Development of Radiological Models for Three-Dimensional Reconstruction of the Stomach as a Surgical Planning Method in Revisional Bariatric Surgery
It has been shown that three-dimensional radiological reconstruction from CT scan images is very useful in the preoperative planning of complex cases using the patient's preoperative studies. It has been seen to have the most benefit in hepatobiliary and colorectal surgery. Different reconstruction means have been proposed, but all of them are considered validated to plan the critical steps of the intervention. This paper presents our 3D reconstruction model of post-bariatric surgery anatomy, to propose its applicability in revisional surgery. Anatomical models of three-dimensional stomach imaging and post-surgery anatomy have been developed. CT scan images are obtained with the Siemens Somatom Perspective 64equipment. Image recovery is in DICOM format and the processing to achieve three-dimensional reconstruction is done with the OsiriX computer program, performing a complete segmentation of the entire surface to be reconstructed, and a modification of image density. The obtaining of three-dimensional reconstruction images of post-bariatric surgery anatomy allows to develop models that can improve preoperative planning in revision surgery cases, but the risk-benefit of the radiation produced by the CT scan must be assessed to do it systematically.
Introduction
The use of three-dimensional reconstruction technology has represented a significant advance in radiological techniques [1]. Its routine use, along with the already known advances in imaging techniques [1], has improved the diagnoses of many pathologies, and has greatly enhanced the anatomical understanding of certain lesions and all their anatomical relationships [2, 3]. Moreover, in terms of preparation and treatment planning, 3D reconstructions have led to a clear improvement with optimized results, and increased patient safety [2, 3].
The field of hepatobiliary surgery has probably experienced the most evolution as a result of the implementation of 3D technology in preoperative planning, allowing for complete anatomizing of the lesions to be excised, knowing in great detail their location, visceral relationships, and vascular relationships [4, 5]. Real-scale printed models have even been developed from the radiological reconstruction, which allow systematizing the steps of the intervention before it is performed [6, 7]. Colorectal surgery has also experienced a great evolution in the preparation of complex cases, in order to understand the morphology of the different colonic segments, to have a more precise location of the lesions and their anatomical relationships, and a better arrangement of the laparoscopic trocars [8, 9, 10, 11, 12]. Similarly, abdominal wall laparoscopic surgery has been making progress in recent years in the development of techniques, using image processing as a fundamental pillar in this fact [2]. There is less experience in the field of bariatric surgery, where this technology has not been apparently useful in primary surgery [13, 14]. However, with the increase that revisional bariatric surgery is experiencing in recent years, a new path opens in preoperative planning [13, 14]. Cases of failure of vertical gastrectomy due to weight regain, abdominal pain or digestive intolerance due to sleeve stenosis, or the need for resection of the gastrojejunal anastomosis of the bypass due to dysfunction, ulcer or stenosis, can benefit from 3D reconstruction of images. The making of a new gastric tube after resizing calculated according to the existing volumetry, or the making of a new reservoir with anastomosis knowing the initial length of it, either from a previous sleeve or bypass, guarantees more reliable postoperative results [13, 14]. This paper presents the development of 3D anatomical models of post-bariatric surgery anatomy and their application in revisional laparoscopic surgery.
Materials and Methods
The study is limited by the need to have a prior abdominal CT scan, performed as a diagnostic study, either due to complications of their bariatric process or some other diagnostic problem.
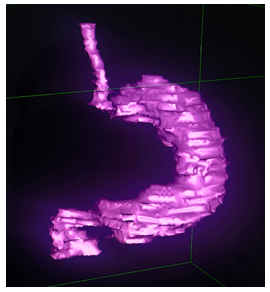
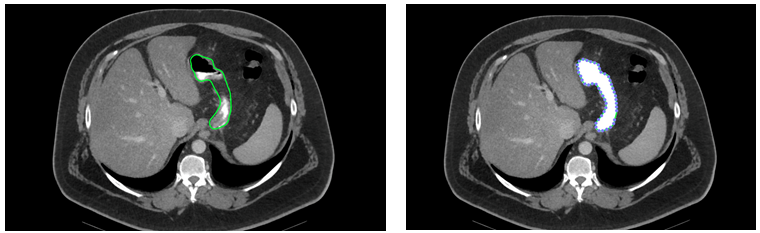
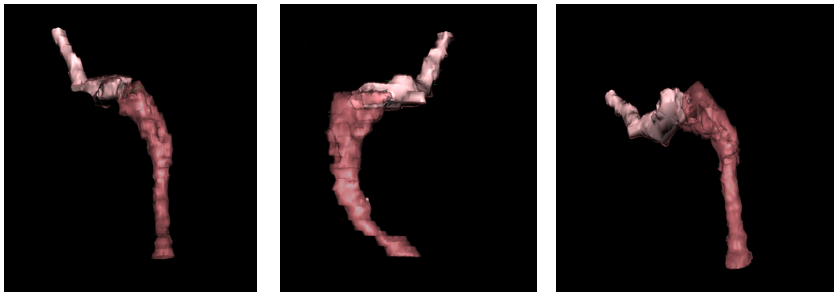
Anatomical models of three-dimensional stomach imaging (Figure 1) and post-surgery anatomy have been developed. CT scan images are obtained with the Siemens Somatom Perspective 64® equipment, with image slices 3 mm thick. Image recovery is in DICOM format and the processing to achieve the three-dimensional reconstruction is performed with the OsiriX® software, performing a complete segmentation of the entire surface (Figure 2) of the esophagus, the stomach, and the first portion of the alimentary loop in the case of the bypass, and a modification of image density [10, 11].
Results
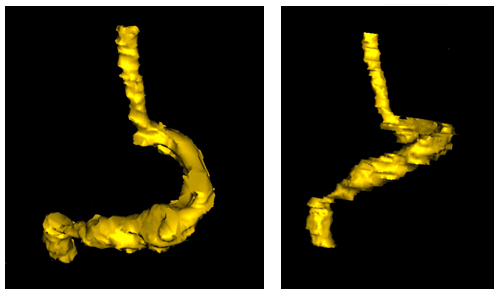
We present the 3D reconstruction models of the post- primary bariatric surgery anatomy of three intervened patients who are candidates for revisional surgery. Case 1: Laparoscopic vertical gastrectomy with sustained abdominal pain without evidence of complication (Figure 3).
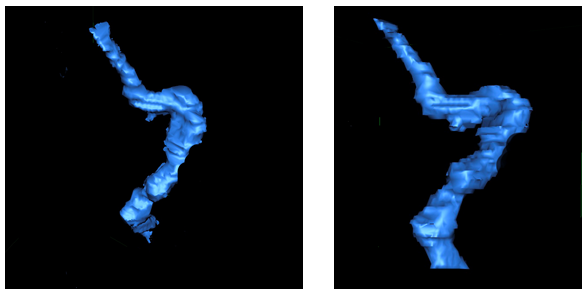
Case 2: Laparoscopic vertical gastrectomy with abdominal pain and digestive intolerance due to partial stenosis of the gastric sleeve (Figure 4). Case 3: Gastrojejunal anastomosis of laparoscopic gastric bypass stenosed due to anastomotic ulcer. The cases were assessed in the preoperative planning of the reintervention (Figure 5).
Discussion
The multidisciplinary approach to complex cases in any field of surgery is essential to ensure a good postoperative outcome [15]. In addition, specifically assessing each situation provides the patient with the security of receiving a completely individualized surgery, which is therefore much more planned and safe [15]. 3D reconstruction technology brings significant benefits in these situations, as it allows for detailed knowledge of anatomical structures, including disposition references, relations with adjacent organs, length, and volumetry, which can be fundamental in surgical planning, especially when it comes to a reintervention [11, 12, 13, 14]. Primary bariatric surgery performed in specialized units achieves excellent results in both weight loss and resolution of comorbidities [16]. The percentage of excess BMI lost achieved by vertical gastrectomy is 68.3%, and by gastric bypass it is 76%. Regarding the resolution of associated comorbidities such as arterial hypertension, sleep apnea syndrome, arthropathies, and hyperuricemia, no statistically significant changes are shown in favor of one procedure or the other 3 or 5 years after surgery [17, 18]. Revision surgery is considered in cases of failure of the primary technique due to poor results in terms of weight loss (regain or insufficient weight loss), recurrence of comorbidities, or the appearance of complications derived from primary surgery, such as abdominal pain, digestive intolerance, anatomical rotation, tube stenosis, anastomotic stenosis, or food retention syndromes [19, 20, 21, 22].
The latest 2018 IFSO survey reports a total of 63,000 revisional surgical procedures reported by 57 societies (9% of the total number of total bariatric procedures, which represents around 700,000 interventions) [22]. Knowing the modified anatomy after the first intervention, through 3-dimensional radiological reconstructions, added to what endoscopic techniques provide, offers the surgeon basic information in order to know in advance the surgical field they will encounter, how to comfortably approach it, what possible complications may arise, and how to anticipate their resolution [14]. Our reconstruction model based on CT scan images, performing manual segmentation of the structures, and a subsequent change in density and color for correct identification, is very useful in pre-surgical planning of cases of revisional bariatric surgery, and can be systematically performed in complex cases, since the time needed to obtain the images is completely acceptable and does not increase the economic cost of the intervention. It allows for the assessment of stenotic or rotated segments in vertical gastrectomy. Similarly, it is feasible to calculate the volume of the gastric reservoir of the bypass for a possible resection of the same, ensuring that enough functional stomach will remain [14]. The risk-benefit ratio of performing a CT scan as a protocol in case of considering revision surgery, and not only in case of complications, should be assessed [23]. The combination of these models with virtual reality technology, and augmented reality, even associated with artificial intelligence methods that should be explored [24, 25], could represent an evolution in the development of simulators and surgical planners, not only for use in clinical practice, but also in training and education [11, 26, 27, 28].
Conclusion
The acquisition of three-dimensional reconstruction images of post-bariatric surgery anatomy allows for the development of anatomical models that can enhance preoperative planning in cases of laparoscopic bariatric revisional surgery. This, in turn, improves the development of surgical reintervention, ensuring more successful postoperative outcomes.
References
-
Siewerdsen JH (2023) Image quality models for 2D and 3D x-ray imaging systems: A perspective vignette. Med Phys 50(1): 109-116.
-
Marconi S, Pugliese L, Botti M, Peri A, Cavazzi E, et al. (2017) Value of 3D printing for the comprehension of surgical anatomy. Surg Endosc 31(10): 4102-4110.
-
Gong X, Pan ZY, Chen J, Yang S, Jiang T, et al. (2021) Application of 3D reconstruction through CT to measure the abdominal cavity volume in the treatment of external abdominal hernia. Hernia 25(4): 971-976.
-
Fang C, An J, Bruno A, Cai X, Fan J, et al. (2020) Consensus recommendations of three-dimensional visualization for diagnosis and management of liver diseases. Hepatol Int 14(4): 437-453.
-
Balci D, Kirimker EO, Raptis DA, Gao Y, Kow AWC (2022) Uses of a dedicated 3D reconstruction software with augmented and mixed reality in planning and performing advanced liver surgery and living donor liver transplantation (with videos). Hepatobiliary Pancreat Dis Int 21(5): 455-461.
-
Perica ER, Sun Z (2018) A systematic review of three- dimensional printing in liver disease. J Digit Imaging 31(5): 692-701.
-
Song C, Min JH, Jeong WK, Kim SH, Heo JS, et al. (2023) Use of individualized 3D-printed models of pancreatic cancer to improve surgeons’ anatomic understanding and surgical planning. Eur Radiol.
-
Bourgouin S, Bège T, Lalonde N, Mancini J, Masson C, et al. (2012) Three-dimensional determination of variability in colon anatomy: applications for numerical modeling of the intestine. J Surg Res 178(1): 172-80.
-
Killeen T, Banerjee S, Vijay V, Al-Dabbagh Z, Francis D, et al. (2010) Magnetic resonance (MR) pelvimetry as a predictor of difficulty in laparoscopic operations for rectal cancer. Surg Endosc 24(12): 2974-2979.
-
Trebolle JF, Escolar JD, Sánchez FM, García VE, Luesma MJ, et al. (2021) 3D morphome- tric analysis of colon applied to a laparoscopic surgical approach. Cadaver study. Actual Med 106(814): 260-270.
-
Trebolle JF, Serrano NP, Benítez CY, Muñoz PM, Bartolomé MJL, et al. (2023) Augmented reality technology applied to surgical planning in oncological colorectal surgery. Clin Radiol Imaging J 7(2): 000204.
-
Romano G, Di Buono G, Galia M, Agnello F, Anania G, et al. (2023) Role of preoperative CT angiography with multimodality imaging reconstruction to perform laparoscopic Complete Mesocolic Excision (CME) and Central Vascular Ligation (CVL) in right-sided colon cancer: Is it really useful? A prospective clinical study. Eur J Surg Oncol 49(1): 209-216.
-
Marie L, Nacache R, Scemama U, Chatta I, Gaborit B, et al. (2018) Preoperative Prediction of Small Bowel Length Using CT Scan and Tridimensional Reconstructions: a New Tool in Bariatric Surgery? Obes Surg 28(5): 1217- 1224.
-
Hanssen A, Sabbag DJ, Hanssen RA, Hanssen DA (2021) 3D CAT Scan and Gastric Volumetry in the Planning of Revisional Bariatric Surgery. J Laparoendosc Adv Surg Tech A.
-
Subramaniam A, Wengritzky R, Skinner S, Shekar K (2022) Colorectal Surgery in Critically Unwell Patients: A Multidisciplinary Approach. Clin Colon Rectal Surg 35(3): 244-260.
-
Pereferrer FS, Domínguez-Adame LE, Ibarzabal A, Macias MS, Azcárate VV, et al. (2017) Quality criteria in bariatric surgery: Consensus review and recom- mendations of the Spanish Association of Surgeons and the Spanish Society of Bariatric Surgery. Cir Esp 95(1): 4-16.
-
Pacheco-Sánchez D, Pinto-Fuentes P, Asensio-Dıáz E (2019) Actualización en Cirugía Bariátrica/Metabó lica. Nutr Clin Med XIII(2): 113-27.
-
Ikramuddin S, Korner J, Lee WJ, Connett JE, Inabnet WB, et al. (2013) Roux-En-Y Gastric Bypass vs Intensive Medical Management for the Control of Type 2 Diabetes, Hypertension, and Hyperlipidemia: The Diabetes Surgery Study Randomized Clinical Trial. JAMA 309(21): 2240-2249.
-
Lo Menzo ES, Szomstein S, Rosenthal RJ (2015) Reoperative bariatric surgery. In: Nguyen NT, et al. (Eds.), The ASMBS Textbook of Bariatric Surgery, New York, pp: 269-282.
-
Mahawar KK, Graham Y, Carr WRJ, Jennings N, Schroeder N, et al. (2015) Revisional Roux-en-Y Gas- tric Bypass and Sleeve Gastrectomy: a Systematic Review of Comparative Outcomes with Respective Primary Procedures. Obes Surg 25(7): 1271-80.
-
Mora Oliver I, Fernández NC, Ballester RA, Ramírez MDC, Serrano JO (2019) Re- visional bariatric surgery due to failure of the initial technique: 25 years of experience in a specialized Unit of Obesity Surgery in Spain. Cir Esp 97(10): 568-74.
-
Frutos MD, López A, Sabench F, Vives M (2022) Cirugía bariátrica de revisión. Monografías de la AEC, Nº13. Asociación Española de Cirujanos. Madrid. Spain.
-
Albert JM (2013) Radiation risk from CT: implications for cancer screening. AJR Am J Roentgenol 201(1): W81- 7.
-
Wichmann JL, Willemink MJ, De Cecco CN (2020) Artificial Intelligence and Machine Learning in Radiology: Current State and Considerations for Routine Clinical Implementation. Invest Radiol (9): 619-627.
-
Bhayana R, Bleakney RR, Krishna S (2023) GPT-4 in Radiology: Improvements in Advanced Reasoning. Radiology 307(5): e230987.
-
Bailer R, Martin RCG (2019) The effectiveness of using 3D reconstruction software for surgery to augment surgical education. Am J Surg 218(5): 1016-1021.
-
Izard SG, Juanes JA, Peñalvo FJG, Estella JMG, Ledesma MJS, et al. (2018) Virtual Reality as an Educational and Training Tool for Medicine. J Med Syst 42(3): 50.
-
Rizzetto F, Bernareggi A, Rantas S, Vanzulli A, Vertemati M, et al. (2020) Immersive Virtual Reality in surgery and medical education: Diving into the future. Am J Surg 220(4): 856-857.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage