Weight Loss through Vinyasa Flow Yoga - A Pilot Feasibility Study in Singapore
Obesity has become an increasing concern in the world and has also become a public health threat in many countries. Governments and private sectors are working hard to develop various strategies to assist people to have a better control over their health. Regular exercise, which is part of a healthy lifestyle help to improve cardiovascular health, leading to weight loss and hence prevention of certain potential illnesses. Yoga, being one of the physical exercises, promotes body’s natural harmony and functional balance, which in turn, helps individuals to live a better life. This paper outlines the pilot study conducted in Singapore to investigate the effects of Vinyasa Flow Yoga coupled with Pranayama on the weight-related outcomes in adults, in particular, reduction of body weight and body fat percentage. The results show that weekly Yoga practices impose positive results on the reduction of body weight and fat percentage, and hence can be considered essential for a healthy lifestyle.
Introduction
Over the years, obesity is seen to be an increased phenomenon across the world, where, since the millennium, obesity is said to be a national health threat and a major public health challenge, with approximately 72.5 million adults in the United States categorised as obese [1]. Further to that, obesity is not only an adult issue but also observed in children, where it has been reported that 23.8% of boys and 22.6% of girls are obese in the developed countries, while for the developing countries, the percentage of obese boys and girls are 12.9% and 13.4%, respectively [2]. For the case of Singapore, it is reported that 25.6% of Singaporean as considered to be overweight, while 6.8% of Singaporeans are obese [3, 4, 5]. Looking at the condition that is being observed currently, it is projected that almost half of the world’s adult population will be overweight or obese by 2030 [6]. In the same paper, it is also mentioned that 5% of all deaths in the world is caused by obesity, and the economic impact that is caused by obesity is as high as that of smoking and armed conflict, where a total amount of $2.0 trillion, $2.1 trillion and $2.1 trillion are spent in dealing with obesity, smoking and armed conflict, respectively.
As defined by the Centers of Disease Control and Prevention (CDC) [1], one is considered as obese when his/ her body mass index (BMI) is 30 or higher and overweight when the BMI is between 25 to 29.9. The condition of overweight has proven to be a cause for various diseases. The study has shown that overweight in men and women is closely linked to type 2 diabetes [7]. Also, compared to Caucasians, Asians are said to be at higher risk to develop diabetes and heart disease when the BMI reading is equal or more than 23 due to higher body fat contents (Ministry of Health M., Why is being obese a problem? 2018). Individuals with a BMI of higher than 27.5 possess higher chances to develop these diseases.
The major and independent risk factor for most of the cardiovascular diseases (CVD) is obesity, especially visceral obesity. Generally, obesity is associated with low-grade inflammation and endothelial dysfunction which are the main starting points of CVD and when such inflammation is not catered to, then, it leads to chronic inflammation as seen in most CVD cases. Several studies have shown that obesity impairs the endothelial function and levels of endothelin-1 (ET-1) which is a potent vasoconstrictor, are higher in such cases. Further to that, ET-1 is capable of both initiating and progressing coronary atherosclerosis.
In fighting issues about overweight or obesity, [6] highlighted that “No single solution creates sufficient impact to reverse obesity: only a comprehensive, systemic program of multiple interventions is likely to be effective.” Governments, as well as private sectors, have been putting efforts to develop various intervention strategies, such as the provision of weight management guidelines, or health programmes such as National Step ChallengeTM that is carried out with support from the Ministry of Health in Singapore. Such interventions aim to assist individuals to lose weight or prevent weight gain. Mobile applications are also created to assist mobile phone users to maintain a healthy lifestyle, for instance, Healthy 365 app, ActiveSG App and NUH myMeds [3].
It has been known that regular exercise and a controlled diet contribute to a healthy lifestyle. Besides, the frequent exercises also lead to improved cardiovascular health, returns the blood pressure cholesterol to the normal level [8]. On top of that, there are also studies that show that exercises act as a non-pharmacologic treatment option for disturbed sleep [9], produces an anxiolytic effect within the body [10], and even enhance self-esteem [11].
Continuous researches have been carried out to look into the relationship between physical exercises and weight loss, and Yoga, being one of the physical exercises, comprises of meditation, pranayama (control of breathing), asanas (postures) and relaxation [12], promotes natural harmony and functional balance in the organ systems leading to a better health condition.
Some other studies reveal that the practice of Yoga not only aids in weight reduction but also reduces blood pressure, glucose level and high cholesterol [13]. However, the study also stressed that this is through the long-term examination of the individuals, and there are not enough studies to address if Yoga aids the reduction of high risk for diabetes and its related common health problems. The argument of long-term examination and practices is also supported by the paper of Kristal, et al. [14], wherein it was reported that middle-aged men and women found that the reduction of weight is more evident for those who practice Yoga for four years or more, emphasising that weight loss is a long term goal and process and not to be aimed to be achieved in only a few months. We may see the initial results in a few months, but the continuous effort is required to maintain such a loss. Although there are article claims that the weight management through yoga is based on the mechanism that the practice of yoga enhanced mindfulness and energy expenditure while reducing the body pain, but the exact mechanism underlying Yoga’s effectiveness is still yet to be examined in detail [15].
However, the participants in the above-mentioned studies were mostly women, for instance, about 75 – 79% of the respondents in the research of Ross, et al. (2013) [16] and Flegal, et al. [17] are women while it is reported that the study of Vartanian & Wharton [18], McIvera, et al. [17] and Badawy & Natiq [20] comprised of 100% women. Hence, there is insufficient information about the effect on the benefits of yoga on men.
Throughout different studies, various types of yoga are adopted as part of the study, while there are some papers that do not specify the type of yoga that is being practised (i.e., only the word Yoga is used in the paper), generally, Yoga practices adopted by various researchers include Iyengar Yoga [17, 21], Ashtanga Yoga [22] or Hatha Yoga [19].
However, it has been noted that the practice of Yoga also helps to generate mindfulness among the individuals, which in turn makes them more aware on their daily life, that is, to be more mindful eating and exercising, and eventually achieving the weight loss. Some papers agree in this statement, including [21] and [23], who also agree that we do not possess much understanding towards how mindfulness is practised in terms of eating and weight management, as there are too many complicating factors in this analysis, including various definitions of mindfulness by different individuals.
This pilot research is established to investigate the effects of Vinyasa Flow Yoga on the weight-related outcomes in adults in Singapore, especially the reduction in body weight and body fat percentage.
Methodology
Sample Size
The sample for the actual projected study can be calculated through the “OpenEpi” software version 3, using the Kelsey et al, formula which gives a sample of about 318 for a confidence interval of 95%. Based on the study by Treece and Connelly the suggested sample size for a pilot study should be 10% of the sample size planned for the actual projected study, which in this case would yield about 30-32 participants as the sample size. For research in the field of medical studies, both Hill and Isaac & Michael suggested that the sample size for a pilot study should be in the range of 10- 30. Based on these justifications, the estimated sample size for this pilot study was 30 participants aged 20 to 50 and consisting of different genders and races.
Inclusion and Exclusion Criteria
In order to be included in the study, the consenting participants must be adults working full-time (about 35- 44 hours a week). The age range for adults would be as per the WHO guidelines: 20-50 years of age (WHO 2019, WHO 2019a). Participants are also expected to attend at least one 60-minute Yoga class per week. The exclusion criteria for this study are as follows: participants who practice yoga for less than 60 minutes per week; participants who work part-time (less than 35-44 hours per week) and participants who are not willing to share the body composition measurement data.
Methods
The participants who meet the inclusion criteria and who have consented to participate in the study after going through the full details provided in the participant information statement, were requested to complete a set of questionnaires that would enable the researchers to determine the demographics of the study population and to record the frequency of yoga classes attended, other physical activities, types of diet and typical daily schedule of the study participants.
Soon after completing the questionnaires, the body composition measurement which includes the body weight and body fat measurements of the study participants were taken using appropriate scales and recorded as the baseline body composition data. As the study participants went through their regular Vinyasa flow yoga classes over the study period, the body composition measurements were taken once every six weeks for three times and recorded.
A typical Vinyasa Yoga class included the following components: the class started with the centering, where pranayama is practised. This was then followed by warm- ups and Sun Salutations. The energising asanas were mainly standing asanas while calming asanas were mainly sitting and supine asanas. The asanas included twists, backbends, forward folds and arm balances. All asanas were basic, which is suitable for all levels of practitioners, and inversions, shoulder stand and headstand asanas were not considered here.
Statistical Analysis
The data collected over the study period of 4.5 months was recorded and the results were summarized by descriptive statistics such as mean and standard deviation. The effect size which is defined as the mean difference between baseline and every follow-up was reported with a 95% confidence interval. Statistical significance was assessed by paired t-test. Finally, an AIC based stepwise multivariate mixed-effects regression model was fitted to estimate the effect sizes across the follow-ups after adjusting the set of covariates selected by the algorithm. The statistical software R version 3.6.2 [24] was used for statistical analysis.
Results and Discussions
Demographics
About 60% of the study population were males and the remaining females and 40% of them were Chinese, followed by 27% of Indians and 23% Europeans. In terms of age distribution, 40% of the study population belonged to the age group 31 to 40 years and the remaining participants were equally distributed between the age groups of 20-30 years and 41 to 50 years (Table 1).
| Variables | Groups | Number | Percentage |
|---|---|---|---|
| Gender | Male | 18 | 60.00% |
| Gender | Female | 12 | 40.00% |
| Total | 30 | 100.00% | |
| Races | Chinese | 12 | 40.00% |
| Races | Indian | 8 | 26.67% |
| Races | European | 7 | 23.33% |
| Races | Others | 3 | 10.00% |
| Total | 30 | 100.00% | |
| Age | 20 – 30 | 9 | 30.00% |
| Age | 31 – 40 | 12 | 40.00% |
| Age | 41 – 50 | 9 | 30.00% |
| Total | 30 | 100.00% |
Table 1: Demographic information of the Participants.
From the data obtained, the mean age of the sample was recorded as 34.05 ± 9.06 years old, with males registered at a mean of 33.52 ± 9.07 years old and females registered at 34.53 ± 9.10 years old. The first measurement was taken at the beginning of the test period, and this is regarded as the baseline measurement. Subsequently, three follow-up measurements F1, F2 and F3 were taken.
BMI
With the definition of the Body Mass Index (BMI) guidelines provided by the CDC (CDC, 2000), a person is considered as overweight if the BMI is more than or equal to 25.0 kg/m2, and is considered at obese if the BMI is recorded as more than or equal to 30.0 kg/m2. At the baseline measurement, 9 participants (30%) of the participants were overweight, while 1 (3.33%) was obese. After three rounds of follow-up measurements, 29 participants showed a reduction in the BMI index, while one participant showing maintenance of the BMI value. Worth noting, among the participants who were overweight and obese, it was recorded that 2 participants had the BMI dropped from overweight to normal, and the obese participant also had the BMI dropped from obese to overweight.
Bodyweight and Body Fat
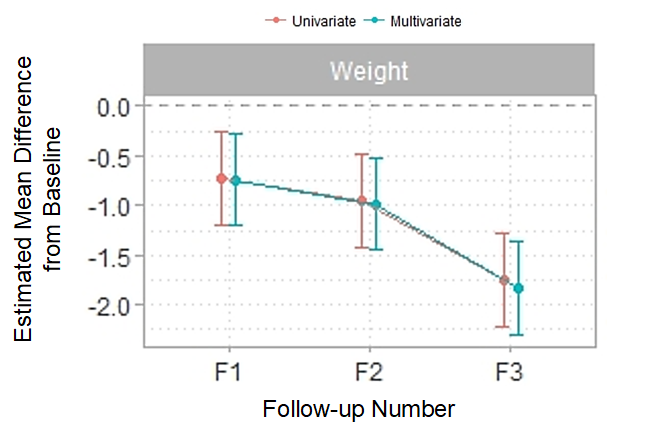
In terms of the observation of body weight and body fat percentage, two types of analyses were performed, namely univariate and multivariate analyses. Figure 1 and Table 2 show the comparison of the estimated mean difference in the weight of the samples measured against the baseline for three follow-up measurements. On the baseline measurement, the mean weight for male and female participants was 74.33 ± 9.78 and 59.16 ± 6.32 kg, respectively. Generally, all participants were showing a decreasing pattern from the baseline measurement to F3 follow-up measurement. Looking at both Table 2 and Figure 1, the results have indicated a decrease in the weight of the participants.
| Follow-up | n | Mean | SD | EffectSize | P-value |
|---|---|---|---|---|---|
| Baseline | 30 | 65.23 | 10.81 | ||
| 1 | 30 | 64.51 | 10.36 | -0.72(-1.19,-0.25) | 0.003 |
| 2 | 30 | 64.28 | 10.71 | -0.95(-1.42,-0.48) | <0.001 |
| 3 | 30 | 63.49 | 10.57 | -1.74(-2.21,-1.27) | <0.001 |
Table 2: Details of mean, standard deviation and P-value for the weight measurements of 30. participants.
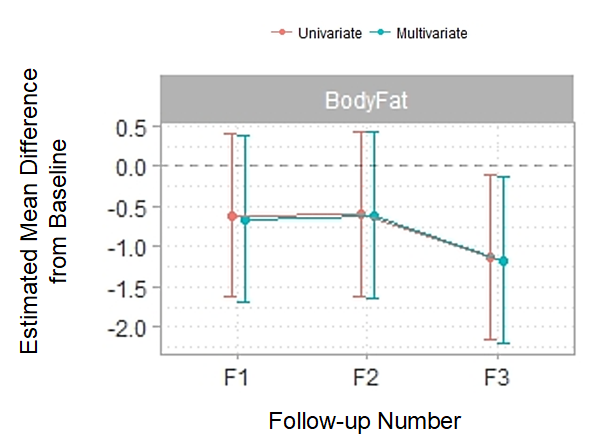
On the other hand, Table 3 and Figure 2 shows the details of the baseline measurement after three follow-up measurements of body fat percentage. At the baseline measurement, the body fat percentage among male participants was 24.59 ± 7.54 %. This value was then dropped to 24.43 ± 7.15 % on the third follow-up measurement. On the other hand, the body fat percentage for female participants were registered to be 30.76 ± 4.47 % at the baseline measurement, which was then 29.83 ± 4.69 %. Based on the guidelines provided by the American Council on Exercise (ACE), the acceptable body fat percentage for men and women are given as 18 – 24 % and 25 – 31 %, respectively. The results show that the participant’s average body fat is considered as acceptable even though the range is close to obesity. The positive note to observe in this reading is that these values of body fat percentage were both further reduced at the end of the measurement period.
| Follow-up | n | Mean | SD | EffectSize | P-value |
|---|---|---|---|---|---|
| Baseline | 30 | 28.29 | 6.54 | ||
| 1 | 30 | 27.67 | 6.29 | -0.62(-1.63,0.4) | 0.232 |
| 2 | 30 | 27.69 | 6.01 | -0.6(-1.61,0.42) | 0.247 |
| 3 | 30 | 27.16 | 6.40 | -1.13(-2.15,-0.11) | 0.03 |
Table 3: Details of mean, standard deviation and P-value for the weight measurements of 30 participants.
The results coincide with the findings of Rioux & Ritenbaugh [25], where, through clinical trials, the practice of Yoga has shown improvements in some medical conditions that are related to obesity, including the reduction of BMI, body fat, body weight and waist circumference. These reductions in body weight and body fat also supports the arguments by Ross, et al. [21], where an improvement in the diet and body weight was observed for those individuals who practice yoga [26].
Conclusion
This pilot feasibility study clearly indicates the possibility of not only bodyweight loss but also a potential reduction in the body fat with regular practice of Vinyasa flow yoga. As highlighted in this paper, reduction in body weight and body fat can also decrease the occurrences of other serious diseases such as cardiovascular diseases and diabetes. This study also reveals that bodyweight reduction is feasible not only in women who practice Vinyasa flow yoga but also in men as the majority of the study participants were males. This study can be further extended to the actual projected sample size in order to further validate the results obtained in the pilot study.
Acknowledgement
The authors would like to thank the UON Singapore Pte. Ltd. for funding this project through the UON Singapore’s Small Research Project Grant.
References
-
CDC (2000) Vital signs: state-specific obesity prevalence among adults-the United States, 2009. Morbidity and Mortality Weekly 59(30): 1-5.
-
Ng M, Fleming T, Robinson M, Thompson B, Graetz N (2014) Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 384(9945): 766-781.
-
My Health (2018) Apps Listing. Ministry of Health.
-
(2018) How does obesity affect my health? Ministry of Health.
-
(2018) Why is being obese a problem? Ministry of Health.
-
Dobbs R, Sawers C, Thompson F, Manyika J, Woetzel J, et al. (2014) Overcoming obesity: An initial economic analysis. McKinsey Global Institute.
-
Sullivan P, Morrato E, Ghushchyan V, Wyatt H (2005) Obesity, inactivity, and the prevalence of diabetes and diabetes-related cardiovascular comorbidities in the U.S.,2000-2002. Diabetes Care 28(7): 1599-1603.
-
Brown W, Mishra G, Lee C, Bauman A (2000) Leisure time physical activity in Australian women: relationship with well-being and symptoms. Research Quarterly for Exercise and Sport 71(3): 206-216.
-
Kline C (2014) The Bidirectional Relationship Between Exercise and Sleep: Implications for Exercise Adherence and Sleep Improvement. American Journal of Lifestyle Medicine 8(6): 375-379.
-
Fetzner M, Asmundson G (2015) Aerobic Exercise Reduces Symptoms of Posttraumatic Stress Disorder: A Randomized Controlled Trial. Cognitive Behaviour Therapy 44(4): 301-313.
-
Martin K, Lichtenberger C (2002) Fitness enhancement and body image change. In: Cash TTF, (Ed.), Body images: A handbook of theory research, and clinical practice, Guilford Press, New York, 47: 414-421.
-
Nayak N, Shankar K (2004) Yoga: a therapeutic approach. Physical Medicine and Rehabilitation Clinics of North America 15(4): 783-798.
-
Yang K (2007) A Review of Yoga Programs for Four Leading Risk Factors of Chronic Diseases. Evidence- Based Complementary and Alternative Medicine 4(4): 487-491.
-
Kristal A, Littman A, Benitez D, White E (2005) Yoga practice is associated with attenuated weight gain in healthy, middle-aged men and women. Alternative Therapy and Health Medicine 11(4): 28-33.
-
Bernstein A, Bar J, Ehrman J, Golubic M (2014) Yoga in the management of overweight and obesity. American Journal of Lifestyle Medicine 8(1): 33-41.
-
Ross A, Friedmann E, Bevans M, Thomas S (2013) National survey of yoga practitioners: mental and physical health benefits. Complementary Therapies in Medicine 21(4): 313-323.
-
Flegal K, Kishiyama S, Zajdel D, Haas M, Oken B (2007) Adherence to yoga and exercise interventions in a 6-month clinical trial. BMC Complementary and Alternative Medicine 7: 37.
-
Vartanian L, Wharton C (2012) Appearance vs. health motives for exercise and for weight loss. Psychology of Sport and Exercise 13: 251-256.
-
McIvera S, O’Halloranb P, McGar M (2009) Yoga as a treatment for binge eating disorder: A preliminary study. Complementary Therapies in Medicine 17(4): 196-202.
-
Badawy H, Natiq G (2014) Effects of daily workout on agility, flexibility and reduced the weight among the Iraqian women. Science, Movement and Health 14(1): 73-77.
-
Ross A, Brooks A, Touchton-Leonard K, Wa G (2016) A Different Weight Loss Experience: A Qualitative Study Exploring the Behavioral, Physical, and Psychosocial Changes Associated with Yoga That Promote Weight Loss. Evidence-Based Complementary and Alternative Medicine, pp: 1-11.
-
Benavide S, Caballero J (2009) Ashtanga yoga for children and adolescents for weight management and psychological well-being: An uncontrolled open pilot study. Complementary Therapies in Clinical Practice 15(2): 110-114.
-
Tapper K (2017) Can mindfulness influence weight management related eating behaviors? If so, how? Clinical Psychology Review 53: 122-134.
-
R Core Team (2019) R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria.
-
Rioux J, Ritenbaugh C (2013) Narrative review of yoga intervention clinical trials including weight-related outcomes. Alternative 19(3): 32-46.
-
ABET (2019) History of ABET.
- Investigation of Polymorphisms in PPAR-Ɣ and TRHR Genes and their Impact on Turkish Diabetic and Obese Individuals
- The Impact of Aircraft Noise Exposure on the Efficacy of Empagliflozin Therapy in an Animal Model of Obesity
- Rooibos Mitigates Metabolic and Inflammatory Dysfunctions in Mice Fed a High-Carbohydrate Diet
- Synergistic Effect of Combined Leaf Extract of Vernonia amygdalina, Ocimum gratissimum, and Zingiber officinale Tuber on Phytochemical Profile, Antioxidant Activity, Serum Insulin, and Biochemical Parameters in Streptozotocin-Induced Diabetic Rats
- Investigation of Cardiovascular Responses to Aerobic Exercise in Obese University Students
- A Look at the Phase Angle Obtained by Electrical Bioimpedance