Emergency Ultrasound: Hypoechoic Submucosa as Sign of Active Bowel Inflammation - Case Report
Ultrasound is a radiological examination method that is often used in daily practice for the diagnosis of various abdominal conditions that can be very complex. Very often, patients present for an examination with non-specific abdominal pain accompanied by discrete changes in the stool, which can lead to diagnostic confusion in the case of a normal ultrasound finding in the abdomen. Many radiologists have minimal experience with bowel ultrasound outside of basic indications such as appendicitis and intususception and may be uncomfortable interpreting images for other diagnosis. In our paper, we present a case of ileitis in which the diagnosis was established by ultrasound findings of hypoechoic submucosa of the terminal ileum segment along the mesenteric edge. Submucosal hypoechogenicity of the ileum can be the only sign of primary inflammation of the ileum, but also a secondary ultrasound sign of appendicitis, while in our case hypoechogenicity of the submucosa was present only on the mesenteric side of the ileum, which enabled the initial diagnosis of ileitis and the initiation of conservative therapy. Bowel ultrasound is an important diagnostic procedure in the emergency department in cases of acute abdominal pain, which in a large percentage of cases enables the triage of these patients for surgical or medical treatment.
Introduction
Ultrasound is a radiological examination method that is often used in daily practice for the diagnosis of various abdominal conditions that can be very complex. Very often, patients present for an examination with non-specific abdominal pain accompanied by discrete changes in the stool, which can lead to diagnostic confusion in the case of a normal ultrasound finding in the abdomen.
There are many obstacles to the widespread use of bowel ultrasound in clinical practice. Given its relatively new nature, many have not received any formal training on the subject. Sonographers, even pediatric sonographers, who have experience with bowel ultrasound have previously used it mainly to look for appendicitis or intussusception. Similarly, many radiologists have minimal experience with bowel ultrasound outside of these indications and may be uncomfortable interpreting images for other diagnosis [1, 2].
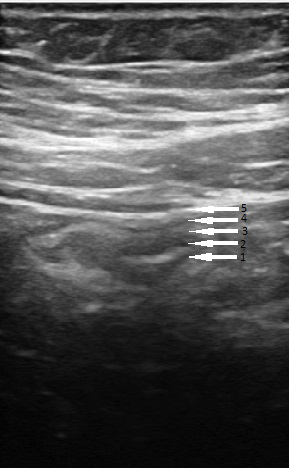
The basic elements of ultrasound diagnostics of the intestine are wall thickness, lumen width, stratification, compressibility, vascularization, peristalsis and mesentery (Figure 1). Stratification of the wall is a very important element of ultrasound diagnostics of the intestine - if it is present, the probability that it is a malignant disease is quite small (Figure 2). The submucosa is the third layer of a total of 5 layers of the intestinal wall and is normally hyperechoic due to its conntective tissue content. In the case of intestinal wall edema, the submucosa most often becomes hypoechoic, which most often happens in cases of inflammation in the digestive tract.
In our paper, we present a case of ileitis in which the diagnosis was established by ultrasound findings of hypoechoic submucosa of the terminal ileum segment along the mesenteric edge.
Case Report
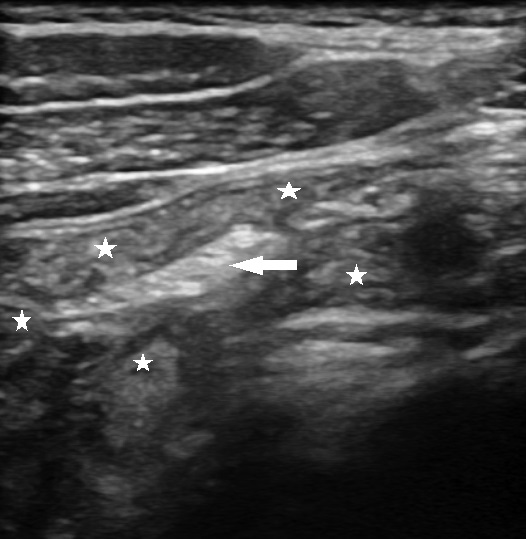
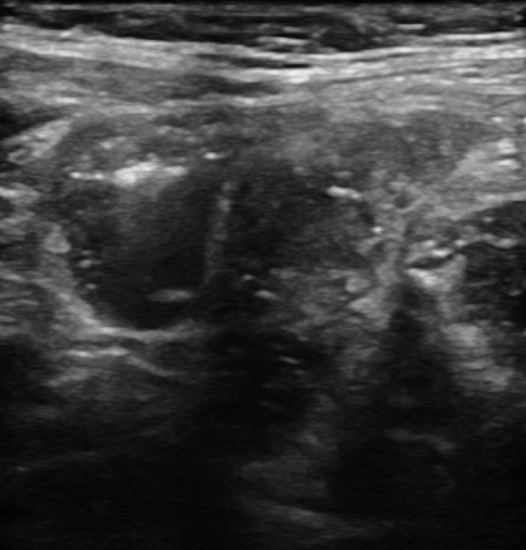
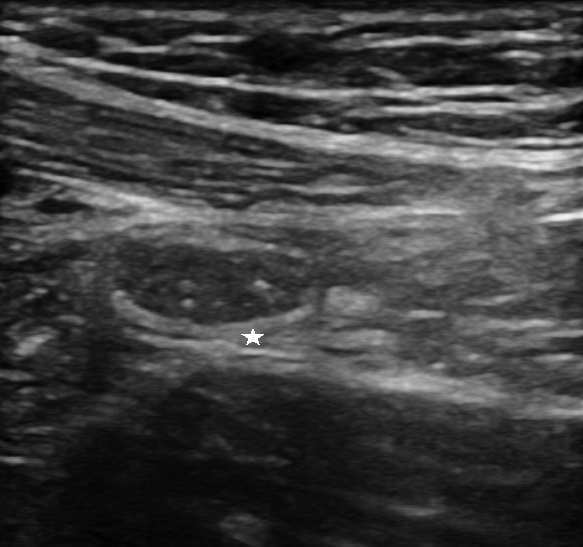
A 30-year old man was admitted to the emergency department with abdominal pain located in right illiac fossa and diarrhea. On physical examination, there was tenderness on the right lower quadrant at palpation with positive Blumberg sign. Blood tests revealed slighty elevated white blood cell count 12.1x10^9 (3.4-9.7x10^9/L), other parameters were within normal range. Ultrasonography examination showed normal appearance of appendix but hypoechoicity in the submucosal layer along the mesenteric edge of the terminal ileum without any changes in mesentery and without free fluid between loops (Figures 3,4). On ultrasound examination, the terminal ileum was of normal wall thickness, preserved stratification, normal vascularization, with small amount of intraluminal fluid, compressible with normal colonic ultrasound finding so initial ultrasound diagnosis of ileitis was made (Figure 5).


Because of the ultrasound findings, conservative therapy was prescribed to the patient and coproculture and fecal calprotectin analyzes were requested. Coproculture showed a normal result, while the fecal calprotectin values were slighty elevated (350 μg/mg) so conservative therapy was continued. The patient’s general condition and laboratory data improved after 10 days so follow up US examination of the abdomen was performed, which showed normal echogenicity of ileal submucosa (Figure 6).
Discussion
From the esophagus to the rectum, the gastrointestinal tract has a typical multilamellar sonographic appearance, which results from its organized and highly stratified histology. This is useful for at least two reasons: This pattern allows the sonographer or radiologist to distinguish the bowel from adjacent structures, and the disorder of the pattern helps in the diagnosis intestinal pathology. Masses can they cross layers while edema can expand certain layers or obscure their edges. Numerous authors have emphasized bowel wall thickening as a key sonographic feature in diagnosing gastrointestinal lesions. However, analyzing the specific pattern of echogenicity of the thickened bowel wall segment and correlating it with the acuity of the disease process or CT has received relatively little emphasis.
On sonography, the submucosal layer is the most prominent echogenic layer of the bowel wall that defines the “sonographic signature” of the bowel [3]. Signs of ileal inflammationon US include a thickened terminal ileal wall (between 1.5 and 3mm), luminal narrowing and hyperaemia [4]. Rarely, there is normal wall thickness of ileum with hypoechoic swollen ileal folds in the edematous mucosa and submucosa and these findings should be related to clinical and laboratory data [5]. In the case of clinical laboratory suspicion of acute appendicitis, ultrasound is the initial radiological examination method. Direct ultrasound means of acute appendicitis are safe and most often lead to an accurate diagnosis. In a certain percentage of cases, the appendix cannot be visualized on an ultrasound examination. There are varying rates quoted in the literature for the appendix being seen, between 24.4% and 69.3% [6]. In this situation, it is important to actively assess for the secondary features often seen which may help direct further management. Repeating the examination after a few hours has been shown to significantly increase the sensitivity of US [7]. One of the secondary ultrasound features of acute appendicitis is the thickening of the wall of the terminal ileum, which in this case has preserved stratification and circumferentially hypoechoic submucosa. In our case, the wall of the ileum was of normal thickness, but a hypoechoic submucosa was verified along the mesenteric side of the ileal wall, which may indicate that the primary inflammatory process is localized on the ileum and not on the appendix, which in our case was visualized without any ultrasound sign of inflammation, so we made the diagnosis of ileitis.
From the point of view of the emergency physician, the importance of detecting hypoechoicity of the submucosa of the ileum along the mesenteric side is great, especially in the absence of visualization of the appendix. Submucosal hypoechogenicity of the ileum can be the only sign of primary inflammation of the ileum, but also a secondary ultrasound sign of appendicitis, while in our case hypoechogenicity of the submucosa was present only on the mesenteric side of the ileum, which enabled the initial diagnosis of ileitis and the initiation of conservative therapy. Bowel ultrasound is an important diagnostic procedure in the emergency department in cases of acute abdominal pain, which in a large percentage of cases enables the triage of these patients for surgical or medical treatment.
References
-
Alexander KM, Chan SS, Opfer E, Cuna A, Khashu M, et al. (2021) Implementation of bowel ultrasound practice for the diagnosis and management of necrotising enterocolitis. ADC Fetal & Neonatal Edition 106(1): 96- 103.
-
Maturen KE, Wasnik AP, Kamaya A, Dillman JR, Kaza RK, et al. (2011) Ultrasound imaging of bowel pathology: technique and keys to diagnosis in the acute abdomen. AJR Am J Roentgenol 197(6): 1067-1075.
-
Kimmey MB, Martin RW, Haggitt RC, Wang KY, Franklin DW, et al. (1989) Histologic correlates of gastrointestinal ultrasound images. Gastroenterology 96(2): 433-441.
-
Alison M, Kheniche A, Azoulay R, Roche S, Sebag G, et al. (2007) Ultrasonography of Crohn disease in children. Pediatr Radiol 37(11): 1071-1082.
-
Puylaert JB, Van der Zant FM, Mutsaers JA (1997) Infectious ileocecitis caused by Yersinia, Campylobacter, and Salmonella: clinical, radiological and US findings. Eur Radiol **7**(1): 3-9.
-
Ang A, Chong NK, Daneman A (2001) Pediatric appendicitis in “real-time”: the value of sonography in diagnosis and treatment. Pediatr Emerg Care 17(5): 334-340.
-
Schuh S, Man C, Cheng A, Murphy A, Mohanta A, et al. (2011) Predictors of non-diagnostic ultrasound scanning in children with suspected appendicitis. J Pediatr 158(1): 112-118.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage