Assessment of Relationship between Clinical Manifestation of Chiari Malformation Type I and Volumetric Measurement of Cerebellar Tonsils Herniation within Foramen Magnum
Introduction: Chiari malformation type I (CMI) is diagnosis based on clinical and radiological measurement of cerebellar tonsils herniation of 5mm or more below the foramen magnum (FM). The aim of the study was to determine the relationship between clinical presentation of CMI and cerebellar tonsils herniation measured in 3dimensions (3D), cerebellar tonsils volume and T/F volume ratio (cerebellar tonsils volume/foramen magnum). Methods: The study included 96 patients with CMI based on study sample size and power calculation.3D measurement of cerebellar tonsils was made, the volume of cerebellar tonsils was calculated using ellipsoid volume formula. The transverse diameter of FM measured and the volume of FM calculated using sphere formula. We computed non-parametric statistical tests and hypothesis testing to analyze correlation and variation of cerebellar tonsils measurements, cerebellar tonsils volume, and T/F volume ratio in relation to severity of myelopathy using mJOA (modified Japanese Orthopedics association) score and headache severity using NRS (Numerical Rate Score). Results: The finding showed a correlation between myelopathy severity and the volume of herniated cerebellar tonsils as well as correlation between myelopathy severity and T/F volume ratio (Cerebellar tonsil volume/Foramen magnum volume). There was also correlation between headache severity and cerebellar tonsil volume as well as T/F volume ratio. Conclusion: Consideration of both clinical presentation and radiological measurement in assessment of CMI is crucial, rather than considering only cut off of 5 mm descent of cerebellar tonsils herniation in midsaggital view. Cerebellar tonsils volume and T/F volume ratio are the indicators of severity of myelopathy and headache severity as shown in the study.
Background
The description of CMI was initially based on pathological and anatomical anomaly related to the cerebellar tonsils [1]. Based on anatomical definition; CMI is characterized by hindbrain deformity and elongation of the cerebellar tonsils resulting into their descent into the foramen magnum. The classic definition of CMI is radiological and is defined as herniation of the cerebellar tonsils below the foramen magnum of >3 mm in children and> 5 mm in adults [2]. There are questions about the most accurate radiological criteria to diagnose CMI which remain unanswered. Is CMI a sagittal disease? should we only rely on the cut off descent of cerebellar tonsils of 5mm below foramen magnum in sagittal plane in diagnosis of CMI ? Can the descent of cerebellar tonsils in coronal plane reflect the severity of CMI? Can the volume of cerebellar tonsils herniation reflect better the severity of CMI? Can T/F volume ratio (Cerebellar tonsil volume/Foramen magnum volume) reflect better the severity of CMI patients?
Research Methodology
Research Ethics Approval
This study was presented and approved by the Institutional Review Board (IRB) of the College of Medicine and Health Sciences of University of Rwanda with reference number CMHS/IRB/344/2020.
Study Design
The study included 96 patients based on sample size and power calculation This study was conducted in 3 major referral hospitals in Rwanda, King Faisal Hospital (KFH), University Teaching Hospital of Kigali (CHUK) and Rwanda Military Hospital(RMH). We conducted a prospective observational cross sectional analytical study. Patients with clinical and radiological confirmation of CMI was enrolled based on most common clinical findings in patients with CMI; clinical inclusion criteria was at least patients presenting with occipital headache, neck pain, dizziness, limb paraesthesia and increased deep tendon reflex 3+ on physical exam. Cerebellar tonsils herniation at the level of foramen magnum measured in sagittal, coronal and axial planes reflecting respectively the length, height and width of the herniated cerebellar tonsils using cranio-cervical MRI was measured.
Cerebellar tonsils considered to be ellipsoid shape and its volume was calculated based on the following formula: volume =𝑙𝑒𝑛𝑔ℎ𝑡∗ℎ𝑒𝑖𝑔ℎ𝑡∗𝑤𝑖𝑑ℎ𝑡∗0.52 (Adopted from radiological calculation of prostate volume and prostate ellipsoid formula) [3, 4]. The most inlet of the foramen magnum which is the inner diameter of opisthion-basion plane was used as reference point for the above mentioned measurements. FM was considered to be an ovoid shape as state in other literature and it’s volume was calculated as follow: 𝑉=4/3𝜋𝑟3 (Figures 1-3).
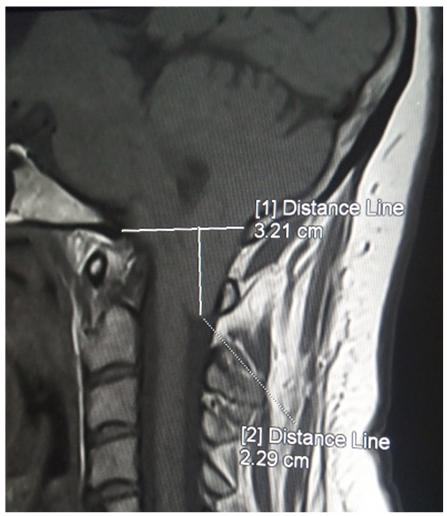
Saggital View
- Distance Line: McRae line measuring the distance from opisthion to basion, corresponding to the transverse diameter of foramen magnum.
- Distance line: Perpendicular line to distance line 1 measuring cerebellar tonsil in sagittal plane. Figure 1: C spine MRI image showing sagittal measurement of cerebellar tonsil.
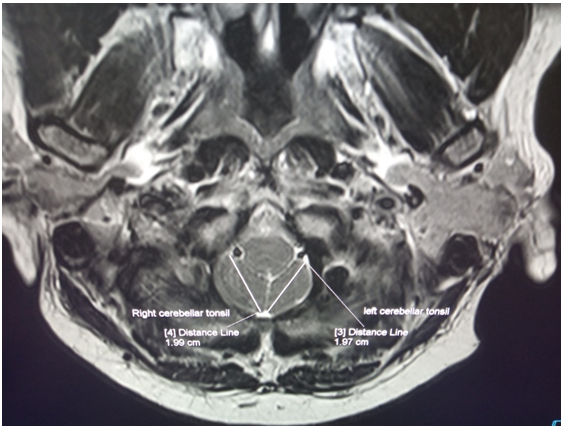
Axial View
- Distance line: The longest length of the left cerebellar tonsil measured in axial plane.
- Distance line: The longest length of the right cerebellar tonsil measured in axial plane. Figure 2: C spine MRI image showing measurement of the longest length of cerebellar tonsils in axial plane.
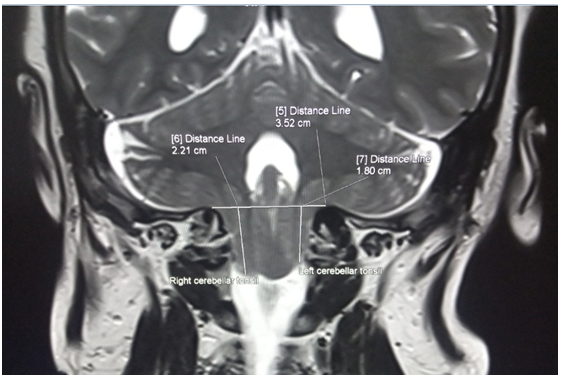
Coronal Plane
- Distance line: The most upper inlet of the foramen magnum in coronal plane.
- Distance line: Perpendicular line to distance line 5 measuring the right cerebellar tonsil in coronal plane. Figure 3: C spine MRI image showing measurement of the longest length of cerebellar tonsils in coronal plane.
Data Management and Statistical Analysis
To assess the relationship between clinical manifestation of CMI and cerebellar tonsils, we computed various non- parametric statistical tests and hypothesis testing to analyze correlation and variation of cerebellar tonsils measurement in sagittal, coronal and axial planes, cerebellar tonsils volume, and the T/F volume ratio (cerebellar tonsils volume/ foramen magnum volume).
We run Spearman Rank correlation test to analyze correlation between headache severity and both sagittal and coronal measurements (right and left), correlation between total cerebellar tonsils volume and foramen magnum, correlation between cerebellar tonsils volume and headache severity, myelopathy severity and tonsils volume, and T/F volume ratio and myelopathy. The hypothesis tests using Wilcoxon rank sum tests was also constructed to assess the significance of variation between right and left cerebellar tonsils measurements (coronal and sagittal measurements) in diagnosis of CMI, cerebellar volume (left and right), and sagittal and coronal measurements. We computed descriptive analysis to determine demographic characteristics of the study participants, occurrence of signs and symptoms among patients with CMI. Before running every test, we assessed the skewness of the data by variable and made a log-transformation whenever suitable likely, we found none. When we found that the data were skewed, we went on running and look for suitable non-parametric tests. We did all the calculations in Python 3 using scipy. Stats, Wilcoxon, Pearsonr, Seaborn and Matplotlib, pyplot Packages and Panda library.
Results
The study included 96 patients based on calculated sample size and statistical power of the study. CMI was most common in female with male to female ratio of 1:1.5. The majority of patients with CMI in our study was in fourth and fifth decade with age ranges: less than 20 years of age, between 20-30 years of age ,between 40-50 years of age and above 50 years representing 7.3%, 12.5%, 39.6%, 32.3% and 8.3% respectively.
Myelopathy followed by sensory loss was the common finding .Upper motor neuron lesion like Hoffman sign, spasticity and clonus was found to be 8% and 18% respectively. The motor weakness as result of CMI was found in 15% of the study population. Scoliosis as result of CMI was found in 5% while syringomyelia was found in 8% in study population.
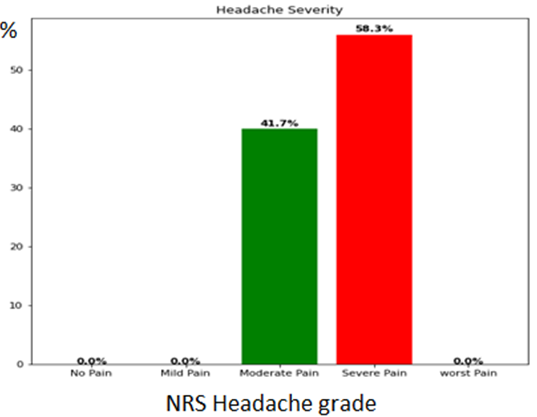
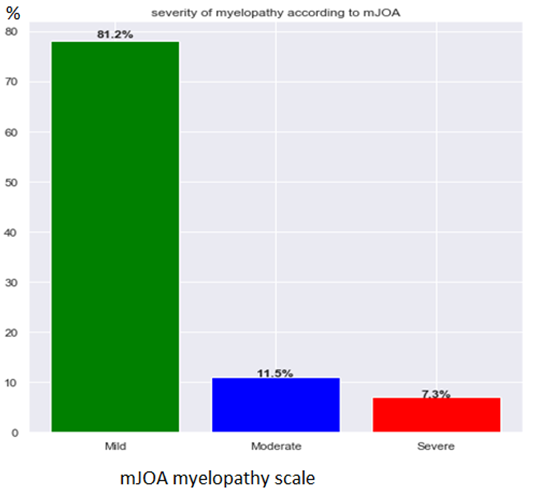
Headache and myelopathy severity was graded according to NRS and mJOA respectively. Patients with CMI mostly presented with severe headache, moderate headache with 58.3% and 41.7% respectively according to pain NRS scale in the study. The severity of myelopathy was classified into mild, moderate and severe according to mJOA. Most patients with CMI was mild myelopathic with 81.2% followed by moderate myelopathy with 11.5 % and severe myelopathy in 7.3% of study subjects (Figures 4 & 5).
| Coronal (mm) | Median(IQR) | Sagittal (mm) | Median(IQR) |
|---|---|---|---|
| left | 11.2(9.3 13.1) | Left | 7.8(6.2 10.4) |
| right | 11.4(10.2 14.1) | Right | 8.8(7.2 11.3) |
| Transverse Diameter of Foramen magnum Median (IQR)mm | |||
| 38.35(36.2 40.63) | |||
| Foramen Magnum volume Median (IQR)mm3 | |||
| 29,517.3(24,774.6 35,088.1)mm3 | |||
| Cerebellar tonsils volume Median (IQR) | |||
| 2,427.61(1,706.01 3,625.2)mm3 | |||
| T/F volume ratio (Cerebellar tonsils volume/FM volume) Median (IQR) | |||
| 0.082(0.053 0.177) |
Table 1: Radiological Measurement of Foramen Magnum and Cerebellar Tonsils.
The measurement of herniated cerebellar tonsils was done in 3D; coronal measurement, sagittal measurement, axial measurement and volume of herniated cerebellar tonsils were calculated.
The diameter of FM was measured and the volume of FM calculated using sphere formula and transverse diameter of FM diameter respectively. The findings are the following:
- The left median coronal measurement was 11.2 mm with interquatile (IQR) range (9.3 mm- 13.1 mm).
- The right median coronal measurement was 11.4 mm with interquatile range of (10.3 mm-14.1mm).
- The left median sagittal measurement was 7.8 mm with interquatile range of (6.2 mm -10.4mm).
- The right median sagittal measurement was 8.8 mm with interquatile range of (7.2mm-11.3mm).
- The median transverse diameter of FM was 38.25 mm with interquatile range of (36.2mm-40.63mm).
- The median volume of foramen magnum was 29,571.3 mm3 with interquartile range of (24,774.6mm- 35,088.1mm).
- The median of total cerebellar tonsils volume was 2,427.61mm3 with interquartile range of (1,706.01mm3 - 3,625.2mm3).
- The median and interquartile range of T/F volume ratio (cerebellar tonsils volume/FM volume) was 0.082(0.053 0.177) respectively.
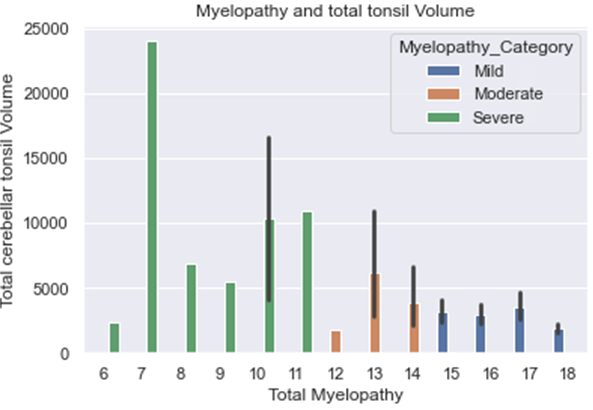
There was a relationship between myelopathy severity and the volume of herniated cerebellar tonsils as well as the relationship between T/F volume ratio and myelopathy severity according to mJOA; there was also a correlation between myelopathy severity and the volume of herniated cerebellar tonsils. The more patient had an increase of volume of herniated cerebellar tonsils, the more the severity of myelopathy on mJOA scale (Figure 6).
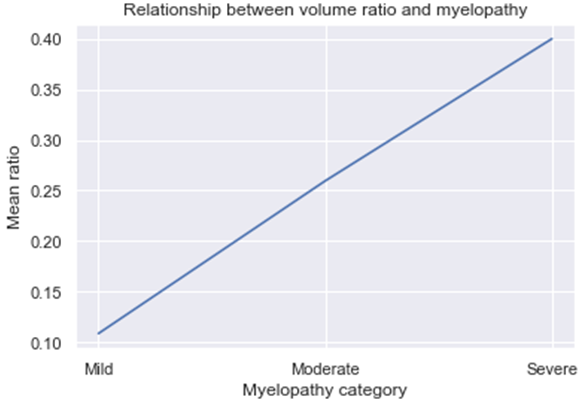
There was a crescendo relationship between T/F volume ratio (cerebellar tonsils volume/Foramen magnum volume) and severity of myelopathy. The increase of volume ratio is proportional to the severity of myelopathy on mJOA scale (Figure 7).
Discussion
The majority of patient with CMI in our study was in fourth and fifth decade with age ranges: less than 20 years of age, between 20-30 years of age, between 40-50 years of age and above 50 years representing 7.3%, 12.5%, 39.6%, 32.3% and 8.3 % respectively. Aska Arnautovic and colleagues in their review of study on demographics, operative treatment and outcome showed that peak age of presentation in the pediatric studies were 8 years, followed by 9 years, and in the adult series,41 years, followed by 46 years old with female to male ratio 1.3:1 [5]. James R Houston, et al. in their study on evidence for sex difference in morphological abnormality in CMI report no sex difference of morphometric abnormalities of CMI malformation [6].
Patients with CMI mostly presented with severe headache and moderate headache with 58.3% and 41.7 % respectively according to pain numeric rating scale in our study. There was no correlation between headache severity and cerebellar descent measurement in both sagittal and coronal. In contrast there was proportional correlation between headache severity and T/F volume ratio (cerebellar tonsils volume/ foramen magnum volume ratio). The study by Heffez DS, et al. [7] reported that there is no correlation between symptoms severity with extent of cerebellar descent in CMI patients [7].
Jonathan Pindrik, et al. in their study on clinical presentation of CMI and syringomyelia in pediatric population report headache or neck pain in 27%-70%, motor or sensory deficits of the extremities, 6%–17%, Scoliosis 18%-50%, Ataxia or gait impairment, decreased coordination 4%–9%,Spasticity 6% [8].
The syringomyelia is define as cerebral spinal fluid cavitation within the spinal cord seen as high signal intensity on T2W image MRI sequence. Syringomyelia was found in 8% of our study population.
The pathogenesis of syringomyelia associated with CMI has not been clarified. Many theories explaining the presence of syringomyelia in CMI have been postulated in literature, however disorder in CSF pathway around FM is taught to be main cause of syringomyelia [9].
The prevalence of syringomyelia in CMI is variable among adults and pediatric population. The occurrence of a syringomyelia in association with CMI varies between 35 to 75% in pediatric patients while in adults syringx associated with CMI varies between 40 to 60% [10]. Aitken and colleagues identified syringomyelia in 12% of patients with CMI [11].
The scoliosis associated with CMI in our study is 5% of the study population.
The exact mechanism of scoliosis in association with CMI is not well known. It is thought to result from chronic compression of cervico-medullary junction by cerebellar tonsils, abnormality in posterior column tracts affect postural reflex resulting in difficulty sustaining appropriate posture there by subsequent scoliosis. However others authors associated the scoliosis with the presence of syringomyelia [12]. Mohammad Hassan A, et al. who report scoliosis resulting from isolated CMI in 3.0% [12]. On the other hand Palma Ciaramitaro, et al. found scoliosis in18%-50% of CMI [10].
Sahib SS, et al. [13] in their study on morphometric and volumetric in pediatric population with CMI found no clinical usefulness of 2D or 3D measurements that can help to differentiate symptomatic pediatric patients with CMI from those who are asymptomatic for CMI in their study, hence recommend another diagnostic criteria beyond classic measurement of tonsil position useful for detecting best candidates for surgical management in patients with CMI [13].
Our study showed a correlation between myelopathy severity and the volume of herniated cerebellar tonsils. There was a proportional increase of volume of herniated cerebellar tonsils and the severity of myelopathy. In addition, our study found a crescendo relationship between T/F volume ratio (cerebellar tonsils volume/foramen magnum volume) and severity of myelopathy. The increase of T/F volume ratio is proportional to the severity of myelopathy.
Currently, there is paucity of data in literature showing the relationship of severity of myelopathy and cerebellar tonsil volume as well as the relationship between T/F volume ratio (cerebellar tonsils volume/foramen magnum volume) and severity of myelopathy as discussed in our study. The T/F volume ratio (cerebellar tonsil volume/Foramen magnum volume) and cerebellar tonsils volume can be an additional tool to be used in diagnosis and predict the severity of CMI.
Conclusion
Many studies showed no correlation between cerebellar tonsils herniation and clinical severity in patients with CMI and suggest other diagnostic criteria beyond standard measurement of cerebellar tonsil position which can help in determining the best candidates who need surgical management for patients suffering from CMI. Our study is the first in current literature to show the correlation between the tonsil volume and T/F volume ratio (cerebellar tonsil volume/ foramen magnum volume) and headache severity using NRS as well as severity of myelopathy using mJOA scale. The study shed light on cerebellar tonsil volume and T/F volume ratio as predictors of severity in patients with CMI. Further studies are recommended to find out if cerebellar tonsils volume and T/F volume ratio (cerebellar tonsil volume/foramen magnum volume) can be used as diagnostic tool in patients with CMI.
Study Limitation and Strength
We should have used imbedded digital calculation of the volume instead of classic calculation of sphere formula which gives approximate result but not true results of calculation. The Foramen magnum is virtual therefore it is exact shape is debatable. The volumetric measurement of cerebellar tonsils and foramen magnum are ideal reflection of severity in patients with Chiari Malformation type I.
References
-
Tubbs RS, Lyerly MJ, Loukas M, Shoja MM, Oakes WJ, et al. (2007) The pediatric Chiari I malformation: a review. Childs Nerv Syst 23(11): 1239-1250.
-
Barkovich AJ, Wippold FJ, Sherman JL, Citrin CM (1986) Significance of cerebellar tonsillar position on MR. AJNR Am J Neuroradiol 7(5): 795-799.
-
Nicholas RP, Lavallée LT, Nguyen LN, Witiuk K, Ross J, et al. (2016) Prostate volume estimations using magnetic resonance imaging and transrectal ultrasound compared to radical prostatectomy specimens. Can Urol Assoc J 10(7-8): 264-268.
-
Nathan MS, Seenivasagam K, Mei Q, Wickham JEA, Miller RA, et al. (1996) Transrectal ultrasonography: why are estimates of prostate volume and dimension so inaccurate. British Journal of Urology 77(3): 401-407.
-
Arnautovic A, Splavski B, Frederick A (2014) Boop and Kenan I. Arnautovic. Pediatric and adult Chiari malformation Type I surgical series 1965–2013: a review of demographics, operative treatment, and outcomes. J Neurosurg Pediatr 5(2): 161-177.
-
Houston JR, Allen NJ, Eppelheimer MS, Bapuraj JR, Biswas D, et al. (2019) Evidence for sex differences in morphological abnormalities in type I Chiari malformation. Neuroradiol J 32(6): 458-466.
-
Heffez DS, Broderick J, Connor M, Mitchell M, Galezowska JA, et al. (2020) Is there a relationship between the extent of tonsillar ectopia and the severity of the clinical Chiari syndrome? Acta Neurochir 162(7): 1531-1538.
-
Pindrik J, Johnston JM (2015) Clinical Presentation of Chiari I Malformation and Syringomyelia in Children. Neurosurg Clin N Am 26(4): 509-514.
-
Koyanagi I, Houkin K (2010) Pathogenesis of syringomyelia associated with Chiaritype 1 malformation: review of evidences and proposal of a new hypothesis. Neurosurg Rev 33(3): 271-285.
-
Ciaramitaro P, Ferraris M, Massaro F, Garbossa D (2019) Clinical diagnosis-part I: what is really caused by Chiari I. Child’s Nervous System 35(10): 1673-1679.
-
Aitken LA, Lindan CE, Sidney S, Gupta N, Barkovich AJ, et al. (2009) Chiari type I malformation in a pediatric population. Pediatr Neurol 40: 449-454.
-
Noureldine MHA, Shimony N, Jallo GI, Groves ML (2019) Scoliosis in patients with Chiari malformation type I. Child’s Nerv Syst 35(10): 1853-1862.
-
Khalsa SSS, Geh N, Martin BA, Allen PA, Strahle J (2018) Morphometric and volumetric comparison of 102 children with symptomatic and asymptomatic Chiari malformation Type I. J Neurosurg Pediatr 21(1): 65-71.
- Ultrasound Guided Therapeutic Nerve Blocks
- Cyclops Lesion Without ACL Reconstruction: A Rare Case in a Patient with Intact Anterior Cruciate Ligament and Tibial Plateau Fracture
- Dosimetric Comparison between Two Dose Calculation Algorithms in SBRT Treatment of Lung Cancer in Ring-based and C-arm Radiation Therapy Equipment
- Adolescent Testicular Adrenal Rest Tumors: A Case Report and Review of the Literature
- Giant Intrathoracic Lipoma: A Rare Presentation
- Image of a Right Renal Angiomyolipoma Complicated by Hemorrhage