Pulmonary Mucormycosis: A Case Report
Mucormycosis an opportunistic mycosis, has emerged as a significant concern among severely immune compromised individuals, particularly those with hematologic malignancies or those who have undergone stem cell or organ transplantation. In this case report, we present a rare case of pulmonary mucormycosis complicated by abscess formation in a middle-aged male with a medical history of Acute Myeloid Leukemia (AML). The imaging findings revealed a non-specific fungal infection, and the pathology report confirmed the diagnosis of pulmonary mucormycosis. Subsequently, the patient underwent a successful left upper lobectomy and is currently in a stable condition.
Introduction
Mucormycosis is a condition that results from an infection caused by fungi belonging to the order of Mucorales. The primary mode of transmission to humans is through inhalation of sporangiospores, although it can also occur through ingestion of contaminated food or traumatic inoculation [1, 2]. Mucorales fungi are ubiquitous and display broad, ribbon-like hyphae morphology that is mostly aseptate or sparsely septate. Human infections can be caused by around 27 species and 11 genera of Mucorales fungi. Among these, Rhizopus arrhizus is the most prevalent causative agent of mucormycosis worldwide, followed by Lichtheimia, Apophysomyces, Rhizomucor, Mucor, and Cunninghamella species [3, 4]. While most filamentous fungi tend to affect individuals with weakened immune systems, such as cancer patients, transplant recipients, and those with inherited immune deficiencies, mucormycosis can also be a potentially fatal infection in individuals with greater immune competency. These include people with diabetes mellitus, those receiving deferoxamine therapy, injection drug users, and those without any apparent immune impairment. [4]. The rhino-cerebral variant of mucormycosis tends to be observed more frequently in individuals with diabetes mellitus, while pulmonary mucormycosis is an infrequent manifestation in patients with hematological malignancies and those who have received organ transplants [5, 6]. Here we present a case of pulmonary Mucormycosis.
A 50-year-old patient was admitted to the hospital for a COVID-19 infection complicated by pseudomonas bacteremia. He has a history of cocaine abuse, heavy smoking, and frequent marijuana use. An infectious workup was sent upon admission, and blood cultures were positive for Pseudomonas. Treatment with Zosyn was initiated. The patient was found to be pancytopenic, and therefore underwent a bone marrow biopsy three days after admission, which revealed results consistent with Acute Myeloid Leukemia (AML). The following day, the medication was changed to Ciprofloxacin. Four days later, the patient experienced a new neutropenic fever, and a chest x-ray was ordered, revealing a new opacity in the left upper lobe. Two days later, the patient experienced worsening chest pain. A CT angiography was obtained, and the findings were concerning for fungal pneumonia (Figure 1).
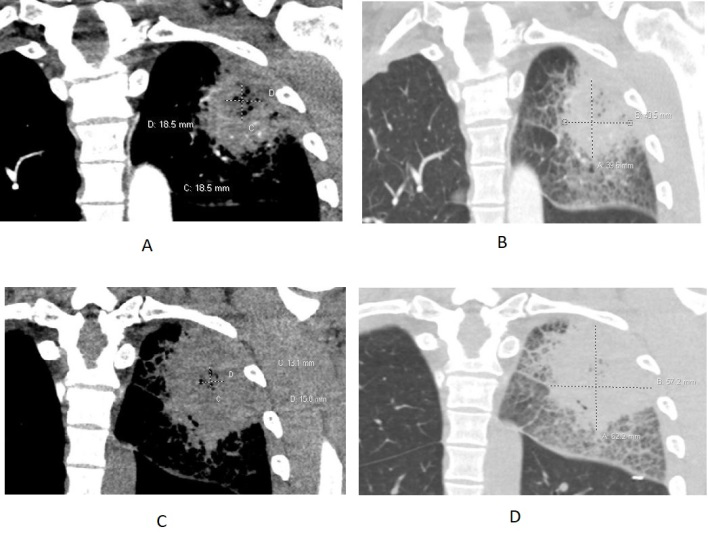
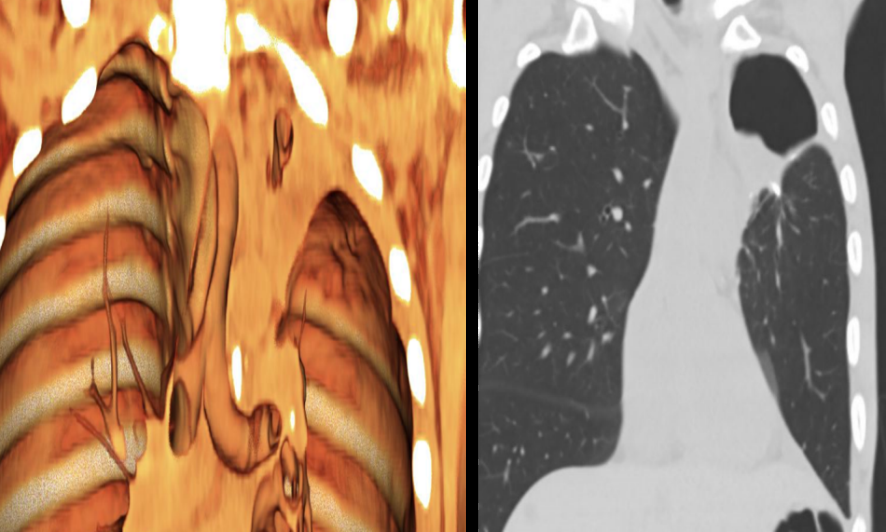
Figure 1: CT chest with coronal reformat at first day of admission (A and B) revealed left upper lobe (LUL) consolidative opacity measures 4.1x4.0 cm with a central area of heterogeneous gas density measures 1.9x1.9 cm. Mild surrounding ground glass and septal thickening. Four days later, Interval increase of LUL opacity (C and D) measures 6.2x5.7 cm and central heterogeneous gas density measures 1.6x1.3 cm. interval increase of surrounding septal thickening and ground glass densities.
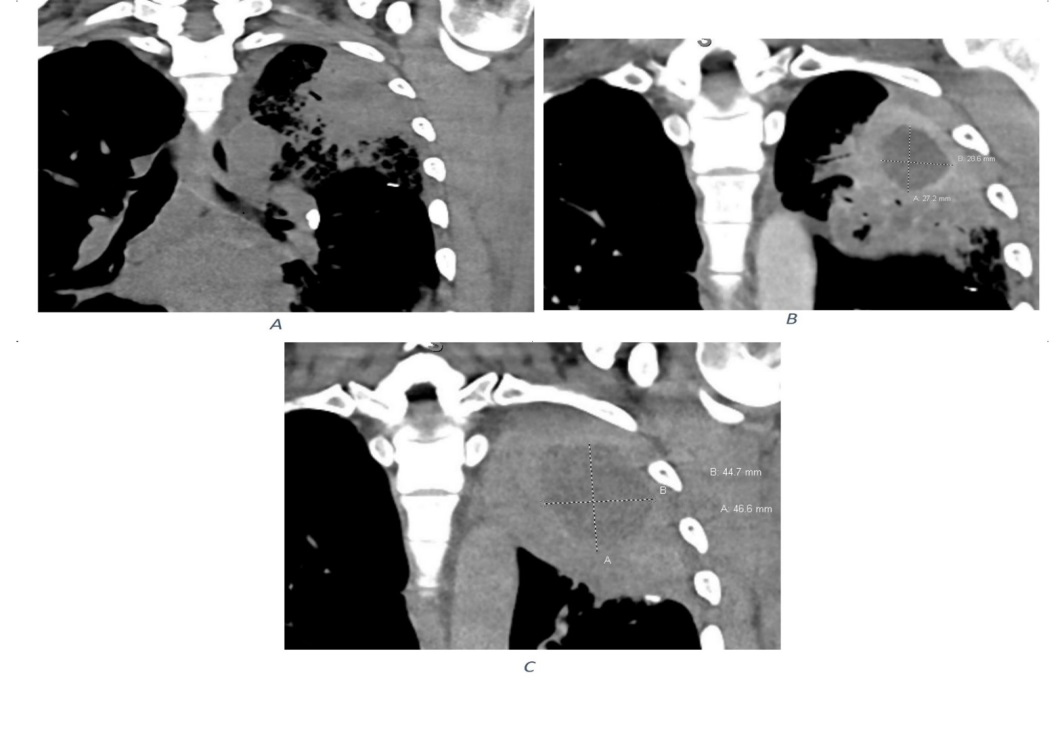
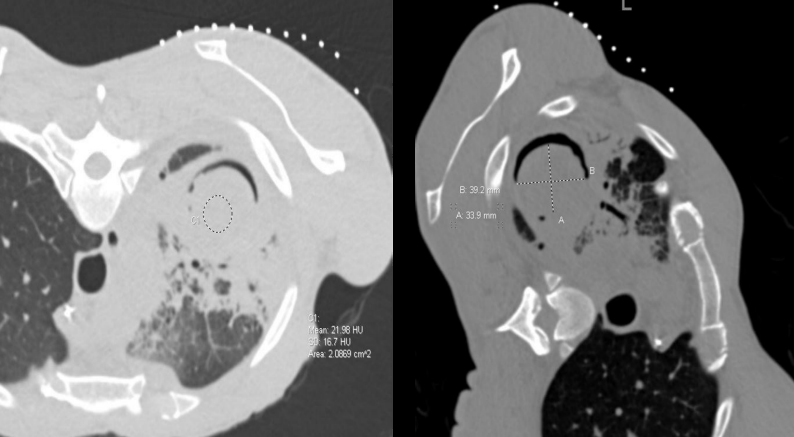
The infectious disease team was consulted, and the medication was changed back to Zosyn, and Posaconazole was started for possible fungal pneumonia. After three days of medication change, a CT sinus was ordered for sinus complaints in the setting of possible fungal pneumonia, which was consistent with worsening sinusitis. On the following day, an MRI of the orbits and facial bones was obtained, which was consistent with probable bacterial/ viral sinusitis. On the same day, a repeat CT chest was obtained, and the findings were concerning for worsening fungal pneumonia. On the next day, Posaconazole was discontinued, and Amphotericin B was initiated based on the recommendations of the infectious disease team. Two days later, the patient started induction chemotherapy with 7+3 Idarubicin, which consists of 3 days of Idarubicin 20mg IV and 7 days of Cytarabine 167mg IV. Three days after starting chemotherapy, a repeat CT chest was ordered, which was consistent with unchanged pneumonia. After seven days, Vancomycin was added to the patient’s regimen. Two days later, a CT chest/abdomen/pelvis was obtained due to persistent fever, and the results were consistent with left upper lobe fluid collection with surrounding pneumonia. The patient was diagnosed with a lung abscess secondary to necrotizing pneumonia (Figure 2). The patient underwent bone marrow biopsy two weeks after admission, which was negative for residual AML. The patient was restarted on Amphotericin B and underwent a repeat bronchoscopy. One day later, the patient was started on Granix. Three days later, a repeat CT chest was obtained, and it was consistent with worsening pneumonia and infection. Amphotericin B was discontinued, and Posaconazole was resumed per infectious disease recommendations. After three days, Zosyn was broadened to Meropenem for persistent fever. Two days later, Vancomycin was discontinued, and the patient resumed Amphotericin for persistent fevers and concern for fungal abscess. Three days later, the patient obtained a repeat CT chest, which was consistent with a persistent abscess in the left upper lobe. After six days, a diagnostic radiology consultation was conducted for CT-guided drainage of the lung abscess, and the procedure was scheduled two days later. However, during a repeat CT scan, the air in a cavity was observed, which could not be drained as a mycetoma/ fungal ball had formed (Figure 3). Additionally, a CT sinus showed a decrease in sinus opacification, with residual mucosal thickening. The patient was referred to a thoracic surgery team for evaluation of surgical intervention as their lung condition was not responding to medical management, and their blood counts had recovered. Pulmonary function tests were ordered and are pending.
The patient underwent a bronchoscopy with a biopsy with a pulmonary specialist. The culture results from the bronchoalveolar lavage (BAL) showed a positive test for Stenotrophomonas maltophilia. The patient underwent a bone marrow biopsy three days after the bronchoscopy, and the results showed no morphologic or immunophenotypic evidence of AML. Two days later, intravenous antibiotics were discontinued, and the patient remained afebrile and stable. After two days, the patient was discharged home with treatment of Posaconazole.
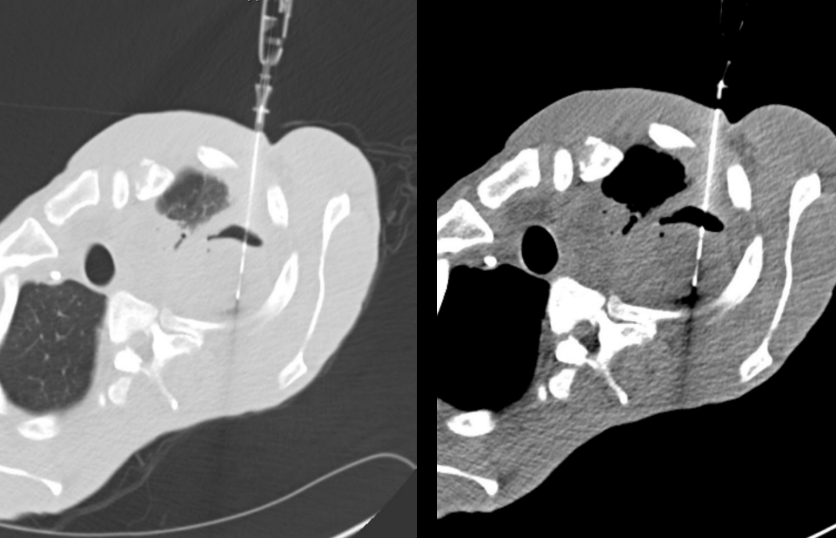
After two weeks, the patient exhibited a substantial clinical deterioration and was readmitted for an evaluation of pulmonary infection progression. A CT chest was performed, which revealed new lesions. The Interventional radiology (IR) team was consulted for a CT-guided biopsy of the left upper lobe (LUL) nodule (Figure 4). The pathological findings were indicative of Mucorales species (Figure 5). Accordingly, Amphotericin B was commenced immediately, as per the infectious disease (ID) recommendations. The thoracic surgery team reviewed the case for potential resection; however, due to the patient’s poor pulmonary function tests (PFTs) and high mortality risk, continued medical management was advised. Micafungin was added after infectious disease (ID) team recommendations. After 3 days, a repeat CT chest was obtained, which showed worsening pneumonia. Vancomycin was discontinued on the following day. Three days later, the patient’s pulmonary function tests (PFTs) were repeated, and it was observed that the patient had improved. A bone marrow biopsy and aspiration were performed on the same day, and the results showed no evidence of acute myeloid leukemia (AML). Two days later, a ventilation-perfusion (VQ) scan was obtained, which revealed that the patient had 33% perfusion to the left lung and 67% perfusion to the right lung. After 6 days, the patient underwent a left upper lobectomy (Figure 6) and was transferred to the Cardiothoracic Surgery (CTS) service following the procedure. After two days, the patient was transferred back to the hematology service with a chest tube to water seal. The chest tube was clamped after four days with good tolerance. A repeat CT chest revealed improvement in the right upper lobe (RUL) nodules and the chest tube was removed with good tolerance. Micafungin was discontinued one day after removing the chest tube. Five days later, the patient started maintenance Onureg (PO azacitidine) and completed a 14-day course. The current plan for the patient is to receive six weeks of daily Amphotericin after lobectomy followed by 4-6 weeks of Amphotericin three times per week.
![Figure 5: Biopsies from the lung (Hematoxylin & eosin-stained sections A [magnification x40] and B [magnification x400]) revealed extensive necrotic lung parenchyma (black arrow) involved by numerous broad aseptate fungal hyphae (red arrows), morphologically consistent with mucormycosis.](/fulltextimages/10772/fig_5.png)
Discussion
Mucormycosis, an opportunistic mycosis, has gained significance in severely immunocompromised individuals with hematologic malignancies or those who have undergone stem cell or organ transplantation. The term zygomycosis, previously used for infections caused by fungi belonging to the Mucorales order, is no longer suitable after a recent taxonomic reclassification eliminated Zygomycetes as a class [7, 8]. Sinopulmonary mucormycosis is the predominant form of infection caused by Mucorales species in individuals with severe immune compromise. The epidemiology of pulmonary mucormycosis is changing, with more instances of breakthrough infections being reported in leukemia and transplant patients who are being treated with Aspergillus- active drugs that do not have anti-Mucorales activity [9, 10]. Mucorales, as compared to other opportunistic molds, have a broader range of hosts, including immunocompetent individuals. Different forms of mucormycosis are more prevalent in hosts with specific immune defects, such as diabetic ketoacidosis predisposing individuals to rhinocerebral mucormycosis. Severely immunocompromised individuals, including patients with high-risk hematologic malignancies and recipients of hematopoietic stem cell and organ transplants, are more likely to develop pulmonary mucormycosis due to chemotherapy-related defects in innate pulmonary host defenses associated with neutropenia or chemotherapy-induced mucociliary dysfunction. Prolonged and severe neutropenia is the sole identifying risk factor in approximately 15% of all reported mucormycosis cases [10]. Pulmonary mucormycosis starts with inhaled conidia that can remain localized in the lungs or spread through the bloodstream. In healthy individuals, phagocytes can eliminate fungal spores and hyphae through various killing mechanisms [11]. Defects in phagocytic cell activity, whether quantitative (e.g. neutropenia) or qualitative (e.g. associated with glucocorticoids, hyperglycemia, or acidosis), can lead to uncontrolled growth of the hyphal form and invasive infection. Hyperglycemia and acidosis can impair phagocytic cells’ activity to kill Mucorales through oxidative and nonoxidative mechanisms. Similarly, corticosteroids can impede migration, ingestion, and phagolysosome fusion in macrophages [12]. In recent years, mucormycosis has emerged as a growing concern, particularly for patients with weakened immune systems. It is still frequently misdiagnosed in clinical settings due to its nonspecific symptoms, often leading to prolonged treatment and delayed management of the infection. The clinical presentation of pulmonary mucormycosis is often vague and unspecific, even in advanced stages of the disease. Patients may experience a range of symptoms, such as refractory fever, a nonproductive cough, progressive dyspnea, and pleuritic chest pain. Furthermore, concurrent sinusitis and pulmonary disease may further complicate diagnosis and management [13]. Rhinocerebral Mucormycosis presents as unilateral facial symptoms such as pain, headache, fever, hyposmia, and congestion. The condition rapidly progresses to black discharge, followed by invasion of orbital nerves and vessels, causing vision loss, nasal cavity and face necrosis, and brain involvement leading to unconsciousness and poor prognosis [14]. Chest radiography usually shows lobar and segmental consolidation in patients with the infection, which can spread to the opposite lung if untreated. On CT, a ground-glass lesion around the blood vessels is a common early finding, which can progress to nodules or masses. The reversed halo sign, which represents a central area of ground glass opacity surrounded by a rim of consolidation, has been identified as a fairly specific sign that can suggest a diagnosis of fungal lung infection in the appropriate clinical context.
The fungus can invade the blood vessels and cause necrosis, which leads to consolidation and masses with a lack of air bronchograms.
Cavitations may also appear on imaging, cavitations represent tissue infarct and destruction and it appear as well-defined mass with air fluid level or necrotic debris surrounded by consolidation. Air-crescent signs can also be observed in patients with centrally located lesions. It’s worth noting that the presence of air-crescent sign is associated with an increased risk of pulmonary artery erosion and the potential for experiencing massive hemoptysis. However, several studies have linked the air-crescent sign to the recovery of neutropenia. Pseudoaneurysms and vascular cutoff signs are other vascular findings. Pleural thickening or effusion indicates pleural infection, while air in intercostal space or subcutaneous soft tissues suggests chest wall spread [15]. The clinical and radiological presentations of invasive pulmonary aspergillosis and pulmonary mucormycosis overlap with each other. Diagnosis of pulmonary mucormycosis may be supported by the presence of multiple nodules (≥10) and, to a lesser extent, pleural effusions. Additionally, it has been suggested that the reverse-halo sign could be a more frequent early radiographic finding in patients with pulmonary mucormycosis compared to aspergillosis. A fungus ball is formed by a mass inside an existing cavity. CT imaging can reveal the presence of a cavity with a fungal ball within it, which may change position and become dependent on a prone scan. The fungal ball consists of fungal hyphae mixed with air and minerals, giving it high attenuation on CT. The presence of fungal strands bridging the fungal ball and the cavity wall is a specific characteristic of aspergilloma [16]. Diagnosing mucormycosis requires a high level of suspicion and is largely dependent on the identification of hyphae invading the tissues, which often requires an invasive procedure. Although cultures from tissue swabs, sputum, or bronchial alveolar lavage may not be definitive, they can provide important indications of disease in immunocompromised patients. Bronchoscopic or percutaneous lung biopsy are effective diagnostic tools for pulmonary mucormycosis.
While it may not be widely accessible, quantitative polymerase chain reaction (qPCR) has proven to be an effective method for detecting mucormycosis by demonstrating circulating Mucorales DNA in various patients [17]. Mucormycosis treatment involves a combination of surgical debridement and antifungal therapy to eliminate infected tissues and underlying predisposing factors. The first-line therapy is intravenous amphotericin B (a lipid formulation), with posaconazole or isavuconazole used as step-down or salvage therapy. Surgery is recommended for patients with localized disease, particularly those with unifocal disease, and can include wedge resection, lobectomy, or pneumonectomy. Surgery in combination with antifungal therapy has been shown to improve outcomes compared to antifungal therapy alone [18].
Conclusion
Pulmonary mucormycosis is an uncommon fungal infection that primarily affects patients with hematological malignancies. The clinical presentation and radiological features are nonspecific, making it challenging to diagnose even in advanced stages of the disease. As a result, it is frequently misdiagnosed, leading to prolonged treatment and delayed management of the infection. Therefore, a high level of suspicion is necessary for an accurate diagnosis. Bronchoscopic or percutaneous lung biopsy are effective diagnostic tools for confirming pulmonary mucormycosis.
Patient consent
An informed consent and permission were obtained from the patient.
References
-
Richardson M (2009) The ecology of the Zygomycetes and its impact on environmental exposure. Clin Microbiol Infect 15 Suppl 5: 2-9.
-
Dam P, Cardoso MH, Mandal S, Franco OL, Sagiroglu P, et al. (2023) Surge of mucormycosis during the COVID-19 pandemic. Travel Med Infect Dis 52: 102557.
-
Jeong W, Keighley C, Wolfe R, Lee WL, Slavin MA, et al. (2019) The epidemiology and clinical manifestations of mucormycosis: a systematic review and meta-analysis of case reports. Clin Microbiol Infect 25(1): 26-34.
-
Roden MM, Zaoutis TE, Buchanan WL, Knudsen TA, Sarkisova TA, et al (2005) Epidemiology and outcome of zygomycosis: a review of 929 reported cases. Clin Infect Dis 41(5): 634-653.
-
Skiada A, Floerl CL, Klimko N, Ibrahim A, Roilides E, et al. (2018) Challenges in the diagnosis and treatment of mucormycosis. Med Mycol 56(suppl_1): 93-101.
-
Azhar A, Khan WH, Khan PA, Alhosaini K, Owais M, et al. (2022) Mucormycosis and COVID-19 pandemic: Clinical and diagnostic approach. J Infect Public Health 15(4): 466-479.
-
Spellberg B, Edwards J, Ibrahim A (2005) Novel perspectives on mucormycosis: pathophysiology, presentation, and management. Clin Microbiol Rev 18(3): 556-569.
-
Hibbett DS, Binder M, Bischoff JF, Blackwell M, Cannon PF, et al. (2007) A higher-level phylogenetic classification of the Fungi. Mycol Res 111(Pt 5): 509-547.
-
Pappas PG, Alexander BD, Andes DR, Hadley S, Kauffman CA, et, al. (2010) Invasive fungal infections among organ transplant recipients: results of the Transplant- Associated Infection Surveillance Network (TRANSNET). Clin Infect Dis 50(8): 1101-1011.
-
Hamilos G, Samonis G, Kontoyiannis DP (2011) Pulmonary mucormycosis. Semin Respir Crit Care Med 32(6): 693-702.
-
Kontoyiannis DP, Lewis RE (2006) Invasive zygomycosis: update on pathogenesis, clinical manifestations, and management. Infect Dis Clin North Am 20(3): 581-607.
-
Krishna V, Bansal N, Morjaria J, Kaul S (2006) COVID-19- Associated Pulmonary Mucormycosis. J Fungi (Basel) 8(7).
-
Espana JDA, Voigt K (2022) Mini Review: Risk Assessment, Clinical Manifestation, Prediction, and Prognosis of Mucormycosis: Implications for Pathogen- and Human-Derived Biomarkers. Front Microbiol 13: 895989.
-
Agrawal R, Yeldandi A, Savas H, Parekh ND, Lombardi PJ, et al. (2020) Pulmonary Mucormycosis: Risk Factors, Radiologic Findings, and Pathologic Correlation. Radiographics 40(3): 656-666.
-
Nam BD, Kim TJ, Lee KS, Kim TS, Han J, et al. (2018) Pulmonary mucormycosis: serial morphologic changes on computed tomography correlate with clinical and pathologic findings. Eur Radiol 28(2): 788-795.
-
Prasad A, Agarwal K, Deepak D, Atwal SS (2016) Pulmonary Aspergillosis: What CT can Offer Before it is too Late. J Clin Diagn Res 10(4).
-
Cox G, Kauffman C, Thorner A (2018) Mucormycosis.
-
Smith C, Lee SC (2022) Current treatments against mucormycosis and future directions. PLoS Pathog 18(10): e1010858.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage