Prediction Model for Risk of Adenoma at Screening Colonoscopy
Aim: To identify risk factors for adenomatous polyps and develop an adenoma prediction model in individuals undergoing screening colonoscopy. Methods: We extracted demographic data, smoking history, current aspirin use and family history of colorectal cancer (CRC) as well as colonoscopy and histopathology results from individuals who underwent screening colonoscopy at the Minneapolis VA Medical Center between 2007 and 2012. Results: 3000 veterans were included. Adenomas were found in 1,063 patients (35%). Advanced adenomas were seen in 248 patients (8%). Risk factors for adenoma: age (OR 1.02, 95% CI 1.01, 1.03), male sex (OR 2.26, 95% CI 1.50, 3.52), and smoking (OR 1.53, 95% CI 1.29, 1.83). Risk factors for advanced adenoma: male sex (OR 3.79, 95% CI 1.18, 23.2) and smoking (OR 1.61, 95% CI 1.10, 2.34). Variables included in the final model were age, sex, BMI, race, use of aspirin, smoking history, and family history of CRC. The adjusted AUROCC for adenoma was 0.532 (95% CI 0.517, 0.554) and for advanced adenoma 0.613 (95% CI 0.564, 0.651). Conclusion: The model can be used to predict the risk of adenoma at screening colonoscopy and identify those patients who will benefit most from screening colonoscopy.
Core Tip
The model developed in this study predicts the risk of adenoma at screening colonoscopy and it represents a clinically useful stratification tool that could allow for targeted use of colonoscopy screening in patients at greatest risk. The model could be used by individual providers to counsel patients on screening options. Further it could be used by large healthcare organizations or national healthcare systems in resource poor areas to target high-risk populations for prioritized screening colonoscopy.
Introduction
Colorectal cancer (CRC) is the second leading cause of cancer-related death in the U.S [1]. CRC incidence and mortality vary significantly with age and gender. Family
history, smoking and obesity are risk factors for CRC [2, 3, 4], while ASA use may be protective [5]. Despite these known variations, current guidelines recommend CRC screening for everyone over age 50 [6, 7] which poses a significant burden on available resources. The American College of Physicians recommend that individualized risk assessment for CRC risk should be performed in all adults, and a screening modality should be selected based on individual risk [8]. However, no definitive way to assess the risk of CRC in individuals has been established. Adenomas are thought to be the precursor lesion in most CRC [9, 10, 11]. The 2008 U.S Multi-Society Task Force screening guidelines emphasized that the primary goal of screening should be prevention of CRC by detection and removal of asymptomatic adenomas [12]. Screening colonoscopy, which allows for the removal of precancerous lesions, has been shown to significantly decrease the risk of developing CRC [9]. Calculating individual risk of CRC is one way to risk stratify patients and prioritize CRC screening. Current available risk calculators for CRC include the Harvard Cancer Risk Index [13], a model from the National Cancer Institute (NCI) [14], and the CRC-PRO calculator [15]. These models require patient data, including age, sex, height, weight, tobacco use, alcohol use, aspirin use, non- steroidal anti-inflammatory drug (NSAID) use, consumption of red meat, milk, calcium/vitamin D supplement use, multivitamin use, exercise frequency, estrogen use, and years of education. Furthermore, these calculators are designed to predict the risk of developing CRC but do not predict the risk of adenoma. Several recent studies have reported scoring systems for advanced colorectal neoplasms for identifying patients most at risk and prioritizing screening colonoscopy [16, 17, 18, 19, 20, 21]. However, none of these studies evaluate the risk of adenoma. We have developed a risk score for adenoma in individuals undergoing screening colonoscopy [22]. The objective of this study was to develop a risk score in veterans undergoing screening colonoscopy at the Minneapolis VA Medical Center.
Materials and Methods
We performed a retrospective chart review of all patients who underwent screening colonoscopy at the Minneapolis Veterans Affairs Medical Center between 2007 and 2012. Incomplete colonoscopies or those with inadequate bowel prep were also excluded. The independent variables were age at colonoscopy, sex, race, BMI, smoking history, current use of aspirin, and history of colorectal cancer in at least one first-degree relative. The outcome variable was one or more adenomas or advanced adenoma/CRC found by the screening colonoscopy.
Statistical Analysis
Model parameters were used to calculate predicted probabilities and estimate an area under the receiver operating characteristic curve (AUROCC) [22]. The effects of these variables, along with interactions selected before model fitting, were estimated by logistic regression. Likelihood ratio tests, combining the main effects with the interaction effects, measured the overall effect of variables involved with interactions. The receiver operating characteristic curve (ROCC) was estimated with the convex hull approach [23], and the area under this curve (AUROCC) was computed. To mitigate bias induced by such reuse of the data, the bootstrap method for estimation of prediction error was applied [24]. Confidence intervals (CIs) for the adjusted estimates were produced by a second, outer bootstrap applied to the entire estimation and adjustment process, yielding a double bootstrap. To obtain adequate precision for the CIs, the outer bootstrap consisted of 2,000 iterations. The cumulative distribution of estimated risk was plotted to determine proportions of the population falling below any particular risk. The statistics were performed and reviewed by a biomedical statistician (R.S.) The predictive equation developed for adenoma is: logit[prob(Adenoma)] or log[p/(1-p)] = -1.545 + 0.019(age - 58.9) + 0.815(male) + 0.068(FDR with CRC) + 0.013(BMI - 27.6) + 0.428(ever smoker) - 0.31(non- white) - 0.04(aspirin user). The predictive equation developed for advanced adenoma is: logit[prob(Advanced Adenoma)] = -3.132 + 0.031(age - 58.9) + 0.533(male) + 0.002(FDR with CRC) + 0.012(BMI - 27.6) + 0.713(ever smoker) + 0.092(non- white) - 0.259(aspirin user).
Results
A total of 3000 veterans were included in the validation of the risk prediction model (Table 1).
| No adenoma | Adenoma | Total | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| (n=1937) | (n=1063) | (n=3000) | |||||||||
| Male | 1815 (94%) | 1033 (97%) | 2848 (95%) | ||||||||
| Median age (IQR) | 61 (56-65) | 62 (57-65) | 61 (57-65) | ||||||||
| White | 1556 (80%) | 822 (77%) | 2378 (79%) | ||||||||
| Black | 112 (6%) | 42 (4%) | 154 (5%) | ||||||||
| Other race | 40 (2%) | 19 (2%) | 59 (2%) | ||||||||
| Unavailable | 229 (12%) | 180 (17%) | 409 (14%) | ||||||||
| Median BMI (IQR) | 30 (26-34) | 30 (27-34) | 30 (27-34) | ||||||||
| Ever smoker | 461 (24%) | 324 (30%) | 785 (26%) | ||||||||
| Aspirin use | 1052 (54%) | 589 (55%) | 1641 (55%) | ||||||||
| FDR with CRC | 275 (14%) | 156 (15%) | 431 (14%) |
IQR: Intraquartile Range; BMI: Body Mass Index; FDR: First Degree Relative; CRC: Colorectal Cancer Complete data on all seven variables was available in 2963 patients (98.8%). Median age of this cohort was 61. The majority, 2848 (95%) were male and 2378 were white (79%). The median BMI was 30. A first degree relative with CRC was present in 14% of patients and in 6.3% of patients this FDR was age < 60 years of age at diagnosis. Adenomas were found in 1,063 patients (35%). 684 patients (22%) had a right-sided adenoma, defined as proximal to the splenic flexure. The vast majority of adenomas were tubular. Advanced adenomas (adenoma ≥ 10 mm, high-grade dysplasia, or villous adenoma) were seen in 248 patients (8%). Adenomas ≥ 10 mm were seen in 201 patients (7%). High-grade dysplasia and villous features were seen in 23 patients (0.8%) and 121 patients (4%), respectively. CRC was found in 13 patients (0.4%). Sessile serrated adenomas were seen in 100 patients (3%). The histopathology results are included in (Table 2).
| Histopathlogic results | n (%) | ||||
|---|---|---|---|---|---|
| ≥ 1 adenoma | 1063 (35%) | ||||
| Left sided adenoma | 606 (20%) | ||||
| Right sided adenoma | 664 (22%) | ||||
| Adenoma ≥ 10 mm | 201 (7%) | ||||
| High grade dysplasia | 23 (0.8%) | ||||
| Villous | 121 (4%) | ||||
| CRC | 13 (0.4%) | ||||
| One or more advanced adenomas (≥ 10 mm, high grade, villous, CRC) | 248 (8%) | ||||
| SSA | 100 (3%) |
CRC, colorectal cancer; SSA, sessile serrated adenoma Risk factors for any adenoma in our study included age (OR 1.02, 95% CI 1.01, 1.03), male sex (OR 2.26, 95% CI 1.50, 3.52), and smoking (OR 1.53, 95% CI 1.29, 1.83). A negative association was seen with non-white race (OR
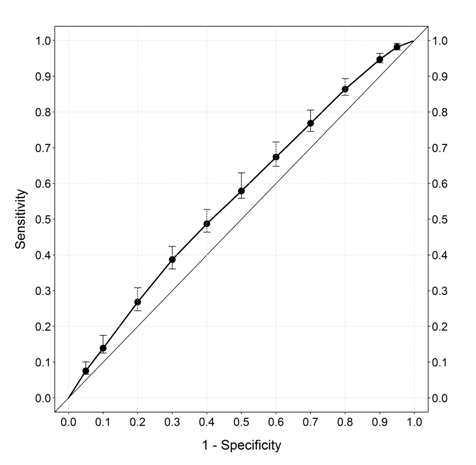
0.734, 95% CI 0.53, 0.99). Risk factors for advanced adenoma included only smoking (OR 2.04, 95% CI 1.53, 2.71). The adjusted AUROCC for any adenoma in the cohort was 0.563 (95% CI 0.517, 0.554) (Figure 1).
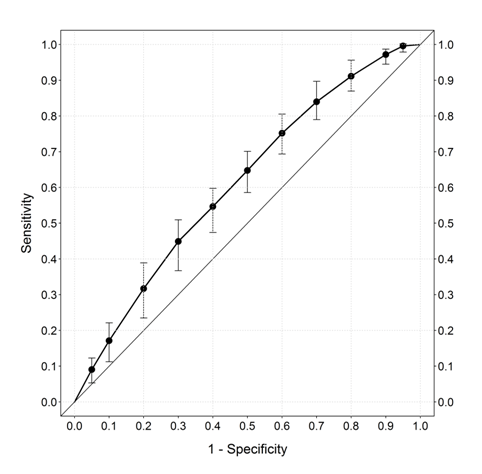
The adjusted AUROCC for advanced adenoma in the cohort was 0.613 (95% CI 0.564, 0.651) (Figure 2).
A plot of predicted risk of adenoma detection (horizontal axis) by fraction of the population at or below that risk (vertical axis) is show in (Figure 3).
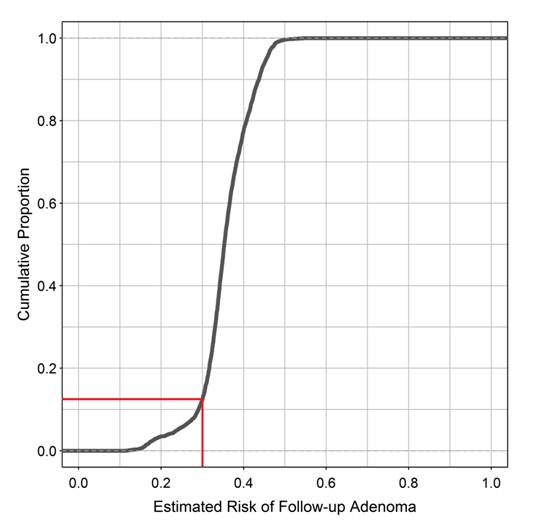
This figure illustrates the model’s impact and potential use in clinical practice. For example, if we define high-risk as individuals where predicted probability of an adenoma is >0.3, 87% are classified as high-risk. This classification would accurately capture 92% of all adenomas. Of the high-risk individuals undergoing colonoscopy, adenoma would likely be found in 37% (28.3% adenoma and 8.7% advanced adenoma) improving the number of therapeutic screening colonoscopies. Of the entire cohort 8% of patients with adenoma would not be prioritized for colonoscopy initially.
Discussion
We developed a risk model in a cohort of veterans undergoing screening colonoscopy. While this study did not compare screening colonoscopy to other screening modalities the results are the first step towards allowing payers, patients and physicians to use risk thresholds to decide whom to offer screening colonoscopy and whom to offer other screening modalities, or which individuals should be prioritized for screening colonoscopy based on estimated risk of harboring adenoma. Our AUC are low (0.56 and 0.61 respectively). While this may be the case the data points used in calculating risk of adenoma and simple and easy to collect. The model could be improved with future studies of a larger, more diverse population. A detailed history of aspirin and NSAID use in addition to pack years and family history via a prospective database would enhance the model. However, this approach is still an improvement on the current practice of informing screening decisions. As illustrated in (Figure 3), a selected threshold for the cumulative probability of harboring adenoma can be used to stratify patients for colonoscopy. For example, if we set the risk threshold for harboring an adenoma at > 0.3, the cumulative fraction of the population below this cut-off would be 13%. This population would be offered less invasive screening, such as fecal occult blood test or even no screening. Only 87% of the population would be prioritized to screening colonoscopy. Of course, the actual cut-off for predicted risk would have to be based on a careful analysis and comparison of cost-effectiveness for each potential cut- off, or multiple cut-offs. Risk factors for adenoma in our study included age, male sex, and smoking. Increasing age and male sex have been consistently associated with risk of adenoma [16, 19, 20, 21]. A negative association was seen with non-white race in our study, but the association with race has been inconsistently observed in other studies [25, 26, 27, 28]. No differences were seen with FDR with CRC. The literature is mixed on the influence of FDR. While some have found an association with FDR [19, 20, 26], others have found no association [29]. Aspirin use was not associated with adenoma risk in our study which is consistent with other studies [19]. Risk factors for advanced adenoma in our study included only smoking. Currently, three models are available in the US to predict the risk of CRC and several published studies estimating the risk of advanced neoplastic adenomas. However, none predict the risk of adenoma [13, 14, 15]. These models are complicated and require data points that can only be supplied by focused patient interview, and many of these variables are subject to recall bias. An ideal model would not only assess adenoma risk rather than colon cancer risk when stratifying patients for colon cancer screening by colonoscopy but would also include only objective risk factors easily identified by electronic chart review and exclude prior endoscopic findings. Two international studies attempted to predict the risk of advanced neoplastic adenoma by including prior endoscopy and history of colonic polyps as risk factors [16, 17]. A South Korean study also evaluated a model that initially does not rely prior endoscopy findings but is recalculated to incorporate flexible sigmoidoscopy findings after low-risk patients undergo flexible sigmoidoscopy [18].
Other studies have calculated risk of adenoma without relying on endoscopic findings. A Polish study used readily identifiable objective risk factors similar to ours: age, sex, BMI, smoking history and FDRs with CRC. Points were assessed for the various risk factors with scores ranging from 0 to 7-8. The risk of detecting advanced neoplasia on screening colonoscopy ranged from 1.32% for patients with a score of 0 up to 19.12% for patients with score of 7-8 [19]. Two additional studies from Asia assess the risk of advanced neoplastic adenoma. One includes readily identifiable risk factors similar to the Polish model [20]. Another from China relied on dietary factors and other risk factors not previously validated such as the consumption of pickled and fried food [21]. It is not clear that these models are applicable to the US population. The variables in our model are relatively easy to obtain and not subject to recall bias. In the future we envision the electronic medical chart to be able to automatically calculate a risk score for individuals that are screen eligible, to inform the discussion between providers and patients. The impact of such a score on screening uptake and decisions needs to be studied. A risk score has other applications, such as, colonoscopy scheduling could be modified to allow for greater time in patients at higher risk of adenoma who might require longer procedure times for polypectomy. Strengths of our study include a large sample size undergoing high quality colonoscopic evaluation as judged by prep quality, adenoma detection rate and withdrawal time. The prep was at least adequate in every colonoscopy. Further the adenoma detection rate in our study of 35% and withdrawal time of eight minutes greater than the established guidelines for determining high-quality colonoscopy [30]. Limitations of our study include that ours is a single center design of mostly male patients. In addition, details on smoking history were limited and did not include pack years. Our study does not have information regarding second-degree relatives with CRC. NSAID use was also missing from this cohort. Further studies from multiple centers with increased diversity would allow for more generalizable results and a prospective study would eliminate potential bias by allowing for more accurate and detailed collection of risk factors (such as NSAID use and second degree relatives with CRC). These factors would strengthen and enhance the model.
Conclusion
The development of a straightforward, clinically useful risk stratification model will allow for the targeted use of colonoscopic screening in patients at greatest risk. The model could be used by individual providers to better counsel patients and large healthcare organizations could use the model to target high-risk populations for prioritized screening colonoscopy.
Acknowledgements
The authors would like to acknowledge the Masonic cancer Center, University of Minnesota and Center for Chronic Disease Outcomes Research, a VA HSR&D Center of Innovation for their grant support. Citation: Hanson BJ, Shamsi N, Shanley R, Shaukat A. Prediction Model for Risk of Adenoma at Screening Colonoscopy .
References
-
Siegel R, Naishadham D, Jemal A (2012) Cancer statistics. CA Cancer J Clin 62(1): 10-29.
-
Verla-Tebit E, Lilla C, Hoffmeister M, Brenner H, Chang-Claude J, et al. (2006) Cigarette smoking and colorectal cancer risk in Germany: a population-based case-control study. Int J Cancer 119(3): 630-635.
-
Giovannucci E, Rimm EB, Stampfer MJ, Colditz GA, Ascherio A, et al. (1994) A prospective study of cigarette smoking and risk of colorectal adenoma and colorectal cancer in U.S. men. J Natl Cancer Inst 86(3): 183-191.
-
Doubeni CA, Major JM, Laiyemo AO, Schootman M, Zauber AG, et al. (2012) Contribution of behavioral risk factors and obesity to socioeconomic differences in colorectal cancer incidence. J Natl Cancer Inst 104(18): 1353-1362.
-
Flossmann E, Rothwell PM (2007) Effect of aspirin on long-term risk of colorectal cancer: consistent evidence from randomised and observational studies. Lancet 369(9573): 1603-1613.
-
Screening for colorectal cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med (2008) 149(9): 627-637.
-
Rex DK, Johnson DA, Anderson JC, Schoenfeld PS, Burke CA, et al. (2009) American College of Gastroenterology guidelines for colorectal cancer screening. Am J Gastroenterol 104(3): 739-750.
-
Qaseem A, Denberg TD, Hopkins RH, Humphrey LL, Levine J, et al. (2012) Screening for colorectal cancer: a guidance statement from the American College of Physicians. Ann Intern Med 156(5): 378-386.
-
Winawer SJ, Zauber AG, Ho MN, O'Brien MJ, Gottlieb LS, et al.(1993) Prevention of colorectal cancer by colonoscopic polypectomy. The National Polyp Study Workgroup. N Engl J Med 329(27): 1977-1981.
-
Winawer SJ, Zauber AG, Stewart E, O'Brien MJ (1991) The natural history of colorectal cancer. Opportunities for intervention. Cancer 67(4): 1143- 1149.
-
O'Brien MJ, O'Keane JC, Zauber A, Gottlieb LS, Winawer SJ, et al. (1992) Precursors of colorectal carcinoma. Biopsy and biologic markers. Cancer 70(5): 1317-1327.
-
Levin B, Lieberman DA, McFarland B, Andrews KS, Brooks D, et al. (2008) Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. Gastroenterology 134(5): 1570-1595.
-
Colditz GA, Atwood KA, Emmons K, Monson RR, Willett WC, et al. (2000) Harvard report on cancer prevention volume 4: Harvard Cancer Risk Index. Risk Index Working Group, Harvard Center for Cancer Prevention. Cancer Causes Control 11(6): 477-488.
-
Freedman AN, Slattery ML, Ballard-Barbash R, Willis G, Cann BJ, et al. (2009) Colorectal cancer risk prediction tool for white men and women without known susceptibility. J Clin Oncol 27(5): 686-693.
-
Wells BJ, Kattan MW, Cooper GS, Jackson L, Koroukian S, et al. (2014) Colorectal cancer predicted risk online (CRC-PRO) calculator using data from the multi- ethnic cohort study. J Am Board Fam Med 27(1): 42- 55.
-
Tao S, Hoffmeister M, Brenner H (2014) Development and validation of a scoring system to identify individuals at high risk for advanced colorectal neoplasms who should undergo colonoscopy screening. Clin Gastroenterol Hepatol 12(3): 478-485.
-
Imperiale TF, Juluri R, Sherer EA, Glowinski EA, Johnson CS, et al. (2014) A risk index for advanced neoplasia on the second surveillance colonoscopy in patients with previous adenomatous polyps. Gastrointest Endosc 80(3): 471-478.
-
Park HW, Han S, Lee JS, Chang HS, Lee D, et al. (2012) Risk stratification for advanced proximal colon neoplasm and individualized endoscopic screening for colorectal cancer by a risk-scoring model. Gastrointest Endosc 76(4): 818-828.
-
Kaminski MF, Polkowski M, Kraszewska E, Rupinski M, Butruk E, et al. (2014) A score to estimate the likelihood of detecting advanced colorectal neoplasia at colonoscopy. Gut 63(7): 1112-1119.
-
Yeoh KG, Ho KY, Chiu HM, Zhu F, Ching JY, et al. (2011) The Asia-Pacific Colorectal Screening score: a validated tool that stratifies risk for colorectal advanced neoplasia in asymptomatic Asian subjects. Gut 60(9): 1236-1241.
-
Cai QC, Yu ED, Xiao Y, Bai WY, Chen X, et al. (2012) Derivation and validation of a prediction rule for estimating advanced colorectal neoplasm risk in average-risk Chinese. Am J Epidemiol 175(6): 584- 593.
-
Shaukat A, Shanely R, Kauff ND, O'Brien MJ, Mills GM, et al. (2015) Development and validation of a clinical score for predicting risk of adenoma at screening colonoscopy. Cancer Epidemiol Biomarkers Prev 24(6): 913-920.
-
Provost F, Fawcett T (1997) Analysis and Visualization of Classifier Performance: Comparison under Imprecise Class and Cost Distributions. Proceedings of the Third International Conference on Knowledge Discovery and Data Mining (KDD-97).
-
Efron B, Tibshirani R (1993) An Introduction to Bootstrap New York: Chapman and Hall.
-
Lebwohl B, Capiak K, Neugut AI, Kastrinos F (2012) Risk of colorectal adenomas and advanced neoplasia in Hispanic, black and white patients undergoing screening colonoscopy. Aliment Pharmacol Ther 35(12): 1467-1473.
-
Lieberman DA, Prindiville S, Weiss DG, Willett W (2003) Prindiville S, Weiss DG, Willett W, Group VACS. Risk factors for advanced colonic neoplasia and hyperplastic polyps in asymptomatic individuals. JAMA 290(22): 2959-2967.
-
Thoma MN, Jimenez Cantisano BG, Hernandez AV, Perez A, Castro F, et al. (2013) Comparison of adenoma detection rate in Hispanics and whites undergoing first screening colonoscopy: a retrospective chart review. Gastrointest Endosc 77(3): 430-435.
-
Corley DA, Jensen CD, Marks AR, Zhao WK, de Boer J, et al. (2013) Variation of adenoma prevalence by age, sex, race, and colon location in a large population: implications for screening and quality programs. Clin Gastroenterol Hepatol 11(2): 172-180.
-
Lynch KL, Ahnen DJ, Byers T, Weiss DG, Lieberman DA, et al. (2003) First-degree relatives of patients with advanced colorectal adenomas have an increased prevalence of colorectal cancer. Clin Gastroenterol Hepatol 1(2): 96-102.
-
Rex DK, Petrini JL, Baron TH, Chak A, Cohen J, et al. (2006) Quality indicators for colonoscopy. Gastrointest Endosc 63(4): S16-28.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient