Unraveling the Genetic Complexity: A Case Report of MYLK Gene Mutation in a Patient with SCAD
Spontaneous Coronary Artery Dissection (SCAD) is a rare and potentially fatal disorder characterized by a tear in the wall of a coronary artery, leading to reduced blood flow to the heart. Although its exact cause remains elusive, SCAD is often associated with fibromuscular dysplasia and other connective tissue disorders. Here, we present a case of a 34-year-old African-American male with SCAD, hypertension, and obesity, whose family history included myocardial infarction, hypertension, and diabetes mellitus. Extensive imaging and cardiovascular evaluation revealed severe stenosis in the left anterior descending artery and a dissection flap in the left main coronary artery. Further genetic testing identified a variant of uncertain significance (VUS) in the MYLK gene, which has been linked to aortic dissections. While MYLK gene mutations have been reported in some SCAD and thoracic aortic aneurysm and dissection (TAAD) patients, they appear to be relatively rare. This case underscores the potential genetic basis of SCAD and highlights the importance of continued research to understand the role of MYLK gene mutations in SCAD and TAAD pathogenesis. Further investigation is warranted to determine the significance of the VUS identified in this patient.
Introduction
A rip in the wall of a coronary artery causes SCAD (Spontaneous Coronary Artery Dissection), a rare and potentially fatal disorder that reduces blood flow to the heart. It can happen as a consequence of a disturbance of the inner lining of the artery or spontaneous rupture of tiny capillaries supplying the arterial wall, resulting in decreased blood flow to the heart muscle. It is not brought on by trauma or medical operations. It can be brought on by stressful situations and is frequently related to underlying vascular disease. Fibromuscular dysplasia, which is present in 70- 90% of SCAD patients, is the biggest risk factor for more frequently found non-atherosclerotic SCAD [1].
A limited number of patients had reported cases of familial inheritance. It may be linked to hereditary conditions that affect the connective tissues in the artery wall, systemic inflammatory illnesses, hormonal treatments, and connective tissue disorders affecting the vascular Ehlers-Danlos syndrome, Marfan syndrome, and Loeys-Dietz syndrome. SCAD is frequently brought on by stressful situations such as mental stress, physical stress, drug usage, and stressful activities. Alport syndrome and polycystic kidney disease have both been linked to it in reports [2].
Evidence points to a genetic foundation for uncommon connective tissue disorders like SCAD and shows that gene mutations may play a role in these conditions. As a result, initiatives have been made to look for these mutations in SCAD patients.
Case Report
This is a case of a 34-year-old African-American male with HTN, obesity, and SCAD. He has presented with chest pain and a syncopal episode of one-week duration. His father with a history of MI and HTN and his mother with a history of DM and HTN. He initially experienced chest discomfort only during exertion, but passed out during a verbal altercation. There were no signs of seizures during the syncope episode. No recent infection, chills, fever, or nausea/vomiting were reported.
This patient has a New York Heart Association (NYHA) functional class of II. A recent EKG (1/28/2022) showed sinus bradycardia with a short PR interval and occasional supraventricular premature complexes, moderate T-wave abnormality, with a ventricular rate of 49, PR interval of 119, and QRS duration of 99. The patient was further evaluated by structural/interventional cardiology considering SCAD.
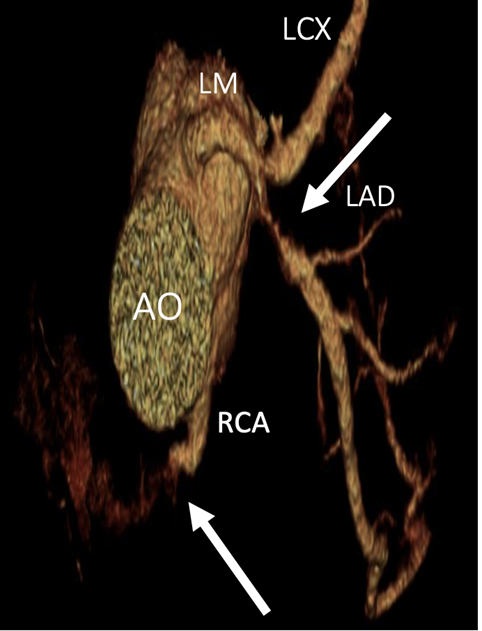
This patient underwent a coronary CTA on 1/26/2022 which revealed a dissection flap extending from the left main coronary artery to the proximal LAD that shows severe stenosis. Near total non-opacification of the RCA was suggested to be due to a long segment dissection flap excluding the proximal part of the RCA. A small dissection extending to the proximal LCX was also suspected. The patient’s troponin trend was elevated (102, 113, 147, 98, 76). A TTE on 1/27/2022 showed the heart to be grossly normal with an EF of 55-60% (Figure 1).
The patient consented to a left heart catheterization (LHC) which revealed that the distal portion of the left main coronary artery has a 10-20% tapering and LAD had an ostial focal 90% stenosis. The LAD supplies large D1 branch vessels, which are otherwise angiographically normal. The LCX is a large caliber non-dominant vessel that gives rise to a large bifurcating obtuse marginal (OM) vessel before continuing in the atrioventricular groove. The lower branch of OM1 has a 40-50% stenosis over a long segment, suggesting a healed prior dissection. The LCX supplies left to right collaterals to the right posterior descending artery (RPDA). The RCA was noted to have a chronic total occlusion proximally and the RPDA filled via left to right collaterals. Cardiovascular surgery was consulted and CABG was done on 1/31/2022 (Figure 2).
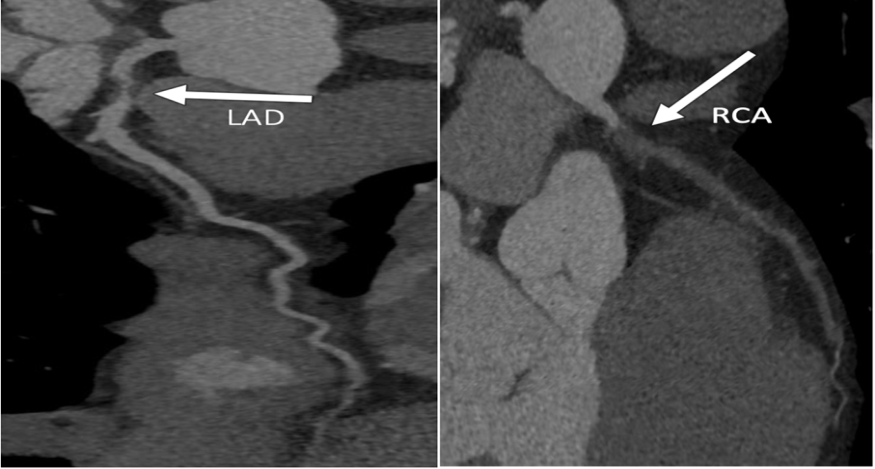
Source: Coronary CTA shows dissection and severe stenosis of proximal LAD, and dissection with non-contrast opacification of RCA (arrows). Figure 2: Curved MPR of LAD and RCA.
Patient is on a daily regimen of amlodipine, aspirin, atorvastatin, carvedilol, and clopidogrel. He also has access to oxycodone for pain relief as needed.
The patient was seen in the Cardiogenomics Clinic on 2/28/2022 to discuss genetic testing options and benefits and limitations. The patient was evaluated by a medical geneticist and genetic counselor and had a detailed discussion about genetic testing. A history of SCAD and HTN was noted. The patient has no syndromic features noted although epicanthal fold (maybe native American ancestry), a wide nasal bridge (uvula was not assessed), but no signs of Marfan syndrome. DDx includes other connective tissue disorders such as Loeys Dietz syndrome. The plan is to send a TAAD (thoracic aortic aneurysms and dissections) gene panel and he was counseled regarding the possibility of VUS and false negative test results.
The genetic testing results show that he has one variant of uncertain significance (VUS) in the MYLK gene. The MYLK gene has been associated with autosomal dominant TAAD. However, at this time, there is not enough evidence to determine the pathogenicity of this variant. The testing did not definitively identify a genetic explanation for his aortic dissection, but it does not rule out the possibility of a genetic contribution or inherited factor to his history. The patient should continue to follow recommendations from his Cardiology team, and close family members should be aware of this family history and consider a Cardiology evaluation. The patient will have a follow-up in 2-3 years.
Discussion
The exact cause of SCAD is not well understood, but some factors such as hormonal changes, physical stress, and connective tissue disorders may increase the risk of SCAD. MYLK (myosin light chain kinase) gene encodes a protein that is involved in the contraction of smooth muscle cells, including the smooth muscle cells in the wall of the coronary arteries. A mutation in the MYLK gene has been associated with an increased risk of SCAD in some studies. A VUS is a genetic variation that has been identified in a person’s DNA, but the effect of this variation on an individual’s health is currently unknown or unclear. Further studies and research are needed to determine its significance.
Studies have investigated the relationship between MYLK gene mutations and SCAD and TAAD. In a case report by Majid, et al. a 41-year-old female SCAD patient was found to have mutations in CBS alleles and the MYLK gene [3]. Carss, et al. research involving 384 SCAD patients revealed only one patient with a MYLK gene mutation [4]. Another study by Tarr, et al. of 91 patients found a single patient with a VUS in the MYLK gene [5]. In the research by Zanxin, et al. one patient was identified with MYLK gene mutation out of 99 patients [6]. Marta et al. also found MYLK gene mutation along with other mutations in SCAD patients [7]. Marco, et al. found MYLK mutation in 4 patients with SCAD [8]. In a single family, nine TAAD patients were found to have MYLK gene mutations in a study conducted by Adel, et al [9]. Syeda, et al. has shown that SCAD and TAAD share multiple overlapping genes, including MYLK [10].
These studies suggest that while MYLK gene mutations have been identified in some patients with SCAD or TAAD, they appear to be relatively rare. Further research is needed to fully understand the role of MYLK gene mutations in SCAD and TAAD. It is important to note that the presence of a VUS in the MYLK gene does not necessarily mean that it is the cause of the patient’s aortic dissection, and additional research is required to determine the pathogenicity of this variant.
Conclusion
In conclusion, SCAD is a rare and potentially fatal disorder caused by a tear in a coronary artery wall, resulting in reduced blood flow to the heart. The exact cause is not fully understood, but it may be linked to hormonal changes, physical stress, and connective tissue disorders. Genetic mutations, including those in the MYLK gene, have been identified in some SCAD cases, but their significance remains uncertain. Further research is needed to fully understand the role of MYLK gene mutations in SCAD. Regular follow-up care and awareness of family history are essential for SCAD patients. As research progresses, more insights into the genetic basis of SCAD are expected to improve diagnosis and treatment approaches.
References
-
Saw J, Sedlak T, Ganesh SK, Isserow S, Mancini GBJ (2015) Spontaneous Coronary Artery Dissection (SCAD). Circulation 131(1): e3-e5.
-
Midoun AA, Adlam D, Nabila Naji NB (2021) Recent Advances on the Genetics of Spontaneous Coronary Artery Dissection. Circ Genom Precis Med 14(6): e003393.
-
Asawaeer M, Amor MM, Ahmed M, Prabhu S, Daya HA (2021) Spontaneous Coronary Artery Dissection (Scad): An Increasingly Recognized Cause for Acute Coronary Syndrome. Journal of the American College of Cardiology 77(18_Suppl 1): 2482.
-
Carss KJ, Baranowska AA, Armisen J, Webb TR, Hamby SE, et al. (2020) Spontaneous Coronary Artery Dissection. Circulation: Genomic and Precision Medicine 13(6): e003030.
-
Tarr I, Hesselson S, Iismaa SE, Rath E, Monger S, et al. (2022) Exploring the Genetic Architecture of Spontaneous Coronary Artery Dissection Using Whole- Genome Sequencing. Circ Genom Precis Med 15(4): e003527.
-
Wang Z, Zhuang X, Chen B, Wen J, Peng F, et al. (2020) 99-Case Study of Sporadic Aortic Dissection by Whole Exome Sequencing Indicated Novel Disease-Associated Genes and Variants in Chinese Population. BioMed Research International 2020: 7857043.
-
Prieto ML, Adlam D, Guimaraes MG, Garcia AS, Tome PV, et al. (2021) Differential miRNAs in acute spontaneous coronary artery dissection: Pathophysiological insights from a potential biomarker. eBioMedicine 66: 103338.
-
Antonutti M, Baldan F, Lanera C, Spedicato L, Zanuttini D, et al. (2020) Spontaneous coronary artery dissection: Role of prognostic markers and relationship with genetic analysis, International Journal of Cardiology 326: 19-29.
-
Shalata A, Mahroom M, Milewicz DM, Limin G, Kassum F, et al. (2018) Fatal thoracic aortic aneurysm and dissection in a large family with a novel MYLK gene mutation: delineation of the clinical phenotype. Orphanet J Rare Dis 13(1): 41.
-
Jeoffrey SMHJ, Kalyanasundaram A, Zafar M, Ziganshin BA, Elefteriades JA (2022) Abstract 11587: Intriguing Genetic Overlap between SCAD and TAD. Circulation 146(Suppl_1): A11587.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage