Bariatric Surgery as a Treatment for Type 2 Diabetes Mellitus: A Narrative Review
Diabetes is a chronic disease with high morbi-mortality and has been considered in the entire world a public health problem. Type 2 diabetes mellitus (T2DM) that accounts up to 95% of all type of diabetes presents hyperglycemia due to deficient secretion or action of insulin and may lead to microvascular complications, specifically retinopathy, nephropathy and neuropathy. Bariatric surgery (BS) has been proven to be a viable option for the treatment of severe obesity in comparison to conservative methods, with long-lasting weight loss and the resolution of obesity-related comorbidities like T2DM. BS results on diabetes remission were pondered. More researches on the mechanisms by which BS achieves its results are needed. The indications of this kind of intervention for mild obese patients must also be further elucidated
Type 2 Diabetes Mellitus
Type 2 diabetes mellitus (T2DM) is a chronic disease with one of the major morbidity and mortality in the world [1]. It covers about 90–95% of all type of diabetes and it’s due to a progressive insulin secretory defect secondary to an insulin resistance state. Therefore, T2DM is an endocrine-metabolic disease of complex etiology, characterized by hyperglycemia due to deficient secretion or action of insulin [2]. About 90% of type 2 diabetic patients are obese or overweight [3]. Food intolerance and socioeconomic differences are considered factors in weight gain [4]. Measures as modifications in food consumption, increased physical activity and weight reduction are cheap, effective and with high impact due to their benefits, which can be implemented in health care [5]. Analysing morbidly obese patients, the most observed comorbidities were hypertension (19%), T2DM (6.6%) and dyslipidemia (7.5%) [6]. It has also been shown that the body mass index (BMI) of patients with T2DM have a direct bearing on their blood pressure and hypertension. According to a Taiwan study there was a bigger attenuation of hypertension prevalence especially in diabetic women with lower BMI [7]. Patients with diabetes mellitus and dyslipidemia have higher body mass index (BMI) values [8].
Hypertension has a widely known association with T2DM, they are the two most common chronic diseases associated with death by congestive heart failure [9]. Low adhesion to clinical treatment may lead to poor results [10]. Bariatric surgery (BS), aimed at weight reduction, has been proven to be a viable option for the treatment of severe obesity in comparison to conservative methods, resulting in long-lasting weight loss, improved quality-of- life, and the resolution of obesity-related comorbidities like T2DM (as well as preventing it) in morbidly obese patients [11]. Articles, among systematic reviews and prospective studies, published in the last ten years at Lilacs, Pubmed and Science Direct databases were researched to support this narrative review using the medical subject headings terms: “diabetes”, “bariatric surgery”, “metabolic surgery” and “gastric bypass”. Bibliographies of the systematic reviews were also searched and relevant papers were included. BS results on diabetes remission were analyzed. The risk of T2DM is higher in older patients or with: family history of the disease, obesity, hypertension, lack of physical activity, metabolic syndrome and prior Gestational Diabetes Mellitus (GDM). T2DM is often associated with a strong genetic predisposition, more so than type 1 diabetes. However, the genetics of T2DM is poorly understood. Although genetic risk factors increase susceptibility to diabetes and are not modifiable, environmental factors, like changes in lifestyle, play an important role in the emergence and development of the disease and are susceptible to prevention and control [2, 5]. There are several causes of type 2 T2DM. Although the specific etiologies are not known, autoimmune destruction of β-cells does not occur, and patients do not have any of the other known causes of diabetes. Obesity or increased percentage of body fat distributed predominantly in the abdominal region causes some degree of insulin resistance. Therefore, testing to detect T2DM in asymptomatic people should be considered in adults of any age who are overweight or obese (BMI ≥25 kg/m2) and who have one or more additional risk factors for diabetes. For all patients, particularly those who are overweight or obese, testing should begin at age 45 years [2]. UK Prospective Diabetes Study (UKPDS) concluded that the complications of T2DM, previously often regarded as inevitable, could be reduced by improving blood glucose and/or blood pressure control. Reducing glucose exposure (HbA1c 7.0 % versus 7.9 % over median 10.0 years), with sulphonylurea or insulin therapy, reduced the risk of “any diabetes-related endpoint” by 12% and microvascular disease by 25%. Although neither of these therapies impaired quality of life, both increased risk of hypoglycemia and weight gain [12].
Diabetes Complications
T2DM may lead to microvascular complications, specifically retinopathy, nephropathy and neuropathy. Non-proliferative retinopathy is the most common complication for patients with T2DM, it is characterized by microaneurysms in the retina and altered vascular permeability which may lead to macular edema and result in substantial visual impairment [13]. Diabetic retinopathy (DR) affects 40%–50% of patients with diabetes and about 37% of the patients with T2DM have some degree of retinopathy at the time of diagnosis [14]. Important DR risk factors include age, hyperglycemia, hypertension, diabetes duration, dyslipidemia, and genetic factors [15]. Diabetic nephropathy is a persistent increase in albuminuria to levels above 30 mg of albumin per gram of urine creatinine. The glomerular filtration rate (GFR) decreases as a result of renal interstitial fibrosis, thus producing macroalbuminuria and possibly setting the stage for the onset of end-stage renal disease (ESRD). Diabetic neuropathy encompasses microvascular degeneration and nerve fiber conduction deterioration which decrease tactile stimuli and increase thermal thresholds, chronic pain, and paresthesia. In 50% of the cases the manifestations are involved with sensorimotor alterations showing a stocking-and-glove distribution [13]. Cholesterol levels are higher in type 2 diabetes mellitus patients with albuminuria. Increased urinary albumin excretion rate (UAER), is associated with atherosclerotic risk factors (hypertension, dyslipidemia and is predictive for progressive renal failure and increased cardiovascular morbidity and mortality in diabetic and non-diabetic patients [16]. Little information is available concerning the lipid abnormalities associated with increased UAER and UAER relation to increased risk of cardiovascular disease [17]. Central obesity was associated with increased UAER in the early stages of kidney disease without clinical macro albuminuria in type 2 diabetic women [18].
Smoking habits led to high total cholesterol in general adult. Smoking habits and hypercholesteremia were both definitive risk for cerebrovascular disease. Smoking habits and hypercholesteremia were also the confirmed risk for dementia, depression, disability and so on, all of these increased mortality rate in the elderly above 65 year [19]. A Taiwanese study demonstrated that the predisposition to albuminuria in patients with type 2 diabetes mellitus was dependent on the joint effects of the risk factors and the DD genotype of the angiotensin- converting enzyme gene. Thus, those patients with type 2 diabetes mellitus who simultaneously carry the DD genotype and possess the individual risk factor of hypertension, smoking, dyslipidemia or obesity are at high risk of albuminuria [16]. Congestive Heart Failure (CHF) is the endpoint of the process, particularly in the case of cardiovascular diseases such as hypertensive heart disease, especially coronary or valve pathologies [20]. CHF importance relies on the fact that it is still the most common reason for hospitalization of ≥ 65 years old people in United States, including over 1 million patients admitted for this condition and more than 300,000 deaths each year [21]. Worldwide speaking, it affects 26 million people. 30% of the cohort of a study regarding the incidence of CHF in middle and low income population was shown to be diabetic, which represents a broad part of the general population [22]. Diabetes is one of heart failure risk factors [23]. And heart failure in type 2 diabetes is generally associated with a high death rate [24]. It has also been shown that there´s an increased risk of heart failure hospitalization associated with short term use of DPP-4 (a type of ant hyperglycemic drug). On the other hand, long term use has proven to have a protective effect that may be related to better long term diabetes control than to the protective effect of the drug itself on heart failure [25]. The use of pioglitazone – hypoglycemic from thiazolidinedione (TZD) class – may also increase signs of heart failure in susceptible patients. However, the occurrence of serious heart failure did not translate to increased mortality or cardiovascular morbidity. Despite that, most mechanisms regarding the cardiovascular outcomes remain unclear requiring further investigation [24].
Bariatric Surgery
Some studies have revealed that bariatric surgery could improve renal function in patients with T2DM [26]. But, evidence of the effect of bariatric/metabolic surgery on microvascular complications is already emerging in the literature [13]. Bariatric surgeries, considered more effective than medical therapy in treatment of T2DM in patients with severe obesity, include a variety of gastrointestinal surgical procedures and achieve substantial and sustained weight loss and glucose-lowering effects. It can also bring early and relevant resolution rates of hypertension [10]. Rates of short and long-term diabetes remission are around 60 to 95%, with low frequency of perioperative and postoperative complications [27]. However, surgery is often not advocated for patients with T2DM who are overweight or have mild obesity [28]. Roux-en-Y gastric bypass (RYGB) is considered one of the most effective treatments for maintaining long-term weight loss. However, it is also associated to failures manifested by the inability to maintain weight loss, weight gain or poor glycemic control [4]. Despite indications for sleeve gastrectomy (SG) or vertical gastrectomy have increased for treatment of morbid obesity, results at medium and long term remain in constant research, as well as several aspects related to surgical technique [6, 29]. These surgical interventions, including ileal interposition, are an important component of metabolic and neuroendocrine managing which favors the resolution of T2DM, even in patients with mild or excessive obesity [30]. In previous treatments for weight loss, 92% of patients in preoperative of bariatric surgery have already done hypo caloric diet and 83% have used anorectic drug, with high success of these treatments. However, 75% of them regained weight in less than 1 year [8]. Recently, gastrointestinal metabolic surgery has been proposed as a new treatment modality for T2DM in patients with BMI < 35 kg/m2 as it had been proven that it results in better glycemic control compared with medical treatment in these patients [11].
Surgical Techniques
The number of bariatric techniques is increasing quickly. New surgeries or modifications of frequently performed surgeries are being proposed to improve efficiency or decrease complications [27]. BS is totally different from gastrointestinal metabolic surgery or diabetes surgery (DS) in the patient characters, goals of surgery, and management although similar in surgical procedure [11].
Laparoscopic techniques are now largely used as they reduced the surgical stress and mortality as compared to the open surgeries. The most frequent surgeries are RYGB, SG, adjustable gastric band (AGB), bilio-pancreatic diversion (BPD) and BPD with a duodenal switch (BPD- DS) [31].
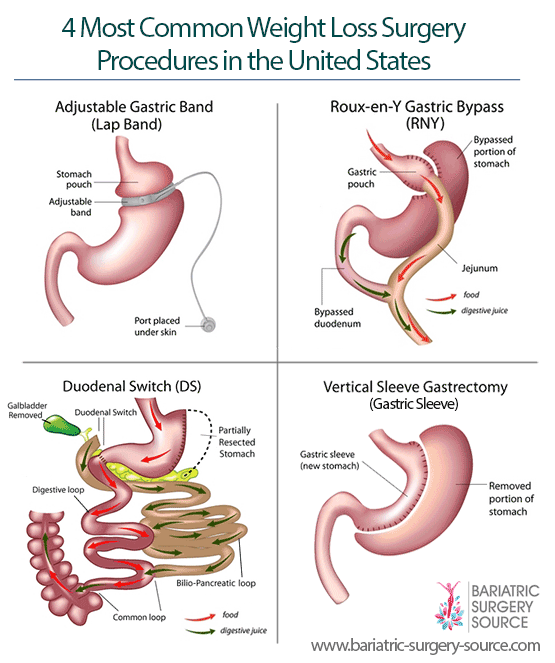
Reprinted from Bariatric Surgery Source. 2016. Retrieved from: http://www.bariatric-surgery- source.com/types-of-bariatric-surgery.html SG, or vertical gastrectomy, have been considered a durable BS comparable to gastric bypass procedures, besides avoids gastric cancer risk in the excluded stomach and reduces the incidence of micronutrient deficiency. At the same time, excluding the duodenum in the bypass procedure had been proven to be more effective in glycemic control than a procedure without duodenum exclusion, such as SG and AGB [11].
Diabetes Resolution Mechanisms through Surgery
Some theories have been created to explain the mechanisms behind diabetes remission after BS [32]. However they are still not completely understood; encompass improved insulin action, better β-cell function, higher adiponectin, lower inflammation and complex changes of hormones of the entero-insular axis, GLP-1 and glucose dependent insulinotropic polypeptide (GIP) [27]. One of the theories considers that the glycemic control improves shortly after surgery simply because the patients are not permitted to eat much in the postoperative period, and by the time they start eating regularly again, the insulin-sensitizing effects of dynamic weight loss are acting. This hypothesis fails to explain the superiority of glycemic control achieved after RYGB compared to equivalent weight loss from dieting or restrictive bariatric operations [32]. The hindgut hypothesis proposes that diabetes control is the result of the delivery of chyme nutrients directly into the distal intestine. The L cells of the distal intestine, in response to the presence of nutrients, secret Glucagon- like peptide 1 (GLP-1) which is the major mediator in this process. GLP-1 stimulates the secretion of insulin and shows proliferative and ant apoptotic effects on β-cells, thus amplifying a physiologic signal that enhances glucose metabolism. This theory is based on experiments such as ileal interposition (transposition of a segment of distal ileum to the jejunum with no gastric or intestinal resection) [32]. The foregut hypothesis suggests that food diverted from the duodenum and proximal jejunum possibly prevents the secretion of a specific signal that promotes insulin resistance and T2DM [3, 32]. It was observed that the surgical procedures have a potential role in albuminuria remission. However, it is not clear if weight loss alone supports decreases in proteinuria. The renoprotection offered by incretins like GLP-1 was described in preclinical animal models [15].
Bariatic Surgery Results
A retrospective review of groups of patients who received BS versus DS, found that patients with diabetes lost less weight than those without diabetes. After five years, although weight loss was inferior in the DS group, the remission of diabetes remained high in the DS group, which shows the importance of the weight loss in diabetes treatment. 73.3% of the DS’s were gastric bypass procedures, while it made up only 47.1% of BS’s [11]. BS, which is a 2-hour procedure requiring a 2-day hospital stay, is a relatively well-tolerated option in patients with T2DM and mild obesity (25≤ BMI ≤35 kg/m2). Being that RYGB and SG had comparable early postoperative morbidity [28]. A study comparing obese patients who underwent gastric surgery with conventional treatment analyzed that after two years the weight had increased by 0.1% in the control group and had decreased by 23.4% in the surgery group. After 10 years, these results changed to 1.6% and
16.1% respectively. The incidence of T2DM in patients undergoing conservative treatment was 28%, compared to 7% in operated patients. Furthermore, gastric surgery had better recovery from diabetes, hypertriglyceridemia, low levels of high-density lipoprotein cholesterol, hypertension, and hyperuricemia, higher level of physical activity and lower caloric intake [33]. One year after RYGB in obese, grades 2 and 3, a reduction in the number of patients with diabetes and Metabolic Syndrome was observed (48% and 85%, respectively). The subjects submitted to gastric bypass also had statistic significant higher reductions in BMI, waist circumference, fasting plasma glucose and serum LDL-cholesterol [34]. Metabolic surgery performed on patients with BMI<30kg/m2 has been shown to be a safe and effective method to treat diabetes. There is still controversy about the factors that could be associated with durable remission of the disease [32]. Patients with T2DM and mild obesity who underwent RYGB had the average BMI decreased to 24.7 Kg/m2 and 93.6% met criteria for remission of T2DM at 3 years follow up; noting that all patients had improvement in glycemic control [31]. In 74.6% of severe obese patients submitted to metabolic surgery, remission lasted over two years and BPD was the most effective intervention used, followed by RYGB and SG [35]. Glycated hemoglobin of 6% or less was achieved by 5% of the patients that were treated with drugs, versus 38% of those that associated bypass with medical treatment and 24% of who underwent SG and used medical therapy [36]. Patients with elevated initial maximum BMI (≥ 50kg/m2) displayed higher T2DM remission and weight loss failure rates after at least two years from RYGB [4]. Remission of diabetes and dyslipidemia occurred in all 120 obese patients submitted to SG in a study in Brazil and there was improvement or remission in 86% of them after 2 years [6]. A cohort study observed that 12.2% of the patients that underwent RYGB had only diabetes resolution, 7.8% had only hypertension resolution, 77.8% resolved both disorders, and 2.2%, none [10].
On the 30th postoperative day of RYGB in patients with BMI >35 kg/m2, a weight loss of approximately 10% was noted in relation to preoperative weights [4].
Reversal or Amelioration of Complications of Diabetes
Analyzing patients post bariatric surgery, it was observed that they remain at risk for developing sight- threatening diabetic retinopathy (STDR), even those who did not have evidence of DR before procedure. However, surgery was associated with a lower progression to STDR or maculopathy compared with routine care (5.7% versus 12.1%) [15]. There is low-quality evidence suggesting that BS might improve albuminuria and urine albumin-to-creatinine ratio (uACR) in patients with T2DM. The effect is probably a result of improvement of hyperglycemia-induced metabolic disorders and obesity-induced hyperfiltration [26]. A meta-analysis with 522 patients reported a reduction of 1.1 mg in albumin excretion for every 1 kg of bodyweight lost after different weight loss methods of bariatric/metabolic surgery. But, the impact of surgery on renal function and on evidence of renal inflammation suggests these effects on the kidney are multifactorial and not exclusively related to weight loss [13]. The analysis of patients that underwent RYGB showed that the percentage of patients with neuropathy (31.3%) was lower than the number of cases at baseline (52.9%). However, the small number of subjects did not made possible a statistically significant data. But, none of the patients developed neuropathy after the treatment [3].
Complications of Bariatric Surgery
Perioperative complications were more frequent after RYGB than AGB, even if the mortality of both techniques were lower than 0.3%. Complications like bleeding, stomal stenosis, leak, vomiting, reflux and nutritional or electrolyte abnormalities were higher for gastric bypasses than AGB, while reoperations were more frequent for AGB. The nutritional deficiencies are very frequent after bypasses, in particular after BPD, requiring a lifelong vitamins and trace elements supplementation. Therefore, although there are low rates of complications, the risk- benefit of BS should be considered [27]. There were only two complications (bronchial pneumonia and dehydration), with good response to clinical treatment after the analysis of SG in a study involving 120 morbid obese patients [6]. Comparing complication rates of DS and BS, similar numbers were noted. But, DS had a significantly higher mortality rate than BS [11]. Smoking can be considered as a modifiable risk factor for early complications after BS in patients with T2DM and lower BMI [23].
Diabetes Recurrence or Failure in Reversal
Rates of diabetes recurrence are not well known, but the free-of-disease time should soften diabetes complications and mortality [27]. After 1 year of RYGB in 17 obese patients with BMI > 35 kg/m2, one of them remained diabetic, with no remission [3]. In a follow-up study of patients undergoing gastric bypass, 5 years from the initial remission, up to 1/3 of them may suffer from a diabetes recurrence, usually associated with the severity and duration of preoperative disease [37]. From 120 morbidly obese patients submitted to SG, 9.1% had regained more than 5 kg of body weight [6]. The recovery rates from hypercholesterolemia did not differ between obese patients who underwent gastric surgery and the conventionally treated even ten years after [33]. Discussion Metabolic deregulation is the defining characteristic of T2DM [13]. The gut hormones play an important role in insulin secretion and glucose homeostasis in patients with T2DM. Bariatric surgical interventions change the digestive hormone profile, stimulating the secretion of the incretin hormones such as anorexic GLP-1 and PYY, suppressing orexigenic hormones like ghrelin [30]. The postoperative control of diabetes is a direct consequence of the rearrangement in gastrointestinal anatomy, and not merely the reduction in caloric intake and weight. BMI alone is not an ideal parameter for defining the indication of surgery for diabetic patients. There isn´t no scientific evidence of a BMI cutoff point for selecting the group that will benefit from the surgical procedure [32]. The sleeve gastrectomy is a surgical technique that has proven to be safe and effective in the surgical treatment of obesity and control of comorbidities [6]. Metabolic surgery needs more studies and discussions to determine its true position as treatment for non-obese diabetic people [32]. RYGB was a safe and effective therapeutic tool to achieve hypertension resolution in patients who also had diabetes mellitus [10].
| Positive Findings | ||
|---|---|---|
| Efficient obesity treatment Therapeutic tool Reversion of comorbidities and its complications (e.g., diabetes, albuminuria, hypertension, lower progression of retinopathy) | ||
| Negative Findings | ||
| Poorly understood Relapse occurs or Failure to reverse Indication for non-obese diabetic population needs more studies | ||
| Complications | ||
| Smoking related to early complications Nutritional Deficiencies; Bleeding, stomal stenosis, leak, vomiting, reflux and nutritional or electrolyte abnormalities; Diabetes surgery has a higher mortality rate. |
Table 1: Summary of findings and outcomes. In conclusion, BS has been shown to be an efficient procedure on the obesity treatment
Table 1: Summary of findings and outcomes. In conclusion, BS has been shown to be an efficient procedure on the obesity treatment and the reversion of its comorbidities such as diabetes. However, more researches on the mechanisms by which BS achieves these results are needed. The indications of this kind of intervention for mild obese patients must also be further elucidated.
References
-
Leyva ER, Aldana DA, Moreiro RG, Mayté Álvarez Fernández, Yuliet Ro dríg uez Be bert, et al_._ (2009) Diabetes mellitus in patientsfromCiego de Avilaprovince: secular serie 1997-2008. Rev Cubana Endocrinol 20(3): 104-119.
-
American Diabetes Association (2015) Classification and Diagnosis of Diabetes. Diabetes Care 38(1): S8- S16.
-
Zeve JL, Tomaz CA, Nassif PA, Lima JH, Sansana LR, et al. (2013) Obese patients with diabetes mellitus type 2 undergoing gastric bypass in Roux-en-Y: analysis of results and its influence in complications. ABCD 26(1): 47-52.
-
Costa AC, Furtado MC, Godoy EP, Pontes ER, Tognini JR, et al. (2013) Insufficient loss of weight and/or absence of DM2 remission after Roux-en-Y gastric bypass: factors that may influence the unsatisfactory results. ABCD 26(2): 112-116.
-
Columbié YL, Miguel-Soca PE, Vázquez DR, Chi YB (2016) Risk factors associated to occurrence of type 2 diabetes mellitus in adults. Rev Cubana Endocrinol 27(2): 123-133.
-
Ramos AC, Bastos EL, Ramos MG, Bertin NT, Galvao TD, et al. (2015) Medium-term follow-up results with laparoscopic sleeve gastrectomy. ABCD 28(1): 61-64.
-
Tseng CH (2007) Body mass index and blood pressure in adult type 2 diabetic patients in Taiwan. Circulat J 71(11): 1749-1754.
-
Silva PT, Patias LD, Alvarez GC (2015) Profile of patients who seek the bariatric surgery. ABCD 28(4): 270-273.
-
Koike MK, Silva V, Romanek FA, Shirassu MM (2016) Relationship of comorbidities and heart failure mortality in the city of São Paulo, Brazil. Medical Express 3(2): 1-6.
-
Cazzo E, Gestic MA, Utrini MP, Machado RR, Pareja JC, et al. (2014) Control of hypertension after Roux-en-Y gastric bypass among obese diabetic patients. Arq Gastroenterol 51(1): 21-24.
-
Lee WJ, Almulaifi A, Chong K, Yao WC, Tsou JJ, et al. (2016) Bariatric versus diabetes surgery after five years of follow up. ASJSUR 39(2): 96-102.
-
Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA (2008) 10-Year Follow-up of Intensive Glucose Control in Type 2 Diabetes. NEJM 359(15): 1577- 1589.
-
Cohen R, Pechy F, Petry T, Correa JL, Caravatto PP, et al. (2015) Bariatric and metabolic surgery and microvascular complications of type 2 diabetes mellitus. J Bras Nefrol 37(3): 399-409.
-
Murray P, Chune GW, Raghavan VA (2010) Legacy effects from DCCT and UKPDS: what they mean and implications for future diabetes trials. Curr Atheroscler Rep 12(6): 432-439.
-
Amin AM, Wharton H, Clarke M, Syed A, Dodson P, et al. (2016) The impact of bariatric surgery on retinopathy in patients with type 2 diabetes: a retrospective cohort study. SOARD 12(3): 606-612.
-
Tseng CH, Tseng CP, Chong CK (2010) Joint effects of hypertension, smoking, dyslipidemia and obesity and angiotensin-converting enzyme DD genotype on albuminuria in Taiwanese patients with type 2 diabetes mellitus. Clin Biochem 43(7-8): 629-634.
-
Tseng CH (2005) Lipid abnormalities associated with urinary albumin excretion rate in taiwanese type 2 diabetic patients. Kidney Int 67(4): 1547-1553.
-
Tseng CH (2005) Waist-to-height ratio is independently and better associated with urinary albumin excretion rate than waist circumference or waist-to-hip ratio in Chinese adult type 2 diabetic women but not men. Diab Care 28(9): 2249-2251.
-
Yan-Ling Z, Dong-Qing Z, Chang-Quan H, Bi-Rong D (2012) Cigarette Smoking and its association with serum lipid/ lipoprotein among chinese nonagenarians/ centenarians. Lipid in Health and Disease 11(94): 1-6.
-
Conraads VM, Beckers PJ (2010) Exercise training in heart failure: practical guidance. Heart 96(24): 2025- 2031.
-
Scott MC, Winters ME (2015) Congestive Heart Failure. Emerg Med Clin of North America 33(3): 553- 562.
-
Dokainish H, Teo K, Zhu J, Roy A, Al-Habib K, et al. (2015) Heart failure in low- and middle-income countries: Background, rationale, and design of the International Congestive Heart Failure Study (INTER- CHF). Americ Heart J 170(4): 627-634.
-
Kalogeropoulos A, Georgiopoulou V, Kritchevsky SB, Psaty BM, Smith NL, et al. (2009) Epidemiology of incident heart failure in a contemporary elderly cohort: the health, aging, and body composition study. Arch Intern Med 169(7): 708-715.
-
Erdmann E, Charbonnel B, Wilcox R, Skene A, Beneditti M, et al. (2007) Pioglitazone Use and Heart Failure in Patients With Type 2 Diabetes and Preexisting Cardiovascular Disease Data from the PROactive Study (PROactive 08). Diab Care 30(11): 2772-2778.
-
Tseng CH (2016) Sitagliptin and heart failure hospitalization in patients with type 2 diabetes. Oncotarget 9.
-
Zhou X, Li L, Kwong JSW, Jiajie Yu, Youping Li, et al. (2016) Impact of bariatric surgery on renal functions in patients with type 2 diabetes: systematic review of randomized trials and observational studies. SOARD.
-
Muscelli E, Alecrim HM (2014) Impact of bariatric surgeries on diabetes outcomes. Rev Soc Bras ClínMéd 12(2): 1-11.
-
Aminian A, Andalib A, Khorgami Z, Sangeeta R Kashyap, Burguera B, et al. (2016) A nationwide safety analysis of bariatric surgery in non severely obese patients with type 2 diabetes. SOARD.
-
Ramos AC, Bastos EL, Ramos MG, Bertin NT, Galvao TD, et al. (2015) Technical aspects of laparoscopic sleeve gastrectomy. ABCD 28(1): 65-68.
-
Eickhoff H, Matafome P, Seica R, Sousa FC (2016) Metabolic surgery in patients with type 2 diabetes: Fiction or therapeutic option? Rev Port Cir 36(1): 19- 28.
-
Lanzaren E (2013) Surgical treatment in type 2 diabetes and mild obesity. Rev Chil Cir. 65(1): 41-49.
-
Campos JM, Lins DC, Silva LB, Araujo-Junior JG, Zeve JL, et al. (2013) Metabolic surgery, weight regain and diabetes re-emergence. ABCD 26(1): 57-62.
-
Sjöström L, Lindroos AK, Peltonen M, Torgerson J, Bouchard C, et al. (2004) Lifestyle, Diabetes, and Cardiovascular Risk Factors 10 Years after Bariatric Surgery. NEJM 351(26): 2683-2693.
-
Schmid H, Goelzer Neto CF, Dias LS, Weston AC, Espíndola MB, et al. (2015) Metabolic syndrome resolution by Roux-en-Y gastric bypass in a real world: a case control study. Rev Assoc Med Bras 61(2): 161-169.
-
Buchwald H, Estok R, Fahrbach K, Banel D, Jensen, et al. (2009) Weight and Type 2 Diabetes after Bariatric Surgery:Systematic Review and Meta-analysis. Am J Med 122(3): 248-256.
-
Ilias EJ (2014) Bariatric surgery versus medical therapy for diabetes - 3-year follow-up. Rev Assoc Med Bras 60(4): 305.
-
Arterburn DE, Bogart A, Sherwood NE, Sidney S, Coleman KJ, et al. (2013) A multisite study of long- term remission and relapse of type 2 diabetes mellitus following gastric bypass. Obes Surg 23(1): 93-102.
- Investigation of Polymorphisms in PPAR-Ɣ and TRHR Genes and their Impact on Turkish Diabetic and Obese Individuals
- The Impact of Aircraft Noise Exposure on the Efficacy of Empagliflozin Therapy in an Animal Model of Obesity
- Rooibos Mitigates Metabolic and Inflammatory Dysfunctions in Mice Fed a High-Carbohydrate Diet
- Synergistic Effect of Combined Leaf Extract of Vernonia amygdalina, Ocimum gratissimum, and Zingiber officinale Tuber on Phytochemical Profile, Antioxidant Activity, Serum Insulin, and Biochemical Parameters in Streptozotocin-Induced Diabetic Rats
- Investigation of Cardiovascular Responses to Aerobic Exercise in Obese University Students
- A Look at the Phase Angle Obtained by Electrical Bioimpedance