Endoscopic Obliteration of GI Fistulas with Cyanoacrylate Glue - Our experience
GI fistula as both Internal and enterocutaneous are important cause for morbidity post operatively. They cause significant mortality due to sepsis and Nutritional electrolyte disturbances. Many expensive modalities of endoscopic closure of persistent fistulas after conservative treatment developed. Cyanoacrylate glue Injection is less commonly done. Here we are sharing our experience with less expensive cyanoacrylate glue In GI fistulas. Good results with endoscopic therapy suggest that this technique is best in achieving closure.
Uma Devi M*, Gopal and Shravan Kumar P
therapy suggest that this technique is best in achieving closure.
Keywords: Conservative therapy; Cyanoacrylate Glue
Introduction
A fistula is an abnormal communication between two epithelialized surfaces. Enterocutaneous fistula (ECF), as the name indicates, is an abnormal communication between the small or large bowel and the skin. An ECF can arise from the duodenum, jejunum, ileum, colon, or rectum. An ECF, which is classified as an external fistula (as opposed to an internal fistula, which is an abnormal communication between two hollow viscera), is a complication that is usually seen after surgery on the small or large bowel and after trauma Indeed, more than 75% of all ECFs arise as a postoperative complication, whereas about 15-25% result from abdominal trauma or occur spontaneously in relation to cancer, irradiation, inflammatory bowel disease (IBD), or ischemic or infective conditions [1].
ECFs are a common presentation and despite advances in the management, they cause significant mortality (5- 20%), attributable to associated sepsis, nutritional abnormalities, and electrolyte imbalances. ECFs are usually classified into three categories, as follows Low- output fistula (< 200 mL/day), Moderate-output fistula (200-500 mL/day),High-output fistula (>500 mL/day) [2].
Skin excoriation is one of the complications that can lead to significant morbidity in patients with ECF. When the enteric contents are more fluid than solid, this becomes a difficult problem; the skin excoriation makes it difficult to put a collecting bag or dressings over the fistula, and more leakage leads to an increase in the excoriation.
Approach Considerations
The conventional therapy for an enterocutaneous fistula (ECF) in the initial phase is always conservative, because the majority of ECFs spontaneously close as a result of conservative therapy. However, patients who have an ECF with adverse factors, such as a lateral duodenal fistula, an ilea fistula, a high-output fistula, or a fistula associated with a diseased bowel, may require early surgical intervention. Because of morbidity and mortality endoscopic closure became important main stay in treatment Fistula closure tried with endoscopic injection of a variety of sealants: 1. Fibrin glue 2 Fibrin glue with Polygala tin plug 3.Autologous platelet-rich fibrin glue, 4. Bio design enterocutaneous fistula plug, 5 cyanoacrylate glue [3].
Cyanoacrylate Glue
Cyanoacrylates are a class of synthetic glues as monomers, which polymerizes in an exothermic reaction when in contact with a weak base such as blood. They have been extensively used in middle ear surgery, cartilage repairs, repair of cerebrospinal fluid leaks and in skin closure Interventional radiologists have used the polymers for embolization of aneurysms, AV malformations, fistulas. The application of glue is an established treatment for fistulas [1, 2].
Technique of Glue Injection
1ml of cyanoacrylate, was endoscopically injected through the fistula using sclerotherapy needle (22G) and a 2.5-mL glue syringe. We used acetone 4ml to push the solution from the syringe into the needle. Because the presence of moisture causes the glue to set, exposure to normal levels of humidity in the air will start polymerization occurring within seconds. However, by making the glue syringe containing the glue air-tight, we were able to inject the solution safely.
The procedure was repeated after 1 week until the fistula was closed. In all four patients, the esophageal fistulas were successfully closed with two endoscopic injections of cyanoacrylate Glue. Endoscopic injection of Cyanoacrylate glue is a feasible and safe procedure that may be effective for the treatment of non-healing esophageal fistulas and ECFs.
We report on three patients with intractable Chronic enter cutaneous fistulas (ECF) and one Esophageal who were successfully treated with endoscopic injection of cyanoacrylate glue.
- Case 1. Esophago pleural fistula following Posterior spinal surgery for Potts spine.
- Case 2. Colocutaneous fistula following Intestinal Obstruction surgery.
- Case 3. Ilea cutaneous fistula following Ilea resection surgery.
- Case 4: Recto cutaneous fistula following vaginal reconstructive surgery In all cases, the ECF was assessed by means of computed tomography (CT) and fistulography to rule out any intra-abdominal abscess, distal bowel obstruction, active bowel inflammation, or foreign body that would prevent the fistula from healing. Fistulography also provided information about the fistulous tract and the site of communication with the bowel.
Technique of Glue Injection
1ml of cyanoacrylate was endoscopically injected through the fistula using sclerotherapy needle (22G) and a 2.5-mL glue syringe. We used acetone 4ml to push the solution from the syringe into the needle. Because the presence of moisture causes the glue to set, exposure to normal levels of humidity in the air will start polymerization occurring within seconds. However, by making the glue syringe containing the glue air-tight, we were able to inject the solution safely.
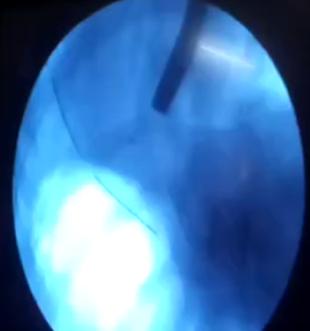
The procedure was repeated after 1 week until the fistula was closed. In all four patients, the esophageal fistulas were successfully closed with two endoscopic injections of cyanoacrylate Glue (Figures 1-3). Case 1: 35 yr old male with H/of potts spine and paraperesis operated for potts spine with anterior spinal fixation developed Short ness of breath and CXR revealed left sided pleural effusion. ICD inserted on left side and food particles drained from ICD tube, CECT chest revealed esophageal Pleural fistula.UGI endoscopy: fistulous opening at 35cms from incisors and 2cms above GE junction.
Patient was initially managed conservatively with Nasojejunal NJ tube feeds for one month, because of persistence of fistula cyanoacrylate glue injection done. Cyanoacrylate glue ingested into fistula in 2 sessions in a gap of 5 days. Complete closure achieved after 1 wk.
Case 2: 17 yrs old female presented with intestinal obstruction in 2010 and underwent sigmoid colostomy with Hartmann’s procedure. Later sigmoid colostomy closure and anastomosed was done postoperatively. pt developed feculent discharge from suture site in left iliac fossa and was managed conservatively fistulous output decreased but small quantity of discharge persisted. Patient presented to GE dept after 7yrs with feculent discharging enterocutaneous fistula.
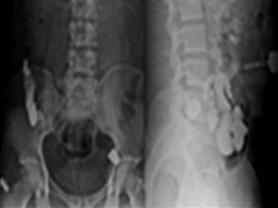
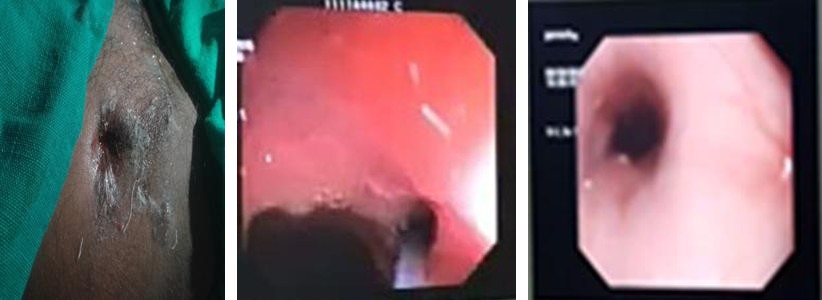
After adequate bowel preparation colonoscopy performed. Two fistulous openings identified at 15 and 18 cms from anal verge. Fistulous tract was demonstrated by Injecting methylene blue dye mixed with contrast from luminal site with use of cannula under fluoroscopy. spillage of dye noted from cutaneous opening and whole fistulous tract demonstrated on fluoroscopy.
Cyanoacrylate glue injected into First fistula closed in one session, 2nd fistula required 2 sessions for closure.

Figure 2: Fistulous opening methlene blue dye from fistula Catheter injecting glue. Case 3: 26 yr old male pt had Ileal perforation and underwent Ileal resection and end to end anastomosis, Later Pt Presented with Discharge from Scar Of drain site Since 1 Month. Examination revealed sinus tract noted in Right iliac fossa. Fistulogram opacified Ileal loops and jejunal loops.1ml of cyanoacrylate Glue Injected into the cutaneous orifice Of the Fistula in two sessions, after one week discharge stopped with closure of the fistula.

from anal verge (Figure 4). Cyanoacrylate glue injected into fistula in two sessions in a gap of 7 days. Complete closure achieved after 2 wk.
All patients tolerated the procedure well. Post procedure none of the patients developed fever, abdominal pain or bleeding.
Discussion
In our study all fistulas are developed post operatively, in various studies, more than 75% of all ECFs arise as a postoperative complication, whereas about 15- 25% result from abdominal trauma [1] in one study, about 95% of ECFs were postoperative, and the ileum was the most common site of ECF1. In our study 2 pts underwent ileal surgery. But fistula developed in ascending colon.
In 49% of fistulas were high-output, and 51% were low-output [3]. All our cases fistulas are small and low output fistulas.
Location of Fistulas
Spontaneous closure occurs in almost 70% of patients. In a study of 186 patients, Rebar et al found that 91% of small-bowel fistulas that closed spontaneously did so within 1 month after sepsis was cured. The remaining fistulas that closed spontaneously did so by the end of 3 months after sepsis cure, with the rest of the lesions requiring surgical closure [4]. Fistulas in GIT after ligament of Traits, and ileal fistulas have fewer tendencies to spontaneously close [5]. A Colocutaneous fistula can develop after colonic surgery, especially when the blood supply to a low colorectal/anal anastomosed is and is difficult to heal spontaneously
Route of Administration of Glue
Route is important in achieving the closure, when fibrin glue was introduced directly into an ECF through the fistula opening in the skin, the results were not encouraging, with the fistula healing in only one out of eight of pts [6]. In our study we have Injected Glue directly into the external orifice resulting in closure, we have injected externally in one pt, and internally in 3 pts.
When fibrin glue was introduced directly into an ECF through the fistula opening in the skin, the results was not encouraging, with the fistula healing in only one out of eight patients [7]. In our study we have Injected Glue directly into the external orifice resulting in closure, we have injected externally in one pt, and internally in 3 pts.
Good results with endoscopic therapy suggest that this technique is best in achieving closure.
Conclusion
GI Fistula after surgery is not uncommon. They Causes morbidity, sepsis and affects quality Of life. Endoscopic methods offers closure rates up to 90% with fewer complications. In Our experience of 4 cases fistula obliteration achieved with endoscopic Cyanoacrylate glue injection, with better results after 2-3 sessions. Endoscopic injection of Cyanoacrylate glue is safe, cost effective and with less morbidity, it is a feasible and safe procedure that may be effective for the treatment of non- healing esophageal fistulas and ECFs.
References
-
Cameron R, Binmoeller KF (2013) Cyanoacrylate applications in the GI tract. Gastrointestinal Endosc 77(6): 846-857.
-
Berry SM, Fischer JE (1996) Classification and pathophysiology of enterocutaneous fistulas. Surg Clin North Am 76(5): 1009-1018
-
Wu X, Ren J, GU G, Wang G, Han G, et al. (2014) Auto logous platelet rich fibrin glue for sealing of low- output entero cutaneous fistulas: an observational cohort study. Surgery 155(3): 434-441.
-
Yoon JH, Lee HL, Lee OY, Yoon BC, Choi SH, et al. (2009) Endoscopic treatment of recurrent congenital tracheoesophageal fistula with Histoacryl glue via the esophagus. Gastrointestinal Endosc 69(7): 1394-1396.
-
Reber HA, Roberts C, Way LW, Dunphy JE (1978) Management of external gastrointestinal fistulas. Ann Surg 188(4): 460-467.
-
Evenson AR, Fischer JE (2006) Current management of entero cutaneous fistula. J Gastrointest Surg 10(3): 455-464.
-
Rabago LR, Ventosa N, Castro JL, Marco J, Herrera N, et al. (2002) Endoscopic treatment of postoperative fistulas resistant to conservative management using biological fibrin glue. Endoscopy 34(8): 632-638.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient