An Unusual Cause of Anasarca – A Paediatric Case Report and Review
Introduction
Menetrier’s disease is a rare cause of hypertrophic gastropathy in paediatric age group. It is characterised by giant hypertrophy of gastric rugal folds affecting proximal stomach [1]. Patients often present with nonspecific symptoms like anorexia, vomiting or loss of weight. As the diagnosis is very rare and symptoms are not specific diagnosis may be delayed. Here we present a case of MD that presented with anasarca and reduced urine output mimicking Nephrotic Syndrome. Keywords: Menetrier’s Disease; Oesophagogastroduodenoscopy; Hypertrophic gastropathy; Ileocolonoscopy; Proteinuria Abbreviations: MD: Menetrier’s Disease; CMV: Cymegalovirus; TGF : Transformin Growth Factor; EGFR: Epidermal Growth Factor Receptor ; GI : Gastrointestinal
Case Report
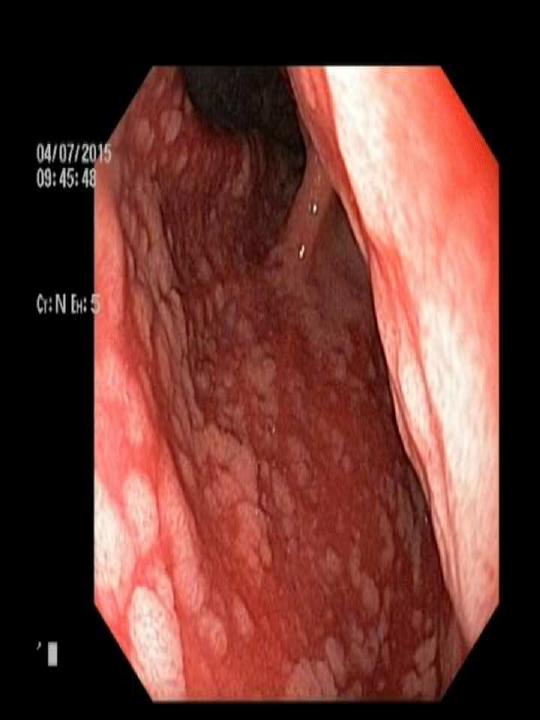
A 4 yr old girl was admitted from emergency with 7 days history of generalised swelling of whole body that started from periorbital area and progressed downwards gradually. History revealed that the illness started with several episodes of vomiting for 5 days with reduced urine output. She was managed locally with intravenous rehydration and symptomatic treatment like acute gastroenteritis without any improvement. She was a well grown young female from non consanguinous birth with normal developmental history. On examination she had facial puffiness, pedal oedema with some dehydration and tachycardia. Abdominal examination revealed ascites. Initial investigation showed hyponatraemia (serum Sodium of 122mmole/L), hypoalbuminaemia ( albumin 1.6gm/dL and globulin 1.8gm/dL) , normal liver enzymes and normal complete blood count. Her abdominal ultrasound was essentially normal except mild ascites. Her hyponatremia was corrected slowly over next 48 hrs. In view of proteinuria a provisional diagnosis of Nephrotic Syndrome was thought of. But serial urine dipstick showed no proteinuria in next few days but her urine output went on decreasing, oedema increased further, was not taking oral feeds and became lethargic. So, she was started on albumin infusion and furosemide injection following which she improved clinically. As urine protein excretion was never in nephrotic range and there was alteration of albumin: globulin ratio some other pathology for protein loss was sought. To exclude enteric protein loss Esophagogastroduodenoscopy and ileocolonoscopy were performed. Upper GI endoscopy revealed polypoid lesions with giant gastric folds with overlying ulcers, oozing and thick mucus, in the fundus and proximal gastric body sparing antrum (Figures 1 & 2).

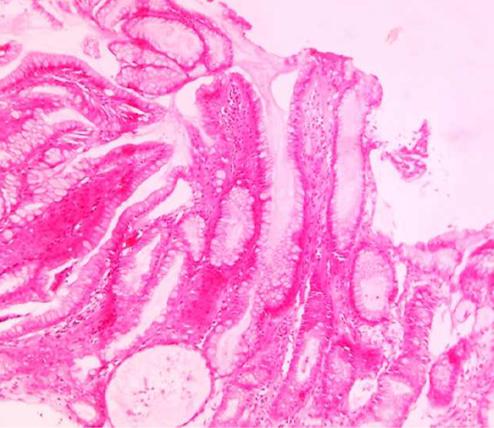
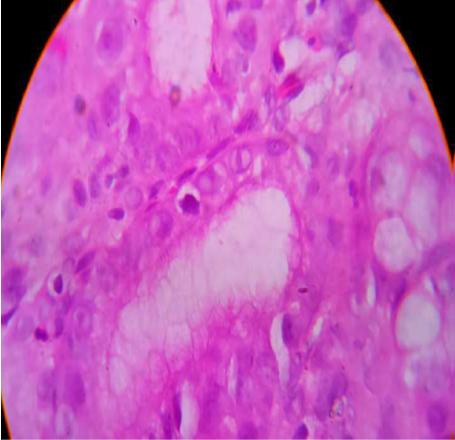
Ileocolonoscopy was normal macroscopically. Biopsy from gastric folds showed markedly hypertrophied foveolae with active gastritis and intranuclear inclusion bodies consistent with cytomegalovirus infection (Figures 3 & 4). This microscopy hinted towards a diagnosis of Menetrier’s disease likely secondary to cytomegalovirus infection.
She improved clinically with proton pump inhibitor, oral anti-emetics and protein rich diet. Plasma albumin level increased steadily over time with highest level of 3.9gram/dL during discharge. Presently she is asymptomatic. Follow up endoscopy after 6 months showed normal appearance of gastric mucosa.
Discussion
Menetrier’s Disease (MD) was first described by Menetrier in 1888 [1]. It is a gastropathy, characterised by giant rugal hypertrophy of gastric mucosa associated with protein loss across the abnormal mucosa. A non protein losing variety of MD has also been reported in children as well as in adults [2]. Till 2008 around 50-60 cases of paediatric MD have been reported all over the world [3]. Aetiology in most of the cases of MD remains unknown. Suggested etiologies include chemical irritants, toxins, dietary factors and immune mediation. But the best known association of paediatric MD is with CMV infection, while adult MD is often associated with H pylori [4]. In a publication of MD in 56 children, 26 were found to have CMV infection and 16 were found to have CMV inclusion bodies in gastric biopsy like the index case [4]. A familial form of protein-losing enteropathy with autosomal dominant inheritance has also been reported [5]. TGF-α, a ligand to EGFR has been implied to play a role in the pathogenesis of Menetrier’s disease due to its local growth-stimulating effect via EGFR binding, leading to foveolar hyperplasia and hypertrophic gastropathy in mice. This specific mediator is found to be over-expressed in adults and children with Menetrier’s disease. Suggested pathogenic mechanism of mucosal damage caused by CMV infection may involve the production of abnormal local TGF-α, which stimulates cell proliferation of gastric mucosa, inhibits gastric secretion, and enhances mucus secretion [6]. Nausea, vomiting and oedema are usual early symptoms, present in the index case as well, which may point towards diagnosis. Laboratory evidences are hypoproteinemia and hypoalbuminemia. MD is associated with low gastric acid production [1]. Children may present with ascites and pleural effusion. Upper GI endoscopy with biopsy is always the definitive investigation of choice that universally reveals large rugal folds [7]. A few other differential diagnoses of giant rugal folds are eosinophilic gastritis, Crohn’s dIsease and neoplasm (lymphoma and gastrointestinal stomal tumour) which can be differentiated by the histopathology [8].
Sometimes endoscopic mucosal resection is necessary to have a definitive diagnosis as simple endoscopic biopsy might not be adequate [2]. Histopathology of MD is similar in children and adults. Hypertrophy of gastric glands, cystic dilatation of glands deep in mucosa, inflammatory cell infiltration and thickened hyperplastic mucosa are the pathological hallmark [1, 9]. In the present case markedly hypertrophied foveolae with active gastritis and CMV inclusion bodies were found which clinched the diagnosis. In adults, MD can have a long clinical course and is associated with considerable morbidity and even mortality, which are related to surgical resection and potential risk for malignant transformation [10]. In most children, the disease resolves spontaneously and treatment is largely supportive, including adequate hydration and albumin transfusion. Treatment of CMV infection when indicated had shown good response. The present case improved well with supportive therapy without any antiviral. Some children, however, do not follow this course. In a case report a child with atypical Menetrier’s disease (non-protein losing) was treated successfully with octreotide [2]. Cetuximab, a monoclonal antibody against epidermal growth factor receptor (EGFR),(which is also a receptor for TGF) has been used as a treatment and resulted in almost normalization of gastric mucosal histology in 7 adults with the disease [11].
Conclusion
Menetrier’s Disease in children is a rare but mostly a benign, self limiting condition. In a few, disease course might be stormy like the present child. But full recovery is usually observed within 5-6 months.
References
-
Chouraqui JP, Roy CC, Brochu P, Gregoire H, Morin CL, et al. (1981) Menetrier's disease in children: report of a patient and review of sixteen other cases. Gastroenterology 80: 1042-1047.
-
Di Nardo G, Oliva S, Aloi M, Ferrari F, Frediani S, et al. (2012) Pediatric non-protein losing Menetrier’s disease successfully treated with octreotide long acting release. World J Gastroenterol 18(21): 2727- 2729.
-
Blackstone MM, Mittal MK (2008) The edematous toddler: a case of pediatric Ménétrier disease. Pediatr Emerg Care 24(10): 682–684.
-
Canan O, Ozcay F, Bilezikci B (2008) Menetrier’s disease and severe gastric ulcers associated with cytomegalovirus infection in an immunocompetent child: a case report. Turk J Pediatr 50(3): 291-295.
-
Larsen B, Tarp U, Kristensen E (1987) Familial giant hypertrophic gastritis (Menetrier’s disease).Gut 28(11):1517–1521.
-
Nomura S, Settle SH, Leys CM, Means AL, Peek RM, et al. (2005) Evidence for repatterning of the gastric fundic epithelium associated with Ménétrier’s disease and TGFalpha over expression. Gastroenterology 128(5):1292-1305.
-
Faure C, Besnard M, Hirsch A, Mougenot JF, Peuchmaur M, et al. (1996) Chronic hypertrophic gastropathy in a child resembling adult Menetrier’s disease. J Pediatr Gastroenterol Nutr. 23(4):419-421.
-
Kraut JR, Powell R, Hruby MA, Lloyd-Still (1981) JD Menetrier’s disease in childhood: report of 2 cases and a review of the literature. J Pediatr Surg 16(5):707-711.
-
Marks MP, Lanza MV, Kahlstrom E, Mikity V, Marks SC, et al. (1986) Pediatric hypertrophic gastropathy. AJR Am J Roentgenol 147(5):1031-1034.
-
Wolfsen HC, Carpenter HA, Talley NJ (1993) Menetrier’s disease: a form of hypertrophic gastropathy or gastritis? Gastroenterology 104(5): 1310-1319.
-
Fiske WH, Tanksley J, Nam KT, Goldenring JR, Slebos RJ, et al. (2009) Efficacy of cetuximab in the treatment of Menetrier’s disease. Sci Transl Med 1(8):8-18.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient