Dual burden of Tuberculosis (TB) and Diabetes Mellitus (DM) as the major risk factor for wide range of population
The bidirectional association between tuberculosis (TB) and diabetes mellitus (DM) creates a dual burden of these diseases globally. DM patients have chronic infections more often than those without DM and one of the possible causes is a compromised immune system that can lead to various persistent infections. This correlation creates special attention and thus the detailed study of the human immune system and needs to develop some good strategies for the prevention of diabetes in patients who are exposed to Mycobacterium tuberculosis (MTB). Both diseases are negatively affecting each other as patients taking diabetic drugs may interact with Anti TB drugs which may decrease the efficiency of drugs and on the other side patients having tuberculosis may be prone to hyperglycemic condition. In this mini-review, we tried to describe the bidirectional association of TB and DM’ and possible mechanisms by which a diabetic patient develops active TB and TB patients develop DM. Reducing diabetes could potentially reduce individual-level risks of TB and ultimately prevent increases in TB population incidences.
Introduction
Tuberculosis (TB) is a contagious airborne disease caused by Mycobacterium tuberculosis H37Rv (MTB) that mostly affects the lungs called pulmonary TB, but also can affect the bones and occasionally other organs having extremely vascular areas such as lymph nodes, kidneys, spine and eyes known as extra-pulmonary TB [1, 2]. In most of the people, infection with MTB is latent TB. However, the infection has the potential to develop into active TB at any time, and persons with active TB become sources of new infections [3]. Despite intensified global efforts of cases of TB worldwide increasing. According to the world health organization (WHO) report 2019, estimates that in 2018, there were about 10.0 million (range 9.0-11.1 million) develops TB disease and globally 1.2 million (range, 1.2-1.3 million) TB deaths have been reported. Among 10.0 million people 57% male, 32% female and 11% youngster suffering from TB disease. Globally, 1.2 million (range, 1.2-1.3 million) TB deaths occur among human immunodeficiency virus (HIV) uninfected population and 251,000 additional deaths reported in HIV infected population [4]. Several studies also demonstrated a bilabial relationship between diabetes mellitus (DM) and the occurrence of TB disease [5].
DM is a health condition in which the body does not produce enough insulin, or does not properly respond to it and leads to high blood sugar levels over a prolonged period. There are two main types of diabetes: Type 1 DM and Type 2 DM. Type 1 DM occurs because of the insulin-producing cells of the pancreas are damaged while Type 2 DM, the pancreas makes insulin, but it either doesn’t produce enough, or the insulin does not work properly. A number of studies have compared the occurrence of TB risk associated with type 1 and type 2 DM separately. These finding suggest that type 1 DM has a stronger association with TB than type 2 DM [6, 7]. DM patients have infections more often than those without DM and one of the possible causes is a compromised immune system that can lead to various persistent infections [8]. The WHO estimates that as many as 346 million people suffer from diabetes globally. An association between DM and TB outcomes and the burden of TB patients with DM globally would suggest that diabetes could increase the number of people infected by a source case and the number of patients needing enhanced anti-TB treatment [9]. The effect of DM on the development and severity of TB’ and the complex interrelations between nutrition, obesity, diabetes, and TB remain challenging issue in the public health and the clinical medicine and represents a global health risk [10, 11].
Probable Mechanisms of the Association between DM and TB
People with DM are much more vulnerable to the infection, or development of latent infection to active TB. The accurate mechanisms by which DM influences to TB are still ambiguous. Compromised Immune System DM is known to affect chemotaxis, phagocytosis, activation, and antigen presentation by phagocytes leads to weakening immune response [12]. DM hampers cell- mediated immunity and has been associated with low level of leucocytes, polymorphonuclear neutrophils (PMNs), and a decreased T-helper1 cytokine response to TB [13]. The phagocytotic capacity of PMNs is lower in diabetic patients compared to normal persons. Macrophages also play a crucial role in the pathogenesis of TB, being the primary site of infection. Macrophage cells are able to kill the bacteria. The function of macrophages is repressed in people with DM [14]. Production of Reactive oxygen species (ROS) and phagocytic and chemotactic abilities are also impaired in diabetic patients [15].
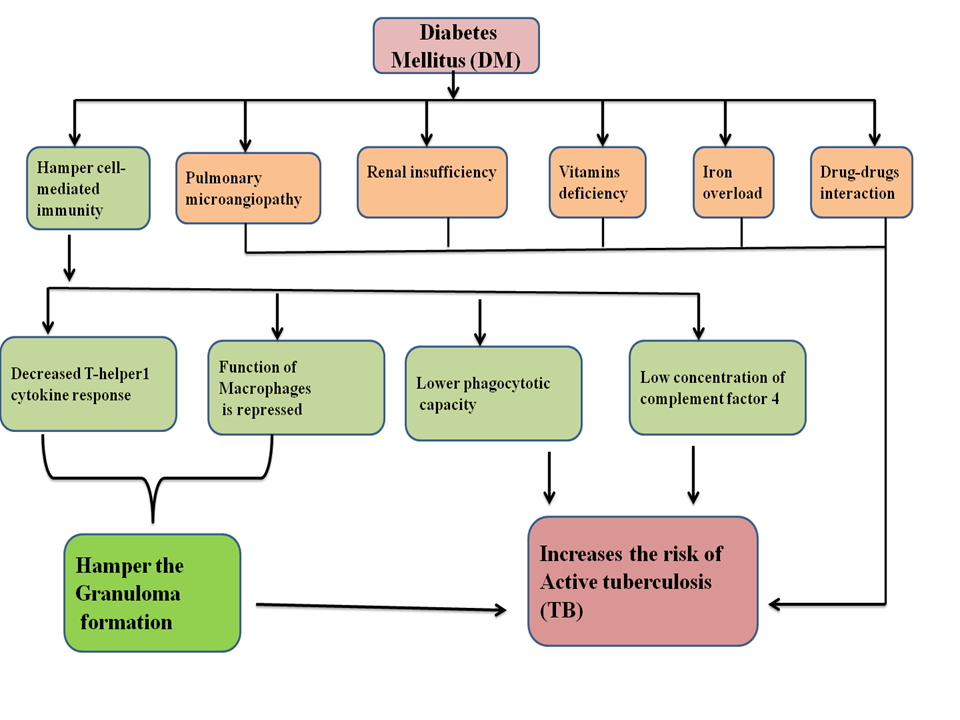
Figure 1: Factors endorsing TB in DM: DM leads to development of latent to active TB having enhanced pathogenicity and compromised immune system. This causes loss in self-defense, pulmonary microangiopathy, renal insufficiency, deficiency of micronutrients and the interaction of anti-TB drug with antidiabetic drugs causing decreased therapeutic index of TB.
Activated macrophages also produce nitric oxide (NO), an important step to eradicate TB infection, but it has been reported that activation of macrophages also impaired in TB–DM [16]. DM patients have impaired PMNs and T-helper1 which may play an important role in the inhibition of TB infection by cytokines production and granuloma formation. Granuloma is a mass of cells that forms when the immune system tries to fight off a harmful substance but cannot remove it from the body; ultimately it inhibits spreading of mycobacterium [17]. Cytokines produced by T-helper 1 (Th1) such as Interferon Gamma (IFN-γ) and Tumor necrosis factor-alpha (TNFα) are important for fighting microbial infection by activating macrophages [18]. DM is known to be associated with chronic inflammation, which would be expected to interfere with efficient immune signaling and reduced Th1 response [19]. All of these DM patients who have a depressed immune system would possibly cause a higher risk of developing TB. (Figure 1).
Complement system is also the component of immune system that improves the ability of antibodies and phagocytic cells eradicate out microbes and damaged cells from an organism endorses inflammation, and attack the pathogen’s plasma membrane. In the complement system once signal generated, initiate a cascade of reaction which would cleave the proteins, involved in the complement pathways, to convert them from inactive (proproteins) to active form. The proteins involved in the complement system are called Complement proteins or complement factors. There are mainly nine complement factors known as namely C1, C2, C3,…..C9. It has been reported that the concentration of complement factor 4 (CR-4) is lower than the normal range in DM patients, which increases the risk of infections [20].
Pulmonary Microangiopathy
Long term DM causes the pulmonary microangiopathy where high blood glucose levels cause the blood vessels to take in more glucose than normal in endothelial cells lining. Glycoproteins formation is increased on the surface of the cells and causes the basement membrane in the vessel wall to grow abnormally thicker and weaker [21]. Pulmonary microangiopathy is a serious hurdle of DM that may account for part of the increased susceptibility of people with DM to TB infection and alter its clinical presentation [22].
Renal Insufficiency
Chronic renal failure (CRF) is the permanent deterioration of renal function that gradually progresses to end-stage renal disease (ESRD). It is also a common complication of DM which strongly associated with an increased risk of TB.
Incidences of TB are increased in patients with ESRD as in comparison with the general population. CRF patients are vulnerable to TB, especially to atypical tuberculosis outside the lung (Extra-pulmonary TB), although the underlying mechanisms are fully not understood [10, 21, 23].
Vitamins Deficiency
DM can be stated as a metabolic disorder which along with TB is often associated with malnutrition. Micronutrients act as a cofactor or part of many enzymes that may play a crucial role in the control and development of DM. Low concentrations of micronutrients may also affect host defense. TB patients commonly suffer from deficiencies in nutrients such as Zinc, vitamins A, C, and D, which are fundamental to the integrity of the immune response, especially the host’s immune response against mycobacterium. Patients having zinc-deficiency have severe immune dysfunctions, mostly affects T helper cells. This also adversely affects activation of many zinc-dependent enzymes and transcription factors. Some studies reported that in HUT-78 cell lines in gene expression of interleukin-2 (IL-2) and IL-2 receptor α (IL- 2Rα) were due to decreased activation of nuclear factor-κB (NF-κB) in zinc deficient cells. Decreased NF-κB activation in HUT-78 due to zinc deficiency was due to decreased binding of NF-κB to DNA, decreased level of NF-κB mRNA, decreased κB inhibitory protein (IκB) phosphorylation, and decreased inhibitor κB kinase (IKK). Decreased NF- κB activation leads to decreased gene expression and generation of pro-inflammatory cytokines such as TNF-α, IL- 1β, and IL-8. The exact mechanism by which vitamin C play important role on lymphocytes is less clear, but it has been shown that it enhance the differentiation and proliferation of B- and T-cells, probably due to its gene regulating effects. Vitamin C deficiency causes impaired immunity and higher susceptibility to infections. Vitamin A is an antioxidant as well as anti-inflammatory vitamin that plays regulatory role in cell mediated immune response as well as in humoral immune responses. Numerous current studies in different populations have demonstrated that vitamin D deficiency increases the risk of tuberculosis. Vitamin D regulates β cell function in pancreatic islets, insulin activity, and the levels of systemic inflammation [10, 24, 25, 26].
Iron Deficiency and Overload
Iron deficiency is the most common cause of anemia, a common accessory to diabetes, this leads to many chronic infections, including TB, which are highly prevalent. Iron is a necessary nutrient for both host and mycobacteria that plays an essential role in host immunity and mycobacterial growth. It has been reported that iron overload in black Africans might be a possible risk factor for death from hepatocellular carcinoma and for death from tuberculosis [27, 28] (Figure 1).
Dose TB cause DM?
TB does not cause DM directly but it may unmask those at risk of DM in the future. TB is also associated with glucose intolerance and hyperglycemia, both of which resolve automatically with TB treatment. Long-time TB treatment causes impairment of blood glucose level is an instance of stress-induced hyperglycemia, will usually improve during TB treatment [29, 30]. During TB infection, proinflammatory cytokines (IL-1, IL-6 and TNFα) may cause an increase in insulin resistance and decreased insulin production, thereby leading to hyperglycemia. Apart from this, Anti TB drugs Isoniazid and Rifampin have hyperglycemic effects. Rifampin directly doesn’t affect the metabolism of insulin, it encourages the metabolism and decreases blood level of sulfonylureas (an antidiabetic drug), leading to hyperglycemia (Figure2).
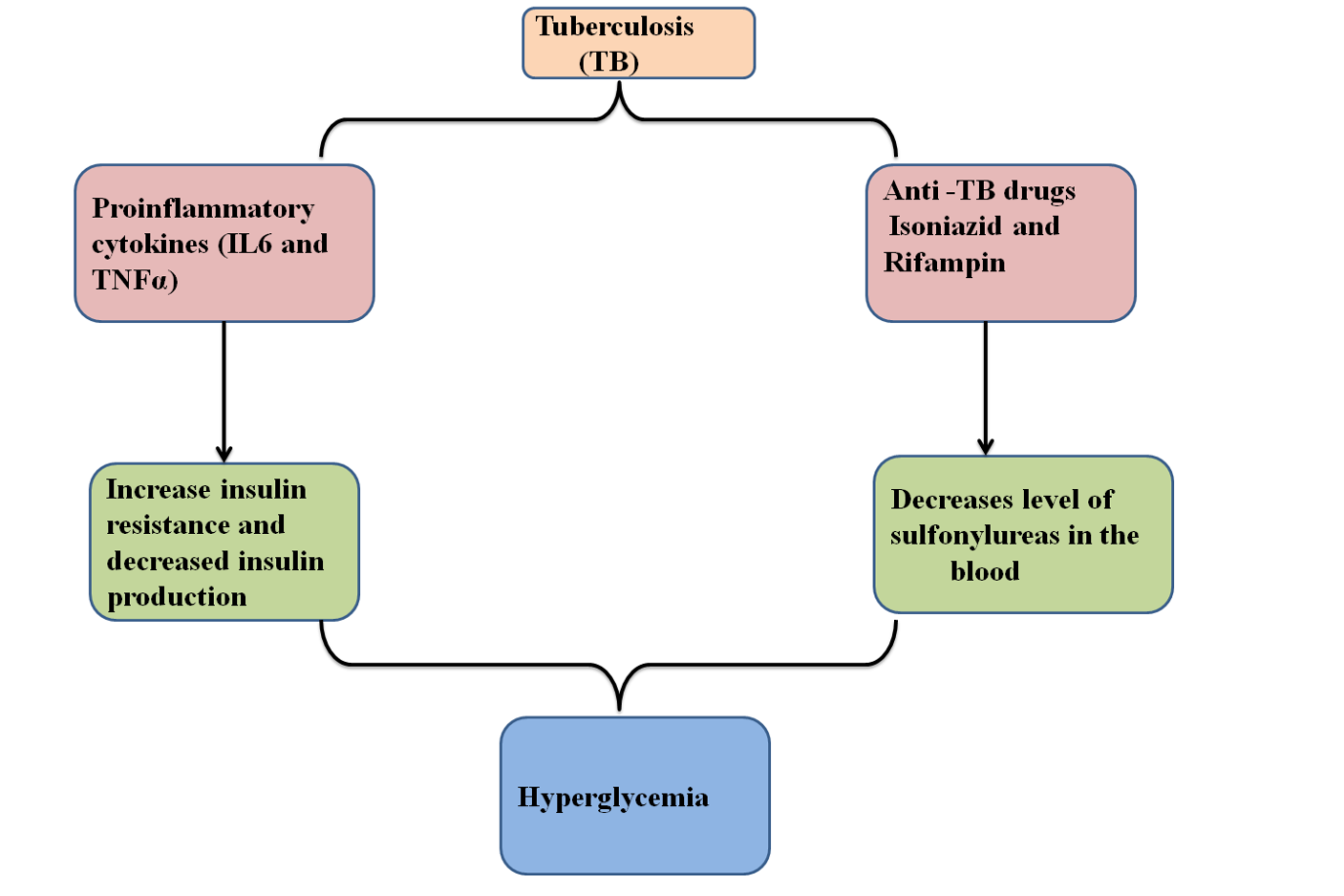
Figure 2: Allegation of TB on DM: MTB infected macrophages start to secrete proinflammatory cytokines to eradicate MTB. Proinflammatory cytokines (TNF-alpha and IL-6) somehow accelerate the insulin resistance and inhibits the insulin production. Anti-TB drugs like Isoniazid and Rifampin decrease the level of sulfonylureas (an antidiabetic drug) in the blood by drug-drug interaction, lead to hyperglycemia.
Pathology of Stress-Induced Hyperglycemia during Active TB
During the start of TB treatment, patients also screened for having hyperglycemia and they receive a new diabetes diagnosis (not earlier known to have diabetes). Although most of the recent studies have not determined what proportion of these new diabetes diagnoses have diabetic levels of blood glucose due to stress-hyperglycemia in response to active TB, and what proportion have previously undiagnosed but pre-existing diabetes [31]. Stress-induced hyperglycemia is a condition of dysglycemia resulting from various illnesses such as trauma, infection and surgery, or myocardial infarction. Stress-induced hyperglycemia results from multiple signal pathways including counter regulatory hormones such as glucagon, growth hormone, catecholamine, cortisol, and cytokines such as TNF-α and interleukin (IL-1) and IL-6. During chronic infections, whether with TB or other pathogens, these cytokines can drive stress-induced hyperglycemia by increasing hepatic glucose production (glyconeogenesis), peripheral insulin resistance or by modifying the signaling properties of insulin receptor substrates (IRS-1) [32, 33]. Increased hepatic output of glucose may therefore be more important than peripheral insulin resistance in the genesis of stress-induced hyperglycemia [34].
Sepsis is described as a harsh circumstances resulting from the presence of infectious microorganisms in the blood or other tissues and the body’s response to their presence, potentially leading to the malfunctioning of various organs. The insulin resistance in sepsis is directly proportional to the severity of stress response and marked by insulin resistance [35]. Insulin induces the phosphorylation of IRS-1 and subsequent activation of Phosphoinositide 3-kinases (PI- 3-K) is impaired resulting in defective glucose transporter-4 (GLUT-4) channel translocation toward the cell membrane from vacuoles, diminished glucose uptake, insulin resistance in skeletal muscle, and hepatic insulin resistance. Although the actual mechanism whereby sepsis induces these alterations are unidentified, but the induced level of TNF-α may play an important role in this mechanism. Aljada, et al. (2002) have confirmed that TNF -α causes reduction of tyrosine phosphorylation and expression of the insulin receptor in endothelial cells and diminishes the insulin- induced IRS-1 tyrosine phosphorylation in hepatocytes leads to make worse the activation of PI-3-K. TNF-α induced IRS- 1 serine phosphorylation which reduces ability to interact with the insulin receptor however, normally IRS-1 tyrosine phosphorylated protein by insulin receptor and to bind PI- 3-K [36, 37, 38, 39, 40, 41]. Gao, et al. [42] demonstrated that an inhibitor κB kinase (IKK) complex is activated by Toll-like receptor 4 (LTR4) as well as by TNF-α and IL-1 is associated with serine phosphorylation of IRS-1. The IKK as a serine kinase which manage the nuclear factor-kappa B (NF-κB) a ubiquitous nuclear transcription factor closely associated with the activation of the genes for almost all of the pro-inflammatory mediators. NF-κB is bounded to inhibitor κB (I κB) before activation, but IKK phosphorylates I κB on the serine residue leads to the degradation of I κB followed by the nuclear translocation of NF-κB. The phosphorylation of IRS-1 and I κB by IKK on the serine may partially elucidate the insulin resistance noted with activation of the pro-inflammatory cascade [42] (Figure 3).
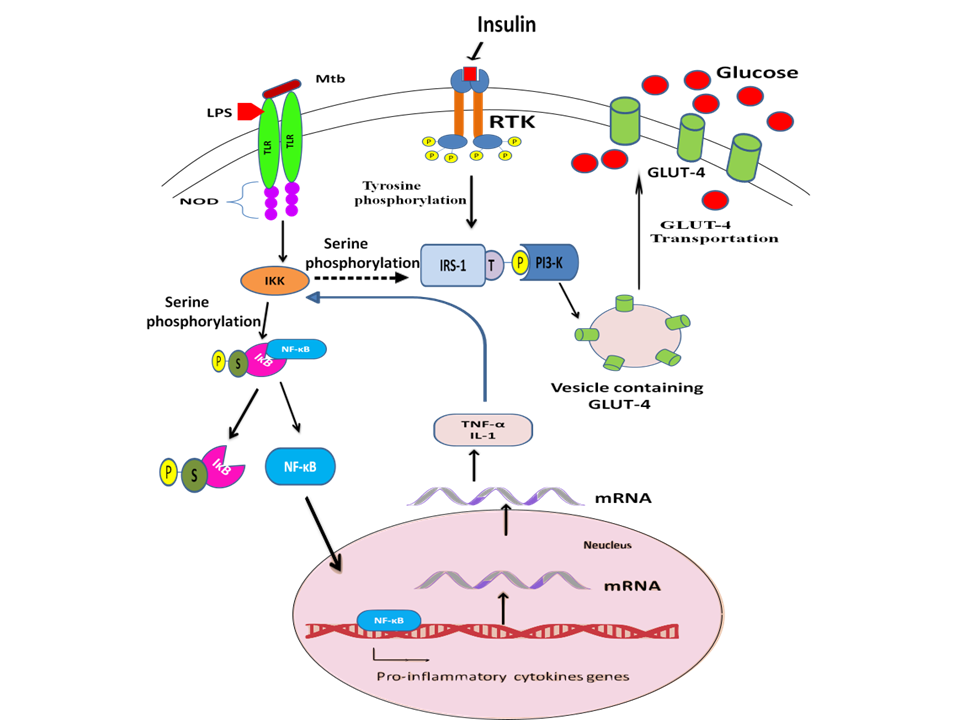
Figure 3: Impact of TB on DM: Lipopolysaccharide (LPS) interact with Toll Like receptors (TLR) and activates inhibitor κB kinase (IKK) complex, a serine kinase which phosphorylates inhibitor κB (I κB) on Serine residue tends to dissociate from nuclear factor-kappa B (NF-κB) and NF-κB translocate inside nucleus and activates pro-inflammatory cytokine genes. Insulin binds with Receptor tyrosine kinase (RTK) lead to dimerisation and auto-phosphorylation. RTK phosphorylates IRS-1 on Tyrosine residue and activates PI3K which trigger the translocation of GLUT-4 containing vesicles toward cell membrane and mediates uptake of glucose inside the cell through GLUT-4 (an insulin dependent glucose transporter channel). Pro- inflammatory cytokines TNF-α and IL-1 also activates IKK which might be phosphorylates IRS-1 on serine residue and make it inactive so PI3-K could not trigger the GLUT-4 translocation toward membrane and ultimately impair the glucose uptake inside cell. Increased level of glucose in the blood due to sepsis called stress induced hyperglycemia.
Drug-Drug Interaction
As an anti-TB drug Rifampicin is also a strong inducer of hepatic enzymes that accelerates the metabolism of several oral Anti-diabetic agents like sulphonylureas and biguanides’ and reduces their plasma levels in the blood and shown hyperglycemic effect in diabetic patients. However, in non-diabetic patients it enhances the intestinal absorption of glucose and may simulate the symptoms of diabetes. Isoniazid interacts with sulphonylureas and inhibits their action in the diabetic patients and in non-diabetic patients it impairs the release and action of insulin leading to hyperglycemia [43, 44].
Is there any Possibility to Diminish TB by Targeting DM?
TB treatment outcomes are adversely affected by DM, the reason behind it is not completely understood but drug- drug interactions adversely affects from medications. The suboptimal adherence to medication reduces bioavailability of the drugs and the immunosuppressive effects of DM itself have also been reported [29]. The efficiency of anti- TB drugs is hampered by Anti-diabetic drugs as a result of drug-drug interaction. DM increases the risk of TB by compromising our immune system which creates trouble to combat TB infections. In several studies stated that diabetes continues to be a risk factor for tuberculosis and there is a significant association between diabetes and MDR-TB. So by targeting DM as one of the associated factors of TB, it will optimize treatment response of TB [29, 45].
Significance
We have found reliable evidences which suggest a strong association of DM and TB which, in turn, increases the risk of TB among people those are suffering from DM. The prevalence of DM has been increasing in many countries since long time, thus it may threaten the success of TB control. A better understanding of this bidirectional relationship of the TB and DM is necessary for proper planning and collaboration to decrease the dual burden of diabetes and TB. Screening, prevention and treatment of both diseases together are more effective and may have a beneficial impact on TB control. Emerging information on human studies on the biological mechanisms by which hyperglycemia may affect the host immune response to TB needs to be understood [46]. Earlier management and screening of diabetes may reduce the risk of developing active TB.
Acknowledgement
The authors acknowledge financial support from the Department of Science and Technology-SERB, Council of Scientific and Industrial Research-Institute of Genomics and Integrative Biology under the research project GAP0145 (SERB-DST Grant no: EEQ/2016/000514).
Conflict of Interest
There is no conflict of interest.
References
-
Meena LS, Shaw S (2016) GT Pases: prerequisite molecular target in virulence and survival of Mycobacterium tuberculosis. International Journal of Molecular Biology: Open Access 1(1): 26-27.
-
Kandola P, Meena LS (2014) Extra pulmonary tuberculosis: Overview, manifestations, diagnostic and treatment techniques. Advanced Materials Reviews 1(1): 13-19.
-
Jasmer RM, Nahid P, Hopewell PC (2002) Clinical practice. Latent tuberculosis infection. New England Journal of Medicine 347(23): 1860-1866.
-
WHO (2019) Global Tuberculosis Report. Word Health Organization.
-
Ponce-De-Leon A, Garcia-Garcia Md Mde L, Garcia- Sancho MC, Gomez-Perez FJ, Valdespino-Gomez JL, et al. (2004) Tuberculosis and diabetes in southern Mexico. Diabetes Care 27(7): 1584-1590.
-
Chukanova VP, Sergeev AS, Pospelov LE, Sobkin AL (2000) Epidemiological and immunogenetic analysis of tuberculosis and diabetes mellitus association. Problemy Tuberkuleza (Moskva) 4: 11-14.
-
Olmos P, Donoso J, Rojas N, Landeros P, Schurmann R, et al. (1989) Tuberculosis and diabetes mellitus: a longitudinal-retrospective study in a teaching hospital. Revista medica de Chile 117(9): 979-983.
-
Suzanne E Geerlings, Andy IM Hoepelman (1999) Immune dysfunction in patients with diabetes mellitus (DM). FEMS Immunology & Medical Microbiology 26(3- 4): 259-265.
-
Alisjahbana B, Sahiratmadja E, Nelwan EJ, Purwa AM, Ahmad Y, et al. (2007) The effect of type 2 diabetes mellitus on the presentation and treatment response of pulmonary tuberculosis. Clinical Infectious Diseases 45(4): 428-435.
-
Stevenson CR, Critchley JA, Forouhi NG, Roglic G, G Williams B, et al. (2007) Diabetes and the risk of tuberculosis: a neglected threat to public health? Chronic Illness 3(3): 228-245.
-
Leung CC, Lam TH, Chan WM, Wing W Yew, Kin S Ho, et al. (2007) Lower risk of tuberculosis in obesity. Archives of internal medicine 167(12): 1297-1304.
-
Dooley KE, Chaisson RE (2009) Tuberculosis and diabetes mellitus: convergence of two epidemics. The Lancet infectious diseases 9(12): 737-746.
-
Geerlings SE, Hoepelman AI (1999) Immune dysfunction in patients with diabetes mellitus (DM). FEMS Immunology & Medical Microbiology 26(3-4): 259-265.
-
Fisher-Hoch SP, Whitney E, McCormick JB, Crespo G, Smith B, et al. (2008) Type 2 diabetes and multidrug- resistant tuberculosis. Scandinavian Journal of Infectious Diseases 40 (11-12): 888-893.
-
Janeway C, Travers P, Walport M, Shlomchik M (2004) Immunobiology: The immune system in health and disease, 5th (Edn.), Garland Science, New York.
-
Wang CH, Yu CT, Lin HC, Liu CY, Kuo HP (1999) Hypodense alveolar macrophages in patients with diabetes mellitus and active pulmonary tuberculosis. Tubercle Lung Disease 79(4): 235-242.
-
Rayfield EJ, Ault MJ, Keusch GT, Brothers MJ, Nechemias C, et al. (1982) Infection and diabetes: the case for glucose control. American Journal of Medicine 72(3): 439-450.
-
Madigan MT, Martinko JM, Parker J (1997) Brock biology of microorganisms, 8th (Edn.), Prentice Hall International, Inc., New York.
-
Kawakami K (2003) Tuberculosis in diabetes mellitus: aggravation and its immunological mechanism. Kekkaku 78: 717-722.
-
Geerlings SE, Hoepelman AI (1999) Immune dysfunction in patients with diabetes mellitus (DM). FEMS Immunology & Medical Microbiology 26(3-4): 259-265.
-
Girardi E, Schepisi MS, Goletti D, Bates M, Mwaba P, et al. (2017) The global dynamics of diabetes and tuberculosis: the impact of migration and policy implications. International Journal of Infectious Diseases 56: 45-53.
-
Koziel H, Koziel MJ (1995) Pulmonary complications of diabetes mellitus. Infectious Disease Clinics of North America 9(1): 65-96.
-
Yuan FH, Guang LX, Zhao SJ (2005) Clinical comparisons of 1,498 chronic renal failure patients with and without tuberculosis. Renal failure 27(2): 149-153.
-
Vijayamalini M, Manoharan S (2004) Lipid peroxidation, vitamins C, E and reduced glutathione levels in patients with pulmonary tuberculosis. Cell biochemistry and function 22(1): 19-22.
-
Prasad AS (2008) Zinc in human health: effect of zinc on immune cells. Molecular medicine 14(5-6): 353-357.
-
Chocano-Bedoya P, Ronnenberg AG (2009) Vitamin D and tuberculosis. Nutrition reviews 67(5): 289-293.
-
Walker AR, Segal I (1999) Iron overload in Sub-Saharan Africa: to what extent is it a public health problem? British Journal of Nutrition 81(6): 427-434.
-
Sahiratmadja E, Wieringa FT, van Crevel R, de Visser AW, Adnan I, et al. (2007) Iron deficiency and NRAMP1 polymorphisms (INT4, D543N and 3′ UTR) do not contribute to severity of anaemia in tuberculosis in the Indonesian population. British journal of nutrition 98(4): 684-690.
-
Harries AD, Kumar AM, Satyanarayana S, Lin Y, Zachariah R, et al. (2016) Addressing diabetes mellitus as part of the strategy for ending TB. Transactions of the Royal Society of Tropical Medicine and Hygiene 110(3): 173- 179.
-
Lin Y, Harries AD, Kumar AMV, Critchley JA, van Crevel R, et al. (2019) Management of diabetes mellitus- tuberculosis: a guide to the essential practice. International Union against Tuberculosis and Lung Disease, Paris, France.
-
Magee MJ, Salindri AD, Kyaw NTT, Auld SC, Haw JS, et al. (2018) Stress hyperglycemia in patients with tuberculosis disease: epidemiology and clinical implications. Current diabetes reports, 18(9): 71.
-
McCowen KC, Malhotra A, Bistrian BR (2001) Stress- induced hyperglycemia. Critical Care Clinics 17(1): 107- 124.
-
Hotamisligil GS, Spiegelman BM (1994) Tumor necrosis factor alpha: A key component of the obesity-diabetes link. Diabetes 43(11): 1271-1278.
-
Jeevanandam M, Young DH, Schiller WR (1990) Glucose turnover, oxidation, and indices of recycling in severely traumatized patients. Journal of Trauma 30(5): 582-589.
-
Mizock BA (2001) Alterations in fuel metabolism in critical illness hyperglycemia. Best Practice & Research Clinical Endocrinology & Metabolism 15(4): 533-551.
-
Pessin JE, Saltiel AR (2000) Signaling pathways in insulin action: molecular targets of insulin resistance. Journal of Clinical Investigation 106(2): 165-169.
-
Aljada A, Ghanim H, Assian E, Dandona P (2002) Tumor necrosis factor-alpha inhibits insulin-induced increase in endothelial nitric oxide synthase and reduces insulin receptor content and phosphorylation in human aortic endothelial cells. Metabolism 51(4): 487-491.
-
Hotamisligil GS, Peraldi P, Budavari A, Ellis R, White MF, et al. (1996) IRS-1-mediated inhibition of insulin receptor tyrosine kinase activity in TNF-alpha- and obesity-induced insulin resistance. Science 271(5249): 665-668.
-
Kanety H, Feinstein R, Papa MZ, Hemi R, Karasik A (1995) Tumor necrosis factor alpha-induced phosphorylation of insulin receptor substrate-1 (IRS-1). Possible mechanism for suppression of insulin-stimulated tyrosine phosphorylation of IRS-1. Journal of Biological Chemistry 270(40): 23780-23784.
-
Paz K, Hemi R, LeRoith D, Karasik A, Elhanany E, et al. (1997) A molecular basis for insulin resistance. Elevated serine/threonine phosphorylation of IRS-1 and IRS-2 inhibits their binding to the juxta membrane region of the insulin receptor and impairs their ability to undergo insulin-induced tyrosine phosphorylation. Journal of Biological Chemistry 272(47): 29911-29918.
-
Hotamisligil GS, Budavari A, Murray D, Spiegelman BM (1994) Reduced tyrosine kinase activity of the insulin receptor in obesity-diabetes. Central role of tumor necrosis factor-alpha. Journal of Clinical Investigation 94(4): 1543-1549.
-
Barnes PJ, Karin M (1997) Nuclear factor-kB-A pivotal transcription factor in chronic inflammatory diseases. New England Journal of Medicine 336(15): 1066-1071.
-
Atkin SL, Masson EA, Bodmer CW, Walker BA, White MC (1993) Increased insulin requirement in a patient with Type 1 diabetes on Rifampicin. Diabetic Medicine 10(4): 392.
-
Lebovitz HE (1990) Oral hypoglycemic agents. In: Rifkin H, Porte Jr D, (Eds.), Ellenberg and Rifkins’s diabetes mellitus, theory and practice, 4th (Edn.), Elsevier, New York, pp: 554-574.
-
Pandey A, Shivangi P, Meena LS (2018) Correlated Diabetes Mellitus and Tuberculosis: The Challenge Continues. Molecular and Cellular Biochemistry 2(1): 7.
-
Meena LS, Rajni (2010) Survival mechanisms of pathogenic Mycobacterium tuberculosis H37Rv. FEBS J 277(11): 2416-2427.
- Investigation of Polymorphisms in PPAR-Ɣ and TRHR Genes and their Impact on Turkish Diabetic and Obese Individuals
- The Impact of Aircraft Noise Exposure on the Efficacy of Empagliflozin Therapy in an Animal Model of Obesity
- Rooibos Mitigates Metabolic and Inflammatory Dysfunctions in Mice Fed a High-Carbohydrate Diet
- Synergistic Effect of Combined Leaf Extract of Vernonia amygdalina, Ocimum gratissimum, and Zingiber officinale Tuber on Phytochemical Profile, Antioxidant Activity, Serum Insulin, and Biochemical Parameters in Streptozotocin-Induced Diabetic Rats
- Investigation of Cardiovascular Responses to Aerobic Exercise in Obese University Students
- A Look at the Phase Angle Obtained by Electrical Bioimpedance