Eosinophilic Gastroenteritis: 3 Cases and Review of Literature
Eosinophilic Gastroenteritis: Eosinophilic Gastroenteritis (EGE) is a rare disease affecting one or more segments of gastrointestinal tract, mainly stomach and small bowel with dense eosinophilic infiltration in gastrointestinal tract. It has a chronic clinical course. The patients may or may not have peripheral eosinophilia. The treatment of choice is a short course of corticosteroids. We present three cases of eosinophilic gastroenteritis with review of literature.
Introduction
Eosinophilic gastroenteritis (EGE) is a rare disease characterized by abdominal discomfort and dense eosinophilic infiltration in gastrointestinal tract found on histopathology on in the ascitic fluid. It presents with nonspecific abdominal pain and has a chronic clinical course with relapses and remission [1, 2]. Kaijsar first reported a case of EGE in 1937 [3, 4]. Its pathophysiology is unclear but most patients give history of food allergy.
Mucosal biopsies are adequate for the diagnosis with presence of more than 20 eosinophils per high power field. Mucosal biopsies may not be useful when there is ascites [1, 2, 5]. The patients may or may not have peripheral eosinophilia.
Three subtypes are described depending on layer involved (Klein’s classification) (1) Mucosal involvement presenting as nausea, vomiting, abdominal pain and diarrhoea, (2) Muscularis involvement presenting with features of obstruction and (3) Serosal involvement presenting with ascites [6, 7]. The treatment of choice is a short course of corticosteroids [8]. We report three cases of EGE, two presenting with ascites and one presenting with features of gastric outlet obstruction.
Case 1
An eighteen year old female presented with abdominal distention and pain of two weeks duration. She had nausea and infrequent episodes of vomiting. Her appetite was low and she experienced generalized weakness. There was no history of fever, skin rashes, passing worms, pedal oedema, jaundice, gastrointestinal bleed or any other significant past illness. Her bowel and bladder habits were normal.
Her vital parameters were normal. She had no icterus, lymphadenopathy, oedema or skin rashes. She had ascites, but no organomegaly. Other systems didn’t reveal any abnormality. Abdominal sonography showed thickened gastric wall and mild ascites.
Haematological investigations revealed Haemoglobin 13.1 gm%, Total Leucocyte count 21,500, with Absolute Eosinophil Count 18160, Platelet count 3,21,000 /cu mm. Liver, Kidney function tests and Serum Amylase were normal. Serum IgE was markedly elevated 4931 IU/L.
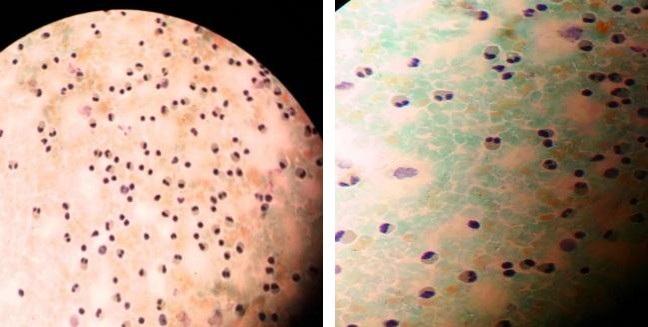
Ascitic tapping was done and revealed turbid fluid with 5000 cells/cu mm with 90% of eosinophils (Figure 1). Fluid proteins were 4.9 gm% with Albumin of 2.3 gm%. ADA was 3.95 IU/L and Amylase 21 IU/L. Stool examination revealed Occult Blood with unremarkable microscopy.
Gastroscopy showed antral gastritis and biopsy from gastric and duodenal mucosa showed eosinophilic infiltrate of 2-3 eosinophils/hpf. She was initially treated with Nitazoxanide 500 mg bid for three days, Rabeprazole 20 mg/day for seven days with diuretics. However, pain and vomiting persisted, hence Prednisolone 40 mg/day was started and tapered 10 mg/week over next four weeks. She made a dramatic recovery with ascites disappearing in three weeks with regression of symptoms. Absolute Eosinophil Count (AEC) dropped to 149 cells/ cu mm. Steroids were stopped in next two weeks with 10 mg alternate day dose. She is asymptomatic after one year follow up.
Case 2
A twenty year old male presented with epigastric pain and abdominal distention of three weeks duration. He vomited often but had no GI bleeding. His bowel and bladder habits were normal. He was investigated in another hospital and was found to have ascites with normal liver function tests. Haematological investigations revealed Haemoglobin 15 gm%, TLC 28,900 cells/cu mm with 61% Eosinophils, AEC 17629. Ascitic fluid Total leukocyte count was 9000 cells//cu mm with 95% Eosinophils, Proteins 4.8 gm%, ADA 10 IU/L and it was negative for malignant cells. He was treated with anti- tuberculous drugs, antibiotics and metronidazole elsewhere without any relief hence referred to us. Anti- tuberculous drugs were stopped and Prednisolone 40 mg/day was started and tapered every week by 10 mg along with Rabeprazole 20 mg/day. He made complete recovery within four weeks and ascites disappeared. There is no recurrence at eight month of follow up.
Case 3
A 46 year male presented with abdominal pain of three months duration, reduced appetite, 4 kg weight loss and vomiting. He was afebrile and his bowel, bladder habits were normal. Examination revealed mild pallor, no lymphadenopathy, no oedema. There was epigastric lump with visible peristalsis left to right.
Investigations showed Hb 12.6 gm%, TLC 17,900 cell/cu mm, AEC 1432/cu mm, Platelets 6.73 lac/cu mm, LDH 336 U/L, β2 micro globulin 2200. USG abdomen revealed marked thickening of gastric wall and peri pancreatic lymphadenopathy. OGD scopy showed marked thickening of oesophageal and gastric mucosal folds which were biopsied. RUT for H. Pylori was positive and treatment for the same was started. However, biopsy from the stomach was reported as Eosinophilic Gastroenteritis. Immunohistochemistry of biopsy did not reveal lymphoma or carcinoma. Prednisolone 40 mg/day was started, tapered by 10 mg every week.
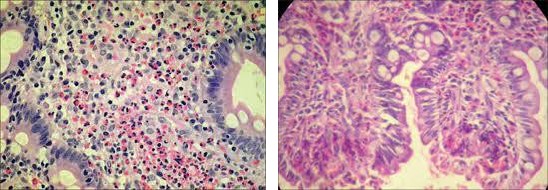
After one month of steroids, AEC dropped to 666, but there was no improvement in symptoms or USG appearance. Repeat OGD showed reduction in thickening of oesophageal folds, gastric and duodenal mucosa showed nodularity, CT abdomen revealed gastric wall thickening 37 mm, D1-D2 luminal narrowing and peri- gastric lymphadenopathy. Laparoscopy was done and true-cut biopsy from stomach and peritoneum revealed 50- to 75 eosinophils /HPF. No evidence of malignancy (Figure 2).
Steroid was restarted with slow tapering over 8 weeks. Patient had gradual improvement over one month and was asymptomatic with disappearance of lump. After three years of follow up, he remains asymptomatic and healthy.
Discussion
EGE is an uncommon condition due to eosinophilic infiltration of one or more segments of gastro- intestinal tract. Hollow organs are more commonly involved although involvement of Pancreas, Liver, is also described as case reports. EGE is common in second to fifth decade of life [7] and is more common in males, however serosal involvement and ascites is more common in females [6]. The clinical presentation depends on the organ involved and the layer involved. It can be vomiting, diarrhoea in mucosal involvement, obstruction in muscularis involvement and ascites in serosal involvement. Useful laboratory tests are complete blood count, absolute eosinophil count. Ultrasonography and C.T. scan of abdomen can reveal a mass or thickening of the walls of the organ involved. Endoscopy can be normal or show thickened folds, mucosal ulcerations. Mucosal biopsy and/or full thickness biopsy or ascitic fluid analysis are diagnostic. As the involvement can be patchy, multiple site biopsies are sometimes advised.
Before labelling any patient with EGE, one must rule out other causes of tissue eosinophilia like intestinal parasitic infestations, lymphoma, gastric malignancies, inflammatory bowel disease, collagen vascular disorders like Polyarteritis nodosa, Churg-Strauss syndrome [2, 7]. For the diagnosis of EGE, following four criteria are used [1, 3]. a. Presence of gastrointestinal symptoms b. Eosinophilic infiltration of one or more areas of gastrointestinal tract with more than 20 eosinophils/ high power field c. Exclusion of eosinophilia in other organs d. Absence of other cause of eosinophilia.
In our patients of ascites, mucosal biopsy was negative but ascitic fluid showed abundant eosinophils, this is common in serosal disease [6].
The patient, who presented with abdominal pain and signs of gastric outlet obstruction, had endoscopically malignant appearing lesion. The biopsy was inconclusive and hence repeat true - cut biopsy was performed which showed layers of stomach heavily infiltrated by eosinophils. This tells the importance of repeat biopsies.
Most of the patients respond well to corticosteroids. Patients can have relapse after omitting steroids. . In Eosinophilic ascites relapses are seen in 26% cases [2] Untreated, mucosal disease can progress to severe malabsorption. Two week treatment with Prednisolone 20 to 40 mg/day produces dramatic clinical improvement regardless of clinical subtype. Some may require long term treatment with low dose Prednisolone 5-10 mg/day. Steroid dependent cases can be treated with Azathioprine and 6 Mercaptopurine [2]. Montelucast a Leukotrienes inhibitor, Anti IgE antibody Omalizumab, Anti IL-5 antibody Mepolizumab have also been tried in small case series with variable results. Elimination diets if allergen is identified can be tried but are cumbersome to follow on long term.
References
-
Liao WH, Wei KL, Po Yen Lin, Wu CS (2012) A rare case of spontaneous resolution og eosinophilic ascites in a patient with primary eosinophilic gastroenteritis. Chang Gung Med J 35(4): 354-359.
-
Bliebel F, Fragoza K, Faller G (2012) acute eosinophilic ascites in a middle aged man. Case reports in gastrointestinal medicine 2012: 4.
-
Gupta P, Singla R, Kumar S, Singh N, Nagpal P, et al. (2012) Eosinophilic ascites, A rare presentation of eosinophilic gastroenteritis. J Assoc Physicians India 60: 53-55.
-
Patel NR, Joshipura VP, Naik RP, Patwari SI, Bhavsar MS (2009) Predominantly muscular eosinophilic gastroenteritis, with ascites A case report and review of literature The internet Journal of Gastroenterology 7(2): 53-55.
-
Hepburn IS, Sridhar S, Schade RS (2010) Eosinophilic ascites, an unusual presentation of eosinophilic gastroenteritis A case report and review. World J Gastrointest Pathophysiol 1(5): 166-170.
-
Elliot JA, Mc Cormack O, Tchrakian N, Mahmud N, Conlon N, et al. Eosinophilic gastroenteritis manifesting as eosinophilic ascites A case report. J Genet Syndr Gene Ther.
-
Fenoglia Preiser CM, Noffsinger AE, Stemmermann GN, Lantz PE (2008) Gastro Intestinal Pathology An atlas and text 3rd (Edn.), Lippincott, Hongkong 1999-1296.
-
Setia N, Ghobrial P, Liron P (2010) Eosinophilic ascites due to severe eosinophilic ileitis. Cyto journal 7: 19
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient