Hydrogen Breath Test to Diagnose Lactose Malabsorption: Milk, Lactose and Osmotic Effect
Purpose: There is no gold standard to diagnose lactose malabsorption. The hydrogen breath test is the most widely used, but many methodological points need to be standardized. Our aims were to verify (a) whether the use of milk rather than lactose solution improves accuracy, and (b) whether different concentrations of the lactose solution modify the results. Materials and Methods: 33 healthy volunteers underwent the H2 breath test after 400 ml of semi-skimmed milk and after an oral solution containing 20 g of lactose in 400 ml of water; a second group of 38 healthy volunteers underwent the H2 breath test after 400 ml of semi-skimmed milk and after an oral solution containing 20 g of lactose in 200 ml of water. Basal gastrointestinal transit was evaluated with radio-opaque markers. Results: In 31 out of 33 subjects H2 breath test results were concordant after milk and 20g of lactose in 400 ml of water. Two subjects were positive after lactose, but negative after milk. The time at which the test became positive was earlier after lactose than after milk. The administration of a more concentrated lactose solution increased discrepant results, as in 5 subjects out of 38 the H2 breath test was negative after milk and positive after lactose solution. Basal gastrointestinal transit time did not show any significant difference between positive and negative subjects. Conclusions: To diagnose lactose malabsorption, milk is a more physiologic substrate for the H2 breath test. Lactose solutions induce an osmotic effect which can cause false positive results.
Introduction
Lactose malabsorption is a widespread condition throughout the world caused by a genetically determined decline of lactase activity, inherited through an autosomal recessive gene [1]. This condition is characterized by a spectrum of clinical expression, as it may be completely asymptomatic or it may cause intolerance of varying degrees: abdominal pain, bloating, flatulence and diarrhoea, evoked by milk and dairy product consumption [2] are the most frequent symptoms. To avoid symptom onset, lactose intolerant patients spontaneously reduce milk and dairy product intake, exposing themselves to a high risk of nutritional defects, such as a secondary loss of bone mass [3]. It has also been shown that many lactase deficient patients fail to recognize their own lactose malabsorption [2, 4, 5, 6]: accordingly, an objective test is needed to ascertain, first of all, lactose absorption capacity. As lactose intolerance is characterized by a clinical overlap with functional bowel disorders, it is possible that a large number of patients may unnecessarily avoid milk and dairy products in their diet. Up to now, there is no test which can be considered as a gold standard to diagnose lactose malabsorption. The hydrogen breath test is one of the most widely used as it is simple and cheap, but, more than 40 years since its introduction in clinical practice [7], many methodological issues still need to be standardized. First of all, the need for a standardized substrate is evident. Results based on an oral dose of lactose of 50g [8, 9] 25g [10], 20g [11, 12] or even 12g [6, 13, 14] are available. There are also marked differences in terms of concentration of the lactose solution, as a 50g dose has been diluted in 500 [15], 300 [13], 250 [16] or 200 cc of water [17]. We have previously shown that increasing concentrations of a low absorbable sugar, sorbitol, determine an increased prevalence of malabsorption [18]. Accordingly, an osmotic effect of the solution may be responsible for a false positivity of the H2 breath test. Our aim was, therefore, to verify whether an osmotic effect may influence H2 breath test result, by comparing test positivity after two lactose solutions and milk administration.
Patients and Methods
Subjects
Eighty-one healthy subjects (55 females mean age 30±2 yrs, age range 20-38 yrs) were enrolled. All subjects were members of the medical or paramedical staff of our hospital, or were students attending our School of Medicine. They were all recruited on a voluntary basis, but no form of recompense was foreseen. They were fully compliant and gave their informed consent to the study. None of them suffered from intestinal, liver, renal, chest, cardiac, metabolic or neurologic diseases and none were taking antibiotics, prokinetics, laxatives or any other drug known to influence colonic flora in the month preceding the study. In particular, the administration of Gastrointestinal Symptom Rating Scale [19] excluded the presence of gastrointestinal symptoms. All the subjects underwent a preliminary H2 breath test after oral lactulose to exclude H2 non-producers. Moreover, to exclude possible interference from intra luminal H2 consumption, methane-producer subjects were also excluded. Five methane-producers and five H2 non-producers were excluded. Seventy-one subjects (50 females, mean age 31±2 yrs, age range 21-37 yrs) thus took part in the study and were subdivided into two groups: the first group (33 subjects, 21 females, mean age 30±4 yrs, age range 20-37 yrs) underwent the H2 breath test after 400 ml of semi-skimmed milk (containing 20g of lactose) and after an oral solution containing 20 g of lactose in 400 ml of water on two separate days at least one week apart, in a random order. The second group (38 subjects, 29 females, mean age 30±5 yrs, age range 20-36 yrs) underwent the H2 breath test after 400 ml of semi- skimmed milk (containing 20g of lactose) and after an oral solution containing 20 g of lactose in 200 ml of water on two separate days at least one week apart, in a random order. The H2 breath test was previously demonstrated to be able to objectively reveal the presence of lactose malabsorption, regardless of the patient’s assessment [5].
Hydrogen Breath Testing
In order to avoid prolonged intestinal gas production, due to the presence of non-absorbable or slowly fermentable material in the colonic lumen, the subject consumed a meal consisting of only rice, meat and olive oil the evening before the test day [20]. This meal was then followed by a 12-hour fasting period. Breath testing started between 08.30 a.m. and 09.30 a.m., after thorough mouth washing with 40 ml of 1% chlorhexidine solution [21]. Smoking [22] and physical exercise [23] were not allowed for one hour prior to and throughout the test. Sampling of alveolar air was performed by means of a commercial device (Gasampler Quintron, Milwaukee, WI, USA) that allows the first 500 ml of dead space air to be separated and discarded while the remaining 700 ml of end-alveolar air are collected in a gas-tight bag. Subjects were instructed to avoid deep inspiration and not to hyperventilate before exhalation. A gas chromatograph dedicated to the detection of H2 and CH4 in air samples was used for breath sample analysis (Model DP12, Quintron Instrument, Milwaukee, WI, USA). The accuracy of the detector was ±2 ppm with a linear response range between 2 and 150 ppm of H2 and between 2 and 50 ppm of CH4. To exclude the possibility of a false negative test due to unknown H2 non-producer status [24], all the subjects underwent breath H2 measurement after lactulose administration on a separate day. Ten grams of lactulose in a 400ml water solution were administered and air samples were collected every 15 minutes for an 8-hour period. A patient was considered an H2 non-producer when none of the breath samples showed a breath H2 excretion value higher than 20 ppm. The presence of an average breath CH4 concentration >5 ppm above that of room air during breath testing was considered indicative of CH4 production [25]. The test was considered as indicative of the presence of lactose malabsorption when breath H2 excretion proved to be higher than 20 ppm over the baseline within four hours after carbohydrate administration, sampling every 30 minutes. If at the end of the fourth hour the test was negative, breath H2 excretion was measured for three hours more, sampling every 30 minutes, and the test was considered positive if the sum of the H2 concentration in breath samples obtained at the 5th, 6th and 7th hour was ≥15 ppm [26, 27]. The peak of breath H2 excretion and the time of occurrence of the peak of breath H2 excretion were also noted. To exclude a possible interference of gastrointestinal transit time, an evaluation of gastrointestinal transit time in Toto with radio-opaque markers was performed in all the subjects, according to Metcalf et al [28], some days before the H2 breath test.
Data Analysis
Breath test results were compared to evaluate the concordance among the solutions. The value of the peak of H2 in breath and the time of occurrence of the peak after milk and lactose solutions were then compared. The variables were tested for distribution with Kolmogoronov-Smirnov normality test. Some variables showed nonparametric distribution and, accordingly, a nonparametric test was performed. The specific test performed for the comparison is indicated in brackets in the text. Variable are expressed as mean±SD or median and range. A p value<0.05 was considered significant.
Results
The first comparison was performed between 400 ml of semi-skimmed milk and a 400 ml water solution containing 20 g of lactose. In 31 out of 33 tested subjects the same results were obtained after both solutions: in fact, 13 subjects were negative and 18 subjects were positive. On the contrary, one female and one male subject proved to be negative after milk and positive after lactose solution. The evaluation, some days before breath tests, of gastrointestinal transit in toto with radio-opaque markers showed no significant difference between patients with positive (37±5 hrs) and negative (36±4 hrs) H2 breath tests (p=NS; unpaired t test). The subjects showing discordant results had a gastrointestinal transit of 35 and 34 hrs, respectively. Figure 1A shows the time at which the test became positive after milk and lactose (20g in 400 cc of water) in the group of 18 subjects positive at both test. It is evident that the time at which the test became positive was significantly earlier (p<0.0001; Wilcoxon matched-pairs signed-ranks test) after lactose solution (median 135 min, range 30-240) than after milk (median 240 min, 90-420). Moreover, the peak of breath H2 excretion was significantly higher (p<0.05; paired t test) after lactose solution (47±18 ppm, mean±DS) than after milk (39±17 ppm, mean±DS) (Figure 1B). After lactose solution, the time at which the peak of breath H2 excretion occurred was significantly earlier than after milk (187±62 min vs 263±96 min, respectively; p<0.004). Figure 2 shows breath H2 excretion after milk and lactose solution in the subjects with discordant results.
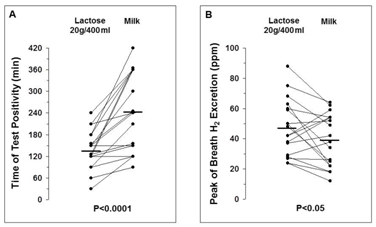
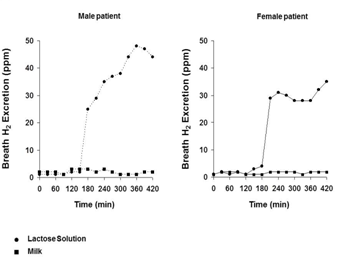
Figure 2: Breath hydrogen excretion after milk and a solution containing 20g of lactose in 400 ml of water in two subjects with discrepant results. The second comparison was performed between 400 ml of semi-skimmed milk and a 200 ml water solution containing 20 g of lactose. Thirty-three out of 38 subjects showed the same result after both test solutions: in particular, 20 subjects were positive and thirteen were negative. In five subjects, breath H2 excretion did not show any modification after milk, but the administration of the solution containing 20 g of lactose in 200 ml of water induced a significant increase of breath H2 excretion, making the test positive. The evaluation of gastrointestinal transit in to with radio-opaque markers some days before breath tests showed no significant difference between patients with positive (34±6 hrs) and negative (33±5 hrs) H2 breath tests (p=NS; unpaired t test). The subjects showing discordant results had a mean gastrointestinal transit of 34±7 hrs. Figure 3A shows the time at which the test became positive after milk and lactose (20g in 200 cc of water) in the group of 20 concordantly positive subjects. Also in this case, the time at which the test became positive was significantly earlier (p<0.0001; paired t test) after lactose solution (median 120 min, range 30-210) than after milk (median 240 min, 90-420) and the peak of breath H2 excretion was significantly higher (p<0.02; paired t test) after lactose solution (49±18 ppm, mean±DS) than after milk (40±15 ppm, mean±DS) (Figure 3B).
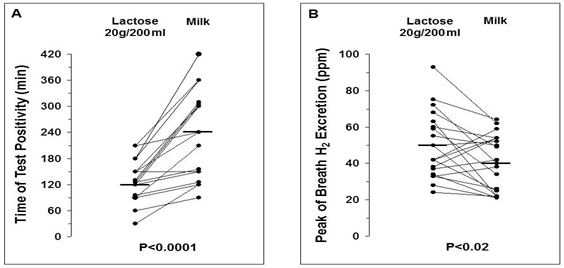
After lactose solution, the time at which the peak of breath H2 excretion occurred was significantly earlier than after milk (178±65 min vs 271±98 min, respectively; p<0.0002). In Table 1, time at which positivity of the test occurred and peak of breath H2 excretion after milk and lactose solution (20g in 200 ml of water) in the five subjects with discordant results are shown. The positivity of the test occurred at 114±49 min and the mean of the peak of breath H2 excretion was 59±18 ppm.
| Positivity time | Peak | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pts | Milk | Lactose 20g/200 ml | Milk | Lactose 20g/200 ml | ||||||
| MC | - | 60 | 3 | 50 | ||||||
| AC | - | 90 | 2 | 55 | ||||||
| RM | - | 150 | 2 | 49 | ||||||
| AM | - | 90 | 3 | 91 | ||||||
| MG | - | 180 | 2 | 49 |
Discussion
The hydrogen breath test is widely used to diagnose lactose malabsorption, but very often the adopted protocol is not correct. Twelve years ago, we conducted a multicentre study to evaluate hydrogen breath test methodology in a group of 15 Italian gastroenterology clinics and many major differences were evident [29]. These differences still characterize daily practice, as demonstrated by the results of a recent consensus conference on methodology, role and indications of the hydrogen breath test [30]. Lactose intolerance may represent a source of confusion in the clinical approach to patients with abdominal symptoms. It has been shown that lactose mal absorbers very frequently fail to properly attribute their symptoms to lactose intake as they are able to ingest substantial amounts of milk without symptom onset [4, 5, 6]. Nevertheless, they spontaneously avoid milk and dairy products and expose themselves to a high risk of nutritional defects [3]. An objective test is therefore needed, which is accurate enough to indicate when lactose malabsorption is really present or absent: this test, particularly in a population characterized by a high prevalence of lactose malabsorption, must make it possible to exclude with certainty that lactose intolerance is responsible for the patient’s symptoms. In other words, in a population characterized by a high prevalence of lactose malabsorption, the negative predictive value of the test is more important than its positive predictive value. The test should be as “physiological” as possible, i.e. it must mirror the patient’s daily life as closely as possible. This applies both to the dose of carbohydrate oral load and to the type of substrate: since patients drink milk and not a lactose solution during their symptom-inducing meals, in our opinion, the test should be performed by giving milk to the patient. Dairy products, especially milk, contain variable amounts of lipids, which induce delayed gastric emptying [31, 32] and a gradual entry of lactose into the intestine. This mechanism may reduce intolerance symptoms [33] and, therefore, it should be considered in the clinical approach to patient symptoms. We therefore compared breath test results after milk or lactose solution in a group of healthy volunteers. When a subject proved to be negative after lactose solutions, milk administration also resulted in a negative test. On the contrary, seven subjects who were negative after milk proved to be positive after the lactose solutions: in particular, two subjects were positive after the 5% solution (20g in 400ml) and 5 were positive after the 10% solution (20g in 200 ml). Both the lactose solutions induced earlier positivity of the test (Figures 1 & 3) suggesting the role of an osmotic effect. A hyperosmolar solution may be responsible for an accelerated intestinal transit, causing malabsorption of the substrate due to a too short contact with intestinal mucosa. This point is also proved by the significantly earlier occurrence of the peak after both the lactose solutions than after milk. Moreover, we previously showed that the administration of a dietary sweetener, sorbitol, a low absorbable sugar, is frequently accompanied by malabsorption of this compound [18]. But, more interestingly, if the substrate is administered in solution at increasing concentrations, the prevalence of malabsorption runs parallel to the concentration of the solution. Our results show that both 5% and 10% lactose solutions may cause false negative breath tests. The time of positivity after 5% solution is similar to the time of positivity after 10% solution: this result suggests that if lactose solution is preferred as a breath test substrate, the concentration of the solution should be less than 5%. Moreover, the earlier positivity of the test after lactose solutions could suggests a shortening of the test. However, we think this is not the case for at least two reasons: first of all, because an important number of subjects, when retested after milk, prove to be negative; secondly, the amount of milk administered during this test is higher than the amount currently consumed in an Italian breakfast. Consequently, we think that an osmotic effect after lactose solution reduces the accuracy of the test and the hypothesis of a false negativity after milk is improbable due to its high oral load. We performed this study in healthy volunteers in order to exclude possible interferences due to alterations of gastrointestinal transit time. We are sure of this, as the measurement of this parameter did not show any difference between positive and negative subjects. However, we think that when the H2 breath test is performed in day-to-day clinical practice, we will with certainty encounter patients with alterations of gastrointestinal transit, especially the subgroup with diarrhea, often characterized by an increased intestinal motor activity. It is conceivable that this subgroup will hamper the osmotic effect of a too concentrated solution, increasing the risk of false positivity and making the test poorly accurate. These considerations, besides alterations of visceral sensitivity [34], may at least in part explain why the threshold dose of lactose-causing symptoms in a group of individuals with low lactase levels ranges from 3 to 90g of lactose [35] and, in a review of multiple studies, the prevalence of intolerance to a 12-g dose of lactose ranges from 0 to 75% of patients [36]. For this reason and also for the recently shown very low accuracy of symptom occurrence during the test [37], we avoid to present symptom occurrence in our results. In conclusion, our data suggest that a more physiologic substrate for the H2 breath test is represented by milk. The use of lactose solution, in fact, may be associated with reduced accuracy: both the 10% and the 5% lactose solutions were influenced by an osmotic effect. It is likely that by slowing gastric emptying, milk fat causes a more gradual transit of lactose through the intestine, optimizing the activity of intestinal lactase.
Acknowledgments
The Authors thank Ms. Susan West for linguistic revision
References
-
Flatz G (1987) Genetics of lactose digestion in humans. Adv Human Genet 16: 1-77.
-
Bayless TM, Rothfeld B, Massa C, Wise L, Paige D, et al. (1975) Lactose and milk intolerance: clinical implications. NEJM 292(22): 1156-1159.
-
Di Stefano M, Veneto G, Malservisi S, Cecchetti L, Minguzzi L, et al. (2002) Lactose malabsorption and intolerance and peak bone mass. Gastroenterology 122(7): 1793-1799.
-
Welsh JD (1970) Isolated lactase deficiency in humans: report on 100 patients. Medicine; 49(4 ): 257-277.
-
Suarez FL, Savaiano DA, Levitt MD (1995) A comparison of symptoms after the consumption of milk or lactose-hydrolyzed milk by people with self- reported severe lactose intolerance. NEJM 333(1): 1- 4.
-
Suarez FL, Savaiano DA, Arbisi P, Levitt MD (1997) Tolerance to the daily ingestion of two cups of milk by individuals claiming lactose intolerance. Am J Clin Nutr 65: 1502-1506.
-
Levitt MD, French P, Donaldson RM. (1968) Use of hydrogen and methane excretion in the study of the intestinal flora. J Lab Clin Med 72: 988-989.
-
Metz G, Jenkins DJA, Peters JJ, Alwin Newman, Laurence M Blendis (1975) Breath hydrogen as a diagnostic method for hypolactasia. Lancet 1: 1155- 1157.
-
Newcomer AD, McGill DB, Thomas PJ, Hafmann AD (1975) Prospective comparison of indirect methods for detecting lactose deficiency. NEJM 293: 1232- 1236.
-
Mishkin B, Yolovsky M, Mishkin S (1997) Increased prevalence of lactase malabsorption in Crohn’s disease patients at low risk for lactose malabsorption based on ethnic origin. Am J Gastroenterol 92: 1148- 1153.
-
Corazza GR, Ginaldi L, Furia N, Marani-Toro G, Di Giammartino D, et al. (1997) The impact of HIV infection on lactose absorbitive capacity. J Infect 35: 31-35.
-
Saltzman JR, Russell RM, Golner B, Barakat S, Dallal GE, et al. (1999) A randomized trial of Lactobacillus acidophilus BG2F04 to treat lactose intolerance. Am J Nutr; 69: 140-6.
-
Ladas S, Papanikos J, Arapakis G (1982) Lactose malabsorption in Greek adults: correlation of small bowel transit time with the severity of lactose intolerance. Gut 23(11): 968-973.
-
Argnani F, Di Camillo M, Marinaro V (2008) Hydrogen breath test for the diagnosis of lactose intolerance: is the rosutine sugar load the best one? World J Gastroenterol 14(40): 6204-6207.
-
Kerlin P, Wong L (1987) Lactose tolerance despite hypolactasia in adult coeliac disease. J Gastroenterol Hepatol 2(3): 233-237.
-
Briet F, Pochart P, Marteau P, Flourie B, Arrigoni E, et al. (1997) Impaired clinical tolerance to chronic lactase ingestion in subjects with lactase intolerance: a placebo effect? Gut 41(5): 632-635.
-
Tolliver BA, Jackson MS, Jackson KL, Barnett ED , Chastang JF, et al. (1996) Does lactose maldigestion really play a role in the irritable bowel? J Clin Gastroenterol 23(1): 15-17.
-
Corazza GR, Strocchi A, Rossi R, Sirola D, Gasbarrini G (1988) Sorbitol malabsorption in normal volunteers and in patients with coeliac disease. Gut 29(1): 44-48.
-
Svedlund J, Sjodin I, Dotevall G (1988) GSRS – a clinical rating scale for gastrointestinal symptoms in patients with irritable bowel syndrome and peptic ulcer disease. Dig Dis Sci 33(2): 129-134.
-
Corazza GR, Strocchi A, Gasbarrini G (1987) Fasting breath hydrogen in celiac disease. Gastroenterology 93(1): 53-58.
-
Thompson DG, O'Brien JD, Hardie JM (1986) lnfluence of the oropharyngeal microflora on the measurements of exhaled breath hydrogen. Gastroenterology 91(4): 853-860.
-
Rosenthal A, Solomons NW (1983) Time-course of cigarette smoke contamination of clinical hydrogen breath-analysis tests. Clin Chem 29(11): 1980-1981.
-
Payne DL, Welsh JD, Claypool PL (1983) Breath hydrogen [H2] response to carbohydrate malabsorption after exercise. J Lab Clin Med 102(1): 147-150.
-
Corazza GR, Strocchi A, Sorge M, Bentai G, Gasbarrini G (1993) Prevalence and consistency of low breath H2 excretion following lactulose ingestion. Possible implications for the clinical use of the H2 breath test. Dig Dis Sci 38(11): 2010-2016.
-
Corazza GR, Benati G, Strocchi A, Malservisi S, Gasbarrini G (1994) The possible role of breath methane measurement in detecting carbohydrate malabsorption. J Lab Clin Med 124(5): 695-700.
-
Strocchi A, Corazza GR, Ellis C, Giovanni Gasbarrini, Levittcorrespondence MD (1993) Detection of low doses of carbohydrate: accuracy of various breath H2 criteria. Gastroenterology 105(5): 1404-1410.
-
Di Stefano M, Missanelli A, Miceli E, Strocchi A, Corazza GR (2004) Hydrogen breath test in the diagnosis of lactose malabsorption: accuracy of new versus conventional criteria. J Lab Clin Med 144(6): 313-318.
-
Metcalf AM, Phillips SF, Zinsmeister AR, MacCarty RL, Beart RW, et al. (1987) Simplified assessment of segmental colonic transit. Gastroenterology 92(1): 40-47
-
Strocchi A, Corazza GR, Anania C, Benati G, Malservisi S, et al. (1997) Quality control study of H2 breath testing for the diagnosis of carbohydrate malabsorption in Italy. The "Tenue Club" Group. It J Gastroenterol Hepatol 29(2): 122-127.
-
Gasbarrini A, Corazza GR, Gasbarrini G, Montalto M, Di Stefano M, et al. (2009) Methodology and indications of H2-breath testing in gastrointestinal diseases: the Rome Consensus Conference. Aliment Pharmacol Ther 29 [1]: 1-49.
-
Hunt JN, Stubbs DF (1975) The volume and energy content of meals as determinants of gastric emptying. J Physiol 245(1): 209-225.
-
Kroop HS, Long WB, Alavi A, John R. Hansell (1979) Effects of water and fat on gastric emptying of solid meals. Gastroenterology 77(5): 997-1000.
-
Ravich WJ, Bayless TM (1983) Carbohydrate absorption and malabsorption. Clin Gastroenterol 12(2): 335-356.
-
Di Stefano M, Miceli E, Mazzocchi A, Tana P, Moroni F, et al. (2007) Visceral hypersensitivity and intolerance symptoms in lactose malabsorption. Neurogastroenterol Motil 19(11): 887-895.
-
Bedine MS, Bayless TM (1973) Intolerance of small amounts of lactose by individuals with low lactase levels. Gastroenterology 65(5): 735-743.
-
Newcomer AD (1981) Immediate symptomatic and long term nutritional consequences of hypolactasia. In: Lactose digestion: clinical and nutritional implications. Paige DM, Bayless TM (eds.) Baltimore: Johns Hopkins Univ Press 280.
-
Vernia P, Di Camillo M, Foglietta T, Avallone VE, De Carolis Av(2010) Diagnosis of lactose intolerance and the “nocebo” effect: the role of negative expectations. Dig Liver Dis 42(9): 616-619.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient