Carcinoma Colon in a Patient with Eosinophilic Gastroenteritis: A Case Report
Eosinophilic gastroenteritis is an uncommon disease which can involve all layers of the gastrointestinal tract anywhere from the esophagus to colon. Clinical features depend upon the site of involvement and layer of GI tract involved. It is an inflammatory disease with remitting and relapsing course. We report a case which presented with discharging fecal fistula in lower abdomen after emergency laparotomy. Initial colonoscopy showed stricture with nodularity of the IC junction and biopsy showed features of eosinophilic gastroenteritis. Due to persistence of fistula he underwent right hemicolectomy with illeo-transverse anastomosis. Biopsy from surgical specimen showed well differentiated adenocarcinoma and eosinophilic infiltrate in muscular is. Surveillance colonoscopy done six months later showed ulcer at anastomotic site and biopsy showed features of eosinophilic colitis. The clinical course of this patient circumstantially indicates a linkage of eosinophilic colitis with carcinoma colon. This is the first reported case of association of eosinophilic colitis with carcinoma colon. We discuss in detail the clinical and pathological features of eosinophilic enteritis and possible mechanisms linking eosinophilic enteritis with carcinoma.
Introduction
Eosinophilic gastroenteritis (EG) is a heterogeneous disorder characterized by the presence of an eosinophilic infiltrate on histopathology involving one or multiple segments of the gastrointestinal tract from esophagus to the rectum [1]. It can involve all layers of GI tract (Mucosa, Submucosa, Muscularis and serosa) [2]. Clinical features are dependent on the site and layer of GI tract involved. EG has a remitting and relapsing course in about 45% patients [3, 4, 5]. Stricture formation has been reported with EG [6]. Inflammatory conditions with remitting and relapsing course like Ulcerative colitis (UC) and Crohn’s disease predispose to carcinoma. Despite being remitting relapsing inflammatory disease EG there is only one case report of association of EG with gastric cancer [7]. We report a case of eosinophilic gastroenteritis leading to adenocarcinoma colon. This is the first case report suggesting an association between Eosinophilic gastroenteritis and adenocarcinoma of colon.
Case Report
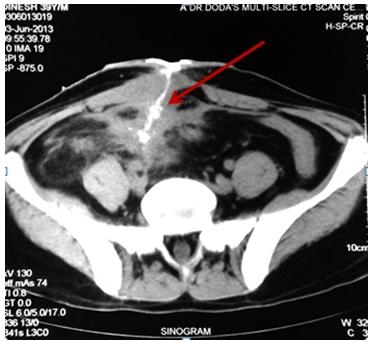
This 42 year old male who had undergone exploratory laparotomy a month ago for acute abdomen for suspected appendicular perforation, presented to us with complaints of passage of small amount (< 50 ml/day) of feculent discharge from lower margin of previous laparotomy site. A CT sinogram was done (Figure 1) which showed thickening of anterior abdominal wall at surgical site with small bowel loops adherent to the abdominal wall and contrast lined tract extending from terminal ileal loop to skin suggestive of enterocutaneous fistula.
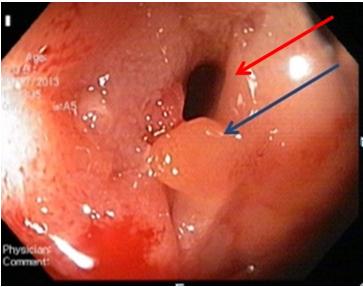
Colonoscopy was done which showed multiple nodules in the caecum with narrowing of illeocecal junction (Figure 2).
Biopsy showed eosinophilia in lamina propria (>30/ hpf) with focal cryptitis with absence of any epithelioid cells, granuloma or malignant cells (Figure 3A & 3B).
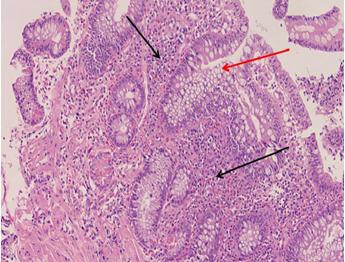
Figure 3A: Pre-operative biopsy from caecal nodules showing distorted crypt architecture (Red arrow) with dense lymphoplasmacytic infiltrates up to muscularis mucosa (Black arrow).
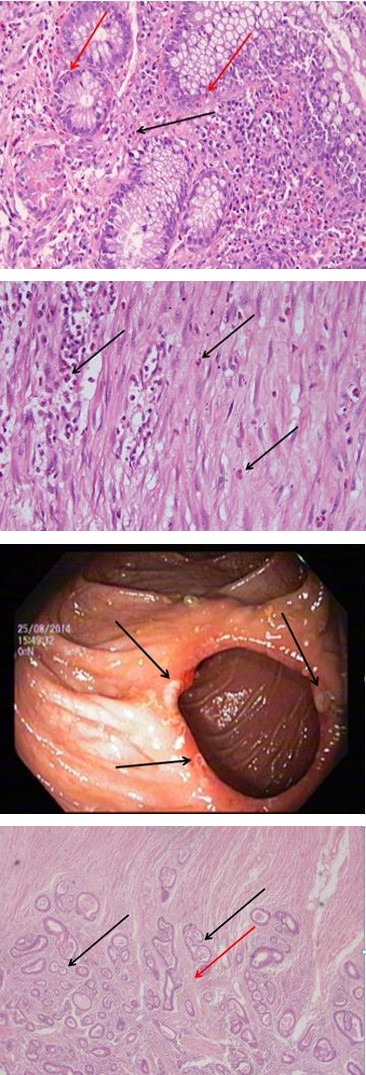
Figure 3B: High power view of pre-operative biopsy from caecal nodules showing dense eosinophilic infiltrates (Black arrow) (>30/hpf) and focal eosinophilic cryptitis (Red arrow).
Except mild anemia other hematological and biochemical parameters were normal. On review of past history he had intermittent small volume diarrhea without blood, pain abdomen, poor appetite and weight loss since past 4 years. There was no history of allergy, atopy or asthma. Montoux test was positive (26mm of induration at 48 hours) but GENE probe assay for tuberculosis was negative. ASCA (Anti-Saccharomyces Cerevisiae Antibody) was negative. In view of illeocecal stricture and persistent fistula he was operated and right hemicolectomy with illeotransverse anastomosis was done. Histopathology of the resected specimen showed a well differentiated adenocarcinoma with tumor infiltrating the muscularis (pT2), proximal and distal margins were tumor free and lymph nodes were free of any malignancy. Eosinophil counts were raised in the muscularis layer of the resected specimen (>30/hpf) (Figure 4A & 4B).
Figure 4A: Microscopic examination of surgical resected specimen showing disorganized glandular architecture (Black arrow) with well differentiated tumor extending into muscle coat (Red arrow).
Figure 4B: High power view of surgical resected specimen showing eosinophilic infiltrates in muscle layer (black arrows).
The diagnosis considered was colonic malignancy with perforation and subsequently fecal fistula formation and stricture. Post-operatively patient recovered well and received 12 cycles of chemotherapy comprising Oxaplatin and 5- fluorouracil. 6 months post-surgery surveillance colonoscopy was done which showed ulcers at the anastomotic site with normal colonic mucosa (Figure 5).
Biopsy from these ulcers showed a dense inflammation of lymphocytes, plasma cells and eosinophils (>20/hpf) in lamina propria, with no evidence of any granuloma or malignancy (Figure 6).
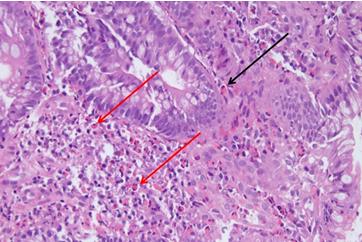
Figure 6: Histological sections of anastomotic site ulcers showing numerous eosinophilic infiltrates (Black arrows) upto lamina propria. His peripheral eosinophil count was normal. In view of persistent tissue eosinophilia in absence of any other underlying cause a diagnosis of eosinophilic gastroenteritis was made. He was started on prednisolone and showed a good clinical response in the symptoms of intermittent diarrhea which he had previously. The presence of eosinophils in caecal stricture before surgery, demonstration of eosinophils in operated specimen and recurrence of anastomotic ulcers with features of eosinophilic gastroenteritis suggest that EC was the underlying predisposing factor leading to carcinoma colon in this patient.
Discussion
First reported by Kaijser in 1937 [8]. EG is rare, with an approximate incidence of 1/100,000. It commonly occurs between second and sixth decade of life [9]. Stomach (26% to 81%) and small intestine (28% to 100%) are the predominantly affected areas, but the esophagus, large intestine, and rectum are also affected [10]. Eosinophilic gastroenteritis has been classified on the basis of depth of infiltration by Klein into mucosal EG, muscular EG and serosal EG [11]. Mucosal involvement is most common (57.5%), followed by muscular (30%) and serosal (12.5%) [9]. Another study has reported the distribution of EG as 44% (19/43) mucosal, 12% (5/43) muscular, and 39% (31/43) serosal [12]. The current accepted criteria for diagnosis of EG are as follows: (a) Presence of recurrent gastrointestinal symptoms (b)Biopsies with a histopathology showing predominant eosinophilic infiltration with sheets of eosinophils.
(c) Absence of parasitic or extra intestinal diseases that may cause eosinophilia [9]. Clinical presentation depends on the layer of GI tract and the site involved. Mucosal EG presents with abdominal pain, nausea, diarrhea, anemia or protein loosing enteropathy. Muscular EG presents as intestinal obstruction, intussusception and gastric outlet obstruction. Rarely may it present as intestinal strictures. Serosal EG typically presents as ascites [13]. Klein et al postulated that direct contact of the allergen with the mucosa initiates an antigen-antibody reaction which leads to release of various cytokines and particularly eotaxin which acts as a chemotactic signal for eosinophils. Thus the disease initiation occurs primarily in the mucosal layer and as the disease activity progresses deeper layers get involved and there is transmural involvement. But in some patients it is seen that the mucosal layer may be not involved and other layers show involvement. It is hypothesized that initially all layers may be involved but after a point of time due to undefined immunological preference the eosinophils remain limited to a particular layer/layers. Thus although the term mucosal, muscular and serosal layers are used, it does not indicate a specific or limited involvement of a particular layer but signifies the predominant layer of involvement of the disease and the inflammatory process with the possibility that transmural involvement may exist [11, 12]. In a recent study of 59 patients the distribution of mucosal, muscular and serosal disease was 52, 3 and 4 respectively [14]. To explain the predominant mucosal involvement it is postulated that EG involves an inward- out pathway in which there is initial involvement of the mucosa and as the disease progresses the deeper layers of the gut wall get involved. Earlier the clinical suspicion for this disease entity was low and the diagnosis was usually made on surgically resected biopsies when specimens were removed for features of obstruction or when patients presented with ascites. In view of higher suspicion now and ease of taking endoscopic biopsies which are predominantly mucosal likely the disease spectrum is shifting towards mucosal disease [14]. Our patient had involvement of both mucosal and muscular layer as both endoscopic and operative biopsies showed eosinophilic infiltrate. Stricture formation and obstruction is the hallmark of muscular layer involvement. Endoscopic findings in patients with eosinophilic gastroenteritis are not specific and include erythema, focal erosions, ulcerations, and pseudopolyps. Endoscopic abnormalities in EG are most striking in the mucosal form, and include thickening of folds, erythema, and friability [15]. Histological criteria for diagnosis in terms of number of eosinophils / HPF may vary according to the site of disease. Eosinophilic esophagitis is defined as eosinophil count more than 15/hpf, but in small bowel a higher cut- off is taken as eosinophil count may be upto 30 eosinophils/hpf in the appendix, terminal ileum, cecum, and proximal colon [16]. Degranulated eosinophils are noted in the intestinal mucosa accompanying histologic damage in EG. Diagnosis of EG may be elusive because of patchy disease distribution or the mucosa being spared altogether in muscular EG. Laparoscopy or open surgical exploration may be required for establishing the diagnosis of muscular disease. Serosal EG may be diagnosed by ascitic fluid examination. The fluid composition in serosal eosinophilic enteritis is mostly protein-rich (median, 43 g/L; range, 30 – 86 g/L), with high leucocyte count (median, 6200/mm3; range, 1300 – 20,500/mm3) and a large proportion of eosinophils (median, 78%; range, 39%–96%) [13]. EG is associated with asthma and allergies in 40%-50% of the cases. Association with peripheral eosinophilia is seen in about 80% of the cases but is not a prerequisite for diagnosis. In the mucosal and serosal types of the disease, a history of atopy is common and does not occur in the muscular type [17]. Mucosal eosinophilic infiltrates can be seen in parasitic infections, H. pylori infestation, connective tissue disorders, vasculitis, intestinal polyps, hyper eosinophilia syndrome, inflammatory bowel disease, celiac disease and post solid organ transplantation with immunosuppression. Our patient did not have any history of allergies or asthma. There was no peripheral eosinophilia. ANA was negative. IgA TTG was negative. Serology testing for H. pylori was negative. Eosinophilic gastroenteritis is a chronic inflammatory relapsing and remitting disease. Three different patterns of disease course are observed - 1) Single flare 2) Recurrent flares 3) Continuous disease activity. Reported relapse rates vary among studies from 18-45% [3, 4, 5]. In a study of 43 patients and a median follow up of 13.1 years, spontaneous remission was observed in 40%, and relapse rates were 33% of all patients and 60% of patients who required corticosteroid therapy [12]. Risk of clinical relapse is lower with patients who have an initial spontaneous remission as compared with patients who need treatment at diagnosis. Hypereosinophilia at diagnosis is associated with increased risk of clinical relapses. Higher risks of relapses are associated with mucosal disease, proximal small intestinal disease and extensive disease. It has been observed that mucosal disease has a more continuous course, muscular disease has a recurring course and serosal usually present with a single flare [12].
Chronic inflammation in gastrointestinal tract is a known risk factor for carcinogenesis [18]. It plays a major role in development of colorectal cancer (CRC) in inflammatory bowel diseases (IBD) [19]. The severity of inflammation correlates with risk of development of dysplastic changes [20]. Various case reports of coexistence of tuberculosis with colonic carcinoma have been reported in literature [21, 22, 23]. The proposed pathogenic mechanism is chronic inflammatory state due to ulcerated lesions of intestinal tuberculosis which leads to carcinogenesis. Schistosomiasis has been implicated in development of colon cancer. The cause of tumorigenesis is postulated to be due to the either endogenously produced carcinogens, impairment of immunological surveillance by chronic immune-modulation, symbiotic action of other infective agents and the presence of schistosomal toxins [24]. Muscular type of EE due to its recurrent nature and stricture formation may serve as a risk factor of GI cancer. Probably due to rarity of disease there is only one case of cancer reported with EG. This is to the best of our knowledge the first case of carcinoma colon associated with EG. Presence of eosinophils in initial mucosal biopsy preoperatively, eosinophilic infiltrates in muscular layer from resected specimen and recurrence of ulcers at anastomotic site post-operatively which showed tissue eosinophilia indicate that this patient had eosinophilic gastroenteritis which lead to carcinoma colon. Eosinophils are a rich source of proinflammatory cytokines which play both protective and pathological effects in the gastrointestinal tract [25]. Eosinophil granules contain a crystalloid core composed of major basic protein (MBP -1) (and MBP-2), and a matrix composed of eosinophil cationic protein (ECP), eosinophil-derived neurotoxin (EDN), and eosinophil peroxidase (EPO). These cationic proteins have pro- inflammatory properties and are known to exert cytotoxic effects on epithelium [26]. Eosinophil-derived transforming growth factor-β is linked with epithelial growth, fibrosis, and tissue remodeling. Eosinophils also generate large amounts of the LTC4, which is metabolized to LTD4 and LTE4. These three lipid mediators increase vascular permeability [27]. In experiments with suspensions of cells from colonic carcinomas, it has been seen that that colonic carcinomas contain large numbers of eosinophils [28]. The infiltration of tumors with eosinophils does not necessarily parallel peripheral blood eosinophilia, although the two phenomenons can occur together. Eosinophilic infiltration is an independent favorable prognostic influence on outcome of colorectal cancer [29]. Eosinophils play a role in the host interaction with the tumor, perhaps by promoting angiogenesis and connective tissue formation adjacent to the cancer [30].
Conclusion
Eosinophilic gastroenteritis is a rare disorder with a wide spectrum of clinical presentation. A high index of clinical suspicion is required for its diagnosis. Increasing luminal assessment due to ease of gastrointestinal endoscopy and colonoscopy has lead to increased diagnosis of mucosal EG. Like other inflammatory disorders, EG may be a predisposing factor development of gastrointestinal malignancy. This is the first case report of carcinoma colon in EG and second published case report of gastrointestinal malignancy with EG.
References
-
Khan S, Orenstein SR (2008) Eosinophilic gastroenteritis. Gastroenterol Clin North Am 37(2): 333-348.
-
Kellermayer R, Tatevian N, Klish W, Shulman RJ (2008) Steroid-responsive eosinophilic gastric outlet obstruction in a child. World J Gastroenterol 14(14): 2270-2271.
-
Chen MJ, Chu CH, Lin SC, Shih SC, Wang TE (2003) Eosinophilic gastroenteritis: clinical experience with 15 patients. World J Gastroenterol (12): 2813-2816.
-
Lee CM, Changchien CS, Chen PC, Lin DY, Sheen IS, et al. (1993) Eosinophilic gastroenteritis: 10 years experience. Am J Gastroenterol 88(1): 70-74.
-
Jeon EJ, Lee KM, Jung DY, Kim TH, Ji JS, et al. (2010) Clinical characteristics of 17 cases of eosinophilic gastroenteritis. Korean J Gastroenterol 55(6): 361- 367.
-
Jagtap S, Nikumbh D, Kshirsagar A, Ahuja N (2012) Unusual presentation of eosinophilic enteritis as multiple strictures of small intestine. Clinics Pract 2(1).
-
Otowa Y, Mitsutsuji M, Urade T, Chono T, Morimoto H, et al. (2012) Eosinophilic gastroenteritis associated with multiple gastric cancer. Eur J Gastroenterol Hepatol 24(6): 727-730.
-
Kaijser R (1937) Zur Kenntnis der allergischen Affektioner desima Verdauungskanal von Standpunkt desima Chirurgen aus. Arch Klin Chir 188: 36-64.
-
Talley N, Shorter R, Phillips S, Zinsmeister A (1990) Eosinophilic gastroenteritis: a clinicopathological study of patients with disease of the mucosa, muscle layer, and subserosal tissues Gut 31(1): 54-58.
-
Mueller S (2008) Classification of eosinophilic gastrointestinal diseases. Best Pract Res Clin Gastroenterol. 22(3): 425-440.
-
Klein N,Hargrove R,Sleisenger M,Jeffries G (1970) Eosinophilic gastroenteritis. Medicine 49(4): 299- 320.
-
Pineton de Chambrun G, Gonzalez F, Canva J, Gonzalez S, Houssin L, et al. (2011) Natural History of Eosinophilic Gastroenteritis. Clinical Gastroenterology and Hepatology 9(11): 950-956.
-
Fenoglio LM, Benedetti V, Rossi C, Anania A, Wulhfard K, et al. (2003) Eosinophilic gastroenteritis with ascites: A case report and review of the literature. Dig Dis Sci 48(5): 1013-1020.
-
Chang J, Choung R, Lee R, Locke G, Schleck C, et al. (2010) A Shift in the Clinical Spectrum of Eosinophilic Gastroenteritis Toward the Mucosal Disease Type. Clin Gastroenterol Hepatol 8(8): 669-675.
-
Treiber G, Weidner S (2007) Eosinophilic Gastroenteritis. Clini Gastroenterol HepatolM 5(5):e16.
-
Lowichik A, Weinberg AG (1996) A quantitative evaluation of mucosal eosinophils in the pediatric gastrointestinal tract. Mod Pathol 9(2): 110-114.
-
Gonsalves N (2007) Food Allergies and Eosinophilic Gastrointestinal Illness. Gastroenterol Clin North Am 36(1): 75-91.
-
Ullman T, Itzkowitz S (2011) Intestinal Inflammation and Cancer. Gastroenterology 140(6): 1807-1816.
-
Itzkowitz S, Xianyang Yio (2004) Inflammation and Cancer IV. Colorectal cancer in inflammatory bowel disease: the role of inflammation. AJP: Gastrointestinal and Liver Physiology 287(1): G7- G17.
-
Rutter M , Saunders B, Wilkinson K, Rumbles S, Schofield G, et al. (2004) Severity of inflammation is a risk factor for colorectal neoplasia in ulcerative colitis. Gastroenterology 126(2): 451-459.
-
Isaacs P, Zissis M (1997) Colonic tuberculosis and adenocarcinoma: an unusual presentation. European Journal of Gastroenterology & Hepatology 9(9): 913- 915.
-
Comert F, Comert M, Kulah C, Taşcilar O, Numanoglu G, et al. (2006) Colonic Tuberculosis Mimicking Tumor Perforation: A Case Report and Review of the Literature. Dig Dis Sci 51(6): 1039-1042.
-
Chakravartty S, Chattopadhyay G, Ray D, Choudhury C, Mandal S (2010) Concomitant tuberculosis and carcinoma colon: Coincidence or causal nexus?. Saudi Journal of Gastroenterology 16(4): 292-294.
-
H Salim O, Hamid H, Mekki S, Suleiman S, Ibrahim S (2010) Colorectal carcinoma associated with schistosomiasis: a possible causal relationship. World J Surg Onc 8(1): 68.
-
Zuo L, Rothenberg M (2007) Gastrointestinal Eosinophilia. Immunol Allergy Clin North Am 27(3): 443-455.
-
Gleich GJ, Adolphson CR (1986) The eosinophilic leukocyte:structure and function. Adv Immunol 39: 177-253.
-
Phipps S, Ying S, Wangoo A, Ong Y, Levi-Schaffer F, et al. (2002) The Relationship Between Allergen- Induced Tissue Eosinophilia and Markers of Repair and Remodeling in Human Atopic Skin. J Immunol 169(8): 4604-4612.
-
Brattain MG, Kimball PM, Pretlow TG. Pitts AM (1977) Partial purification of human colonic carcinoma cells by sedimentation. Br J Cancer 35(6): 850-857.
-
Fernandez-Acenero M, Galindo-Gallego M, Sanz J, Aljama A (2000) Prognostic influence of tumor- associated eosinophilic infiltrate in colorectal carcinoma. Cancer 88(7): 1544-1548.
-
Samoszuk M (1997) Eosinophils and human cancer, Histol Histopathol 12(3): 807-812.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient