obstructive uropathy. Arch Gynecol Obstet 279(6): 915-918.
-
Nedjim SA, Abdi M, Afifi MA, Hagguir H, Mahanna HA, et al. (2021) Spontaneous rupture of the fornix due to a ureteral lithiasis of 3 mm causing a urinoma: report of an original case. Radiol Case Rep 16(10): 3143-3146.
-
Doehn C, Fiola L, Peter M, Jocham D (2010) Outcome analysis of fornix ruptures in 162 consecutive patients. J Endourol 24(11): 1869-1873.
-
Kalafatis P, Zougkas K, Petas A (2004) Primary ureteroscopic treatment for obstructive ureteral stone- causing fornix rupture. Int J Urol 11(12): 1058-1064.
-
Al-Mujalhem AG, Aziz MS, Sultan MF, Al-Maghraby AM, Al-Shazly MA (2017) Spontaneous forniceal rupture: can it be treated conservatively? Urol Ann 9(1): 41-44.
-
Yanaral F, Ozkan A, Cilesiz NC, Nuhoglu B (2017) Spontaneous rupture of the renal pelvis due to obstruction of pelviureteric junction by renal stone: a case report and review of the literature. Urol Ann 9(3): 293-295.
-
Hakan E, Erbay T, Bugra SA, Alma E, Ünal U, et al. (2018) Etiology and treatment of renal forniceal rupture: a single center experience. J Urol Surg 5(2): 68-72.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage