Effects on Metabolic Parameters of Addition of SGLT‐2 Inhibitors on Patients with Type2 Diabetes Inadequately Controlled with DPP‐IV Inhibitors and Metformin
Background: Practice guidelines are open regarding choice of therapy after metformin. The second line agent’s insulin (INS), sulphonylureas (SU) and thiazolidinediones (TZD) may cause either hypoglycaemia or weight gain. Dipeptidyl peptidase‐IV (DPP-4) inhibitors are unlikely to produce that. Sodium‐glucose transporter‐2 (SGLT -2) inhibitors are newer agents with the advantage of weight loss. Indian data regarding combination therapy with Metformin withDPP-4 inhibitors plus SGLT-2 inhibitors arescanty; hence this study is relevant .Moreover the number of patients studied, duration of study, study variables and effects of three SGLT-2inhibitors were analyzed separately. Objectives: To study the glycaemic and other metabolic parameters after treatment with SGLT‐2 inhibitors-canagliflozin or, dapagliflozin, or, empagliflozin in type 2 Diabetes (T2DM) patient inadequately controlled (HbA1c >7.5%) with DPP-4 inhibitors plus metformin. Methodology: Data of 101 T2DM patients inadequately controlled (HbA1c> 7.5%) with DPP-4 inhibitors plus metformin who were prescribed canagliflozin 100 mg or, dapagliflozin 5 or 10 mg, or empagliflozin 10 mg or 25 mg once daily with mean follow‐up duration of 23 weeks were analyzed. Subjects receiving INS, SU and TZD were excluded from analysis. Changes in weight, blood pressure, glycaemia, lipids, renal and hepatic parameters were studied. Subgroup analyses were done to see effects of three SGLT‐2 inhibitors. Results: Results showed that addition of SGLT-2 inhibitors produced favourable effects on all metabolic parameters studied. Conclusion: Our study shows that addition of SGLT2 inhibitors on existing therapy with DPP-4 inhibitors and metformin produces favourable effects on metabolic parameters with the advantage of weight loss and without producing major hypoglycaemic events.
Introduction
It has been seen that modest and sustained weight loss improves glycaemic control and reduces the need for glucose-lowering medications in overweight and obese patients with T2DM [1, 2, 3]. Because the pathogenesis of T2DM is complex and involves multiple metabolic defects, the use of combination therapy with antidiabetic drugs with different mechanisms of action has the advantage of combining complementary mechanisms and has the potential of producing an additive reduction in HbA1c [4].
DPP-4 inhibitors and SGLT-2 inhibitors exert their glucose-lowering effects via different and complementary mechanisms. DPP-4 inhibitors prevent the enzymatic degradation of endogenous incretin hormones (active glucagon-like peptide [GLP]-1 and glucose-dependent insulinotropic polypeptide [GIP]) [5, 6]. Increased plasma concentrations of GLP-1 and GIP stimulate insulin secretion from pancreatic β-cells and inhibit glucagon secretion from pancreatic α-cells, which causes inhibition of endogenous glucose production and a reduction in plasma glucose concentration [7]. SGLT-2 inhibitors reduce the plasma glucose concentration by inhibiting renal glucose reabsorption and producing glucosuria [8]. Metformin and SGLT2 inhibitors are agents associated with weight loss whereas DPP4 inhibitors appear to be weight neutral. When one single pharmacological class does not reach HbA1c target as monotherapy or even when added to metformin, a combination of a DPP-4 inhibitors and a SGLT-2 inhibitors could be helpful with a low risk of adverse events, such as hypoglycaemia or weight gain and the potential advantage of cardiovascular protection [9, 10, 11].
However Indian data regarding combination therapy with metformin withDPP‐4 inhibitors plus SGLT‐2 inhibitors are scanty. In this study we present data Chatterjee S, et al. Effects on Metabolic Parameters of Addition of SGLT‐2 Inhibitors on Patients with Type2 Diabetes Inadequately Controlled with DPP‐IV Inhibitors and Metformin. Diabetes Obes Int J 2019, 4(2): 000201.
regarding the glycaemic and other metabolic parameters after treatment with SGLT‐2 inhibitors-canagliflozin or dapagliflozin or empagliflozin in type 2 DM patient inadequately controlled (HbA1c >7.5%) with DPP‐4 inhibitors plus metformin.
Methods
Methodology
This was a retrospective, real world observational study to evaluate the efficacy and safety of SGLT-2 inhibitors in T2DM patients who were inadequately controlled with (HbA1c >7.5%) DPP-4 inhibitors and metformin. All patients were taking SGLT-2 inhibitors for a period of at least 24 weeks. The study period was from July 2016 to June 2018.
Protocol Characteristics
The included study patients were non-pregnant T2DM who were receiving SGLT-2 inhibitors over and above DPP-4inhibitors plus metformin for a period of at least 24 weeks at the time of recording their data. We excluded all patients with type 1 Diabetes or diabetic ketoacidosis, alcohol or drug dependence, recent or multiple hospitalization for reasons other than hyper glycaemia within past six months, nursing women, history of urinary tract or other systemic infections, haematuria, decompensated heart failure, liver failure, debilitating illness that may adversely affect renal function or on drugs that may adversely affect renal function.
Patients, who were not optimally controlled onDPP- 4inhibitors plus metformin, received SGLT-2 inhibitors as standard of care. Patients not optimally controlled were defined as either having one or more of the following: fasting plasma glucose (FPG) > 150 mg/dL, post prandial plasma glucose (PPPG) > 200 mg/dL, HbA1c>7.5% despite receiving optimal dose of two oral antidiabetic drugs (OADs). All Patients received treatment as per routine standard of care without any experimentation on any patient.
Copyright© Chatterjee S, et al.
Data Collection
Data of all patients fulfilling the inclusion and exclusion criteria was retrospectively collected from our medical case records. Data included all patients’ demographic records with respect to age, gender, body weight, blood pressure (BP), and duration of diabetes. Data was collected of the day of starting SGLT-2 inhibitors and at least 20 weeks after starting SGLT-2 inhibitors. All laboratory investigations data for HbA1c, FPG, PPPG, serum creatinine (Cr), effective glomerular filtration rate(eGFR), urinary albumin creatinine ratio (UACR), sodium (Na) and potassium (K), were also recorded of the day of starting SGLT-2 inhibitors and at least 20 weeks after SGLT-2 inhibitors. Plasma glucose was measured by hexokinase method and HbA1c was measured by high performance liquid chromatographic (HPLC) method (Bio-RAD D-10, Bio-RAD, and Hercules, CA, USA) in our hospitals. Only those patients were considered for final evaluation who had both baseline and post-treatment values of the study parameters. In this study 101 T2DM patients who were inadequately controlled with DPP- 4inhibitors plus metformin were prescribed canagliflozin (100 mg) or dapagliflozin(5 /10 mg), or empagliflozin(10 mg/25 mg) once daily. After a mean follow-up duration of 23 weeks changes in weight, blood pressure, glycaemia, lipids, renal and hepatic parameters were studied. Subgroup analyses were done to see effects of three SGLT- 2 inhibitors. Subjects receiving INS, SU and TZD were excluded from analysis. P<0.05 considered as statistically significant, p computed by paired t‐test.
Results
Table 1 shows the baseline characteristics of the study subjects (n=101). The mean age of the patient was 47.76 years, mean height 162 meters, mean weight and body mass index (BMI) 81.48 kgs and 30.72kg/m2 respectively. The mean systolic and diastolic blood pressures (SBP and DBP) were 131.21 and 79.5 mm of mercury. Mean FBG and PPBG level were 155.55 and 220.33 mg/dl respectively and HbA1c was maintained at 8.17. Obesity was the commonest comorbidity (72.27%) among the study group followed by dyslipidaemia (70.29%), hypertension (63.36%), micro-albuminuria (22.77%), hypothyroidism (20.79%), coronary heart disease (12.87%), fatty liver (11.88%), nephropathy (1.98%).
| Parameter | Mean | Std. Dev. | Median | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Age, years | 47.76 | 11.08 | 47 | ||||||||
| Height, m | 1.62 | 0.1 | 1.64 | ||||||||
| Weight, kg | 81.48 | 14.61 | 80 | ||||||||
| BMI, kg/m2 | 30.72 | 4.91 | 30.33 | ||||||||
| SBP, mmHg | 131.21 | 14.95 | 130 | ||||||||
| DBP, mmHg | 79.5 | 8.39 | 80 | ||||||||
| FPG, mg/dL | 155.55 | 47.8 | 150 | ||||||||
| PPPG, mg/dL | 220.33 | 78.16 | 196.5 | ||||||||
| HbA1c,% | 8.17 | 1.74 | 7.7 | ||||||||
| ALT,U/L | 41.19 | 19.21 | 42 | ||||||||
| AST, U/L | 40.46 | 31.37 | 30 | ||||||||
| CHOLESTEROL, mg/dL | 140.47 | 37.55 | 135 | ||||||||
| TG, mg/dL | 147.58 | 73.54 | 130 | ||||||||
| HDL, mg/dL | 39.1 | 9.31 | 39 | ||||||||
| LDL, mg/dL | 80.6 | 29.48 | 76 | ||||||||
| NON-HDL, mg/dL | 89.99 | 48.08 | 90.5 | ||||||||
| Creatinine, mg/dL | 0.9 | 0.21 | 0.9 | ||||||||
| Duration, weeks | 22.46 | 14.38 | 16.5 | ||||||||
| TG/HDL1 | 4.07 | 2.64 | 3.36 | ||||||||
| ACR | 37.53 | 89.37 | 12.9 | ||||||||
| Met dose, grams/day | 1441.54 | 505.79 | 1000 |
Table 1: Baseline Characteristic Features of the Overall Study Subjects, N=101.
| Co-morbidities | No. of subjects | % | ||||||
|---|---|---|---|---|---|---|---|---|
| HTN | 64 | 63.36 | ||||||
| Micro-albuminuria | 23 | 22.77 |
Table 2: Baseline Characteristic Features of the Overall Study Subjects, N=101.
Chatterjee S, et al. Effects on Metabolic Parameters of Addition of SGLT‐2 Inhibitors on Patients with Type2 Diabetes Inadequately Controlled with DPP‐IV Inhibitors and Metformin. Diabetes Obes Int J 2019, 4(2): 000201.
Copyright© Chatterjee S, et al.
| Nephropathy | 2 | 1.98 |
|---|---|---|
| CHD | 13 | 12.87 |
| Fatty Liver | 12 | 11.88 |
| Dyslipidemia | 71 | 70.29 |
| Overweight/Obesity | 73 | 72.27 |
| Statin Usage | 64 | 63.36 |
| Hypothyroidism | 21 | 20.79 |
Table 3: Baseline Characteristic Features of the Overall Study Subjects, N=101.
| Baseline | Follow-up | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study Parameters | p | ||||||||||||
| Mean | SD | Median | Mean | SD | Median | ||||||||
| Weight, kg | 81.55 | 14.33 | 80.3 | 78.88 | 14.66 | 76 | <0.0001 | ||||||
| BMI, kg/m2 | 30.85 | 4.84 | 30.33 | 27.73 | 9.19 | 29.13 | 0.0002 | ||||||
| SBP, mmHg | 130.85 | 15.01 | 130 | 124.44 | 17.59 | 127 | 0.0015 | ||||||
| DBP, mmHg | 79.43 | 8.54 | 80 | 77.21 | 8.65 | 79.5 | 0.029 | ||||||
| FPG, mg/dL | 154.25 | 48.11 | 147 | 123.15 | 26.4 | 122 | <0.0001 | ||||||
| PPPG, mg/dL | 218.29 | 68.05 | 196 | 176.6 | 54.58 | 165 | <0.0001 | ||||||
| HbA1c,% | 8.09 | 1.68 | 7.65 | 7.33 | 1.6 | 7 | <0.0001 | ||||||
| Cholesterol, mg/dL | 140.82 | 37.5 | 135 | 135.77 | 32.44 | 131 | 0.23 | ||||||
| HDL, mg/dL | 38.97 | 9.31 | 39 | 39.04 | 9.3 | 39 | 0.61 | ||||||
| LDL, mg/dL | 81.04 | 29.5 | 76.5 | 76.81 | 29.27 | 72 | 0.25 | ||||||
| Non-HDL, mg/dL | 89.82 | 48.76 | 90.5 | 80.31 | 48.42 | 86 | 0.042 | ||||||
| Creatinine, mg/dL | 0.9 | 0.21 | 0.9 | 0.89 | 0.24 | 0.9 | 0.71 | ||||||
| TG/HDL, mg/dL | 4.08 | 2.68 | 3.32 | 3.87 | 2.57 | 3.19 | 0.35 |
Table 4: Change in Parameters in the Study Subjects after treatment with DPP-IV Inhibitors+ SGLT-2 Inhibitors + Metformin, N=101.
P<0.05 considered as statistically significant, p computed by paired t-test.
| Baseline | Follow-up | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study Parameters | |||||||||||||
| IQ Range | Median | Range | Lower Quartile | Median | Range | p | |||||||
| ALT | 26 - 54 | 43 | Oct-89 | 23.5 - 44 | 28.5 | 8.4 - 71 | 0.012 | ||||||
| AST | 23.1 - 46 | 30 | 17 - 130 | 26 - 46 | 37 | 16 - 130 | 0.75 | ||||||
| TG | 95 - 173 | 128.5 | 26 - 418 | 91 - 163 | 120 | 54 - 316 | 0.202 | ||||||
| ACR | 8.4 - 28.5 | 12.9 | 0.6 - 574 | Aug-23 | 13 | 2.97 - 199 | 0.22 |
Table 5: Change in Parameters in the Study Subjects after treatment with DPP-IV Inhibitors+ SGLT-2 Inhibitors + Metformin, N=101.
P<0.05 considered as statistically significant, p computed by Signed rank test. Table 2: Change in Parameters in the Study Subjects after treatment with DPP-IV Inhibitors+ SGLT-2 Inhibitors + Metformin, N=101.
Chatterjee S, et al. Effects on Metabolic Parameters of Addition of SGLT‐2 Inhibitors on Patients with Type2 Diabetes Inadequately Controlled with DPP‐IV Inhibitors and Metformin. Diabetes Obes Int J 2019, 4(2): 000201.
Copyright© Chatterjee S, et al.
(p=0.0024) but no such changes were noted in PPBG values.
| Canagliflozin (n=30) | Dapagliflozin (n=40) | Empagliflozin (n=31) | |||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Parameter | Baseline | Follow-up | v | P | e | Baseline | Follow-up | Baseline | Follow-up | ||||||||||||||||||||
| P | valu | e | P | valu | e | ||||||||||||||||||||||||
| Mean±SD | Mean±SD | alu | Mean±SD | Mean±SD | Mean±SD | Mean±SD | |||||||||||||||||||||||
| BMI, kg/m2 | 30.62±4.62 | 28.42±6.95 | 0.004 | 30.09±4.88 | 26.84±10.24 | 0.0081 | 31.62±5.33 | 28.03±9.57 | 0.049 | ||||||||||||||||||||
| SBP, mmHg | 131.83±4.62 | 124.34±14.32 | 0.37 | 128.64±16.82 | 123.67±22.33 | 0.2549 | 133.23±13.23 | 125.06±12.83 | 0.0002 | ||||||||||||||||||||
| DBP, mmHg | 79.27±7.77 | 76.41±8.04 | 0.5 | 78.72±7.02 | 77.38±9.30 | 0.5297 | 80.55±10.52 | 77.52±8.28 | 0.049 | ||||||||||||||||||||
| FPG, mg/dL | 165.33±47.90 | 127.96±26.98 | 0.027 | 150.9±45.99 | 121.11±30.42 | 0.0003 | 151.84±50.80 | 123.19±21.27 | 0.0024 | ||||||||||||||||||||
| PPPG, mg/dL | 222.3±81.85 | 173.27±58.65 | 0.021 | 231.62±80.88 | 176.24±61.49 | 0.0017 | 203.88±70.46 | 186.47±46.94 | 0.3 | ||||||||||||||||||||
| ALT,U/L | 38.57±21.76 | 33.56±16.43 | 0.17 | 42.16±17.56 | 30.9±11.72 | 0.0123 | 40.6±20.04 | 33.13±17.23 | 0.4548 | ||||||||||||||||||||
| CHOLESTEROL, mg/dL | 150.77±39.16 | 138.88±27.82 | 0.74 | 141.16±31.60 | 139.09±34.33 | 0.9849 | 132.09±40.70 | 129.05±33.55 | 0.4089 | ||||||||||||||||||||
| TG, mg/dL | 149±79.03 | 129.17±57.28 | 0.57 | 144.63±76.45 | 132.78±43.44 | 0.3244 | 148.77±68.55 | 143.88±64.98 | 0.2231 | ||||||||||||||||||||
| HDL, mg/dL | 40.15±8.91 | 38.57±7.91 | 0.78 | 39.03±7.14 | 39.81±9.48 | 0.5444 | 38.41±11.83 | 38.81±10.22 | 0.3723 | ||||||||||||||||||||
| LDL, mg/dL | 87.62±31.68 | 80.87±25.40 | 0.78 | 83.34±27.99 | 79.39±34.06 | 0.6436 | 72.54±27.26 | 70.6±25.26 | 0.6232 | ||||||||||||||||||||
| NON-HDL, mg/dL | 99.17±49.98 | 84.34±47.77 | 0.51 | 84.08±49.20 | 78.71±51.71 | 0.4831 | 88.87±46.26 | 79.5±44.90 | 0.0781 | ||||||||||||||||||||
| Creatinine, mg/dL | 0.84±0.25 | 0.84±0.29 | 0.47 | 0.91±0.19 | 0.91±0.22 | 0.59 | 0.95±0.18 | 0.92±0.21 | 0.4215 | ||||||||||||||||||||
| Urine ACR (mg/g) | 18.41±26.87 | 18.42±19.59 | 0.91 | 33.71±47.82 | 36.88±52.87 | 0.91 | 57.15±143.56 | 29.48±56.39 | 0.2387 | ||||||||||||||||||||
| Duration, weeks | 22±12.21 | 25.73±15.66 | 19.9±9.84 | ||||||||||||||||||||||||||
| % of patients with HbA1c <7% | 46.67 | 45 | 45.16 |
Table 6: Changes in Parameters after treatment with SGLT2 inhibitors.
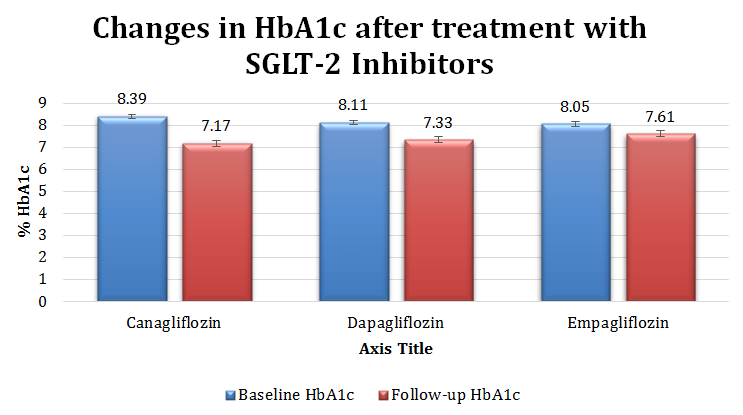
significant reduction in HbA1c values (p=0. 008 and p=0.0005 respectively) but empagliflozin failed to show statistically significant changes (p=0.65).
Chatterjee S, et al. Effects on Metabolic Parameters of Addition of SGLT‐2 Inhibitors on Patients with Type2 Diabetes Inadequately Controlled with DPP‐IV Inhibitors and Metformin. Diabetes Obes Int J 2019, 4(2): 000201.
Copyright© Chatterjee S, et al.
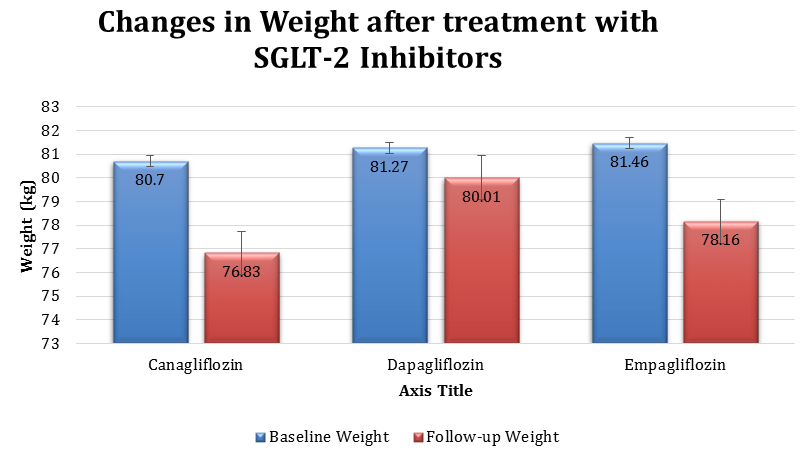
Figure 2 shows the changes in weight in the study group after treatment with SGLT-2inhibitors.When the baseline mean body weights were compared to the mean body weight at follow up all the three SGLT-2 inhibitors showed significant reduction in body weight-canagliflozin (p=0.007), dapagliflozin (p=0.002) and empagliflozin (p<0. 0001).
| [14] | . Dela |
|---|---|
| ith | HbA 1c |
There are many choices for therapy in patients with T2DM requiring treatment intensification. The rationale, mechanism, and clinical data on combination therapy with DPP-4 inhibitors and SGLT-2 inhibitors have been Chatterjee S, et al. Effects on Metabolic Parameters of Addition of SGLT‐2 Inhibitors on Patients with Type2 Diabetes Inadequately Controlled with DPP‐IV Inhibitors and Metformin. Diabetes Obes Int J 2019, 4(2): 000201.
A meta-analysis has evaluated the efficacy and safety of a combination therapy comprising a SGLT-2 inhibitor and DPP-4 inhibitor in type 2 diabetes [18]. Eight randomised controlled trials (RCT) comparing SGLT-2 inhibitor/DPP-4 inhibitor and DPP-4 inhibitor, and five RCTs comparing SGLT-2 inhibitor/DPP-4inhibitor and SGLT-2 inhibitor, with three RCTs involving both comparisons, were included in the review. SGLT-2 inhibitor/DPP-4 inhibitor resulted in a greater mean HbA1c reduction [weighted mean difference (WMD]): - 0.62%]), than did DPP-4inhibitor alone, which was a much less marked reduction (WMD: -0.35%) than with SGLT-2 inhibitor alone. Interestingly, the authors thereafter suggest that additional glucose control is significant when SGLT-2inhibitors are combined with or added to DPP-4 inhibitors but not vice versa, as was also suggested previously [19].
Copyright© Chatterjee S, et al.
| Patients receiving dapagliflozin plus saxagliptin | |||
|---|---|---|---|
| demonstrated greater improvements in glycaemic control | |||
| (ie, HbA and FBG) at week 24 than those receiving either 1c | |||
| dapagliflozin or saxagliptin alone. Furthermore, 41% of | |||
| patients achieved HbA <7% with dapagliflozin plus 1c | |||
| saxagliptinvs 18% and 22% with saxagliptin or | |||
| dapagliflozin, respectively | [20] | . |
| HbA 1c | ||
|---|---|---|
| effect of | SGLT-2 inhibitor as added on to metformin/DPP- | |
| 4 inhibitor combinations was analysed | FBG (<0.0001), |
Body weight changes little when a DPP-4 inhibitor is added to a metformin/SGLT-2 inhibitor combination but, in patients with baseline BMI 30-32kg/m2, adding the SGLT-2 inhibitor to a metformin/DPP-4 inhibitor combination is associated with weight loss of approximately 1.5-3.0kg compared with 0.3-0.4kg among placebo recipients [21, 23]. In this study there was 2.67 kg weight loss when SGLT-2 inhibitor was added to metformin/DPP-4 inhibitor combinations in the study group with mean BMI of 30.85kg/m2 and mean body weight of 81.55 kgs at baseline .This was statistically significant (p<0. 0001).
Chatterjee S, et al. Effects on Metabolic Parameters of Addition of SGLT‐2 Inhibitors on Patients with Type2 Diabetes Inadequately Controlled with DPP‐IV Inhibitors and Metformin. Diabetes Obes Int J 2019, 4(2): 000201.
Adding an SGLT-2 inhibitor to metformin/DPP-4 inhibitor is also associated with a small reduction in blood pressure of about 1.0–2.5mmHg above the effect of placebo for systolic and diastolic pressures but there is little impact when a DPP-4 inhibitor is the third drug added [21, 22, 23, 24]. In the present study in the empagliflozin treated group there was 8.17mmHgreduction of SBP (p=0.0002) and 3.03 mmHg reduction in DBP (p= 0.049).
Finally, the limitations of this study must be considered. First, this is a real world study (RWS). Randomisation and placebo controlling were not done. Secondly, due to small number of cases dose related subgroup analysis of the three SGLT-2 inhibitors couldn’t be done. Thirdly, the DPP-4 inhibitors were not individually analysed. These issues might have implication in the result and outcome of the study.
Conclusion
The present study showed addition of SGLT2 inhibitors as an add-on to DPP-4 inhibitors and metformin in inadequately controlled T2DM produce favourable effects on metabolic parameters with the advantage of weight loss. This only Indian real world study is thus consistent with RCTs and real world studies of western world.
Conflict of Interest
The authors have no multiplicity of interest to disclose.
References
-
(1990) UK Prospective Diabetes Study 7: response of fasting plasma glucose to diet therapy in newly presenting type II diabetic patients, UKPDS Group. Metabolism 39(9): 905-912.
-
Goldstein DJ (1992) Beneficial health effects of modest weight loss. Int J Obes Relat Metab Disord 16(6): 397-415.
-
Pastors JG, Warshaw H, Daly A, Franz M, Kulkarni K (2002) The evidence for the effectiveness of medical nutrition therapy in diabetes management. Diabetes Care 25(3): 608-613.
-
DeFronzo RA (2009) Banting Lecture. From the triumvirate to the ominous octet: a new paradigm for the treatment of type 2 diabetes mellitus. Diabetes 58(4): 773-795. Copyright© Chatterjee S, et al.
-
Ahrén B, Simonsson E, Larsson H, Landin-Olsson M, Torgeirsson H, et al. (2002) Inhibition of dipeptidyl peptidase IV improves metabolic control over a 4- week study period in type2 diabetes. Diabetes Care 25(5): 869-875.
-
Deacon CF (2011) Dipeptidyl peptidase-4 inhibitors in the treatment of type 2 diabetes: a comparative review. Diabetes Obes Metab 13(1): 7-18.
-
Balas B, Baig MR, Watson C, Dunning BE, Ligueros- Saylan M, et al. (2007) The dipeptidyl peptidase IV inhibitor vildagliptin suppresses endogenous glucose production and enhances islet function after single- dose administration in type 2 diabetic patients. J Clin Endocrinol Metab 92(4): 1249-1255.
-
Abdul-Ghani MA, Norton L, Defronzo RA (2011) Role of sodium-glucose cotransporter 2 (SGLT 2) inhibitors in the treatment of type 2 diabetes. Endocr Rev 32(4): 515-531.
-
Guthrie RM (2015) Clinical use of dipeptidyl peptidase-4 and sodium-glucose cotransporter 2 inhibitors in combination therapy for type 2 diabetes mellitus. Postgrad Med 127(5): 463-479.
-
Sharma MD (2015) Potential for combination of dipeptidyl peptidase-4 inhibitors and sodium-glucose co-transporter-2 inhibitors for the treatment of type 2 diabetes. Diabetes Obesity Metab 17(7): 616-621.
-
Abdul-Ghani M (2015) Where does combination therapy with an SGLT2 inhibitor plus a DPP-4 inhibitor fit in the management of type 2 diabetes? Diabetes Care 38(3): 373-375.
-
DeFronzo RA, Eldor R, Abdul-Ghani M (2013) Pathophysiologic approach to therapy in patients with newly diagnosed type 2 diabetes. Diabetes Care 36(S2): S127-S138.
-
Neumiller JJ (2014) Efficacy and safety of saxagliptin as add-on therapy in type 2 diabetes. Clin Diabetes 32(4): 170-177.
-
Engel SS, Seck TL, Golm GT, Meehan AG, Kaufman KD, et al. (2013) Assessment of AACE/ACE recommendations for initial dual antihyperglycemic therapy using the fixed-dose combination of sitagliptin and metformin versus metformin. Endocr Pract 19(5): 751-757. Chatterjee S, et al. Effects on Metabolic Parameters of Addition of SGLT‐2 Inhibitors on Patients with Type2 Diabetes Inadequately Controlled with DPP‐IV Inhibitors and Metformin. Diabetes Obes Int J 2019, 4(2): 000201.
-
Khunti K, Wolden ML, Thorsted BL, Andersen M, Davies MJ (2013) Clinical inertia in people with type 2 diabetes: a retrospective cohort study of more than 80,000 people. Diabetes Care 36(11): 3411-3417.
-
Fu AZ, Qiu Y, Davies MJ, Radican L, Engel SS (2011) Treatment intensification in patients with type 2 diabetes who failed metformin monotherapy. Diabetes Obes Metab 13(8): 765-769.
-
Paul SK, Klein K, Thorsted BL, Wolden ML, Khunti K (2015) Delay in treatment intensification increases the risks of cardiovascular events in patients with type 2 diabetes. Cardiovasc Diabetol 14: 100.
-
Cho YK, Kang YM, Lee SE, Lee J, Park JY, et al. (2018) Efficacy and safety of combination therapy with SGLT2 and DPP4 inhibitors in the treatment of type 2 diabetes: a systematic review and meta-analysis. Diabetes Metab 44(5): 393-401.
-
Scheen AJ (2016) DPP-4 inhibitor plus SGLT-2 inhibitor as combination therapy for type 2 diabetes: from rationale to clinical aspects. Expert Opin Drug Metab Toxicol 12(12): 1407-1417.
-
Rosenstock J, Hansen L, Zee P, Li Y, Cook W, et al. (2015) Dual add-on therapy in type 2 diabetes poorly controlled with metformin monotherapy: a randomized double-blind trial of saxagliptin plus dapagliflozin addition versus single addition of saxagliptin or dapagliflozin to metformin. Diabetes Care 38(3): 376-383.
-
Mathieu C, Ranetti AE, Li D, Ekholm E, Cook W, et al. (2015) Randomized, double-blind, phase 3 trial of triple therapy with dapagliflozin add-on to saxagliptin plus metformin in type 2 diabetes. Diabetes Care 38(11): 2009-2017.
-
Matthaei S, Catrinoiu D, Celiński A, Ekholm E, Cook W, et al. (2015) Randomized, double-blind trial of triple therapy with saxagliptin add-on to dapagliflozin plus metformin in patients with type 2 diabetes. Diabetes Care 38(11): 2018-2024.
-
Søfteland E, Meier JJ, Vangen B, Toorawa R, Maldonado-Lutomirsky M, et al. (2017) Empagliflozin as add-on therapy in patients with type 2 diabetes inadequately controlled with linagliptin and metformin: a 24-week randomized, double-blind, parallel-group trial. Diabetes Care 40(2): 201-209. Copyright© Chatterjee S, et al.
-
Tinahones FJ, Gallwitz B, Nordaby M, Götz S, Maldonado-Lutomirsky M, et al. (2017) Linagliptin as add-on to empagliflozin and metformin in patients Chatterjee S, et al. Effects on Metabolic Parameters of Addition of SGLT‐2 Inhibitors on Patients with Type2 Diabetes Inadequately Controlled with DPP‐IV Inhibitors and Metformin. Diabetes Obes Int J 2019, 4(2): 000201. with type 2 diabetes: Two 24-week randomized, double-blind, double-dummy, parallel-group trials. Diabetes Obes Metab 19(2): 266-274. Copyright© Chatterjee S, et al.
- Investigation of Polymorphisms in PPAR-Ɣ and TRHR Genes and their Impact on Turkish Diabetic and Obese Individuals
- The Impact of Aircraft Noise Exposure on the Efficacy of Empagliflozin Therapy in an Animal Model of Obesity
- Rooibos Mitigates Metabolic and Inflammatory Dysfunctions in Mice Fed a High-Carbohydrate Diet
- Synergistic Effect of Combined Leaf Extract of Vernonia amygdalina, Ocimum gratissimum, and Zingiber officinale Tuber on Phytochemical Profile, Antioxidant Activity, Serum Insulin, and Biochemical Parameters in Streptozotocin-Induced Diabetic Rats
- Investigation of Cardiovascular Responses to Aerobic Exercise in Obese University Students
- A Look at the Phase Angle Obtained by Electrical Bioimpedance