Life Long Experience Treating and Preventing Gastro-Esophageal Reflux
For over 60 years, we have operated upon several hundred patients suffering from gastroesophageal reflux and its complications. Three separate procedures have been devised, tested, applied, and followed for many years, both in the presence or surgical absence of the patient’s cardia.
Opinion
For over 60 years, we have operated upon several hundred patients suffering from gastroesophageal reflux and its complications. Three separate procedures have been devised, tested, applied, and followed for many years, both in the presence or surgical absence of the patient’s cardia. Our interest in esophageal surgery spans over 60 years. To judge the results of our operations we have been guided by Mr. Ronald Belsey’s edict: The correction of an anti-reflux procedure should be judged after no less than ten year follow-up, 9 (R. Belsey, personal communication, 1968).
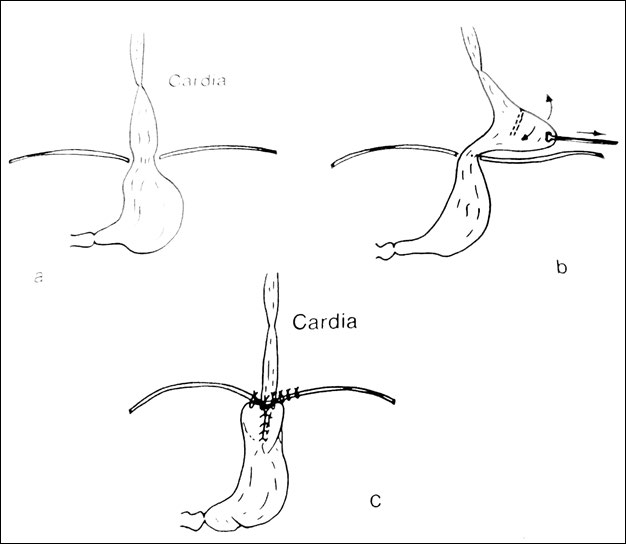
Fundoplication for correction of gastroesophageal reflux, introduced by Raloph Nissen, had become an important breakthrough for the correction of hiatal hernia Opinion [1]. Recurrence followed frequently enough due to slippage. Collis, in 1957, introduced a lengthening gastroplasty and fundoplication [2]. Since then, lengthening by transecting and suturing the cut edges prior to fundoplication because a widely accepted procedure [3].
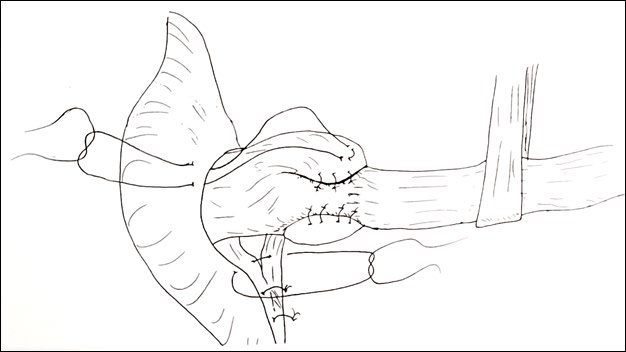
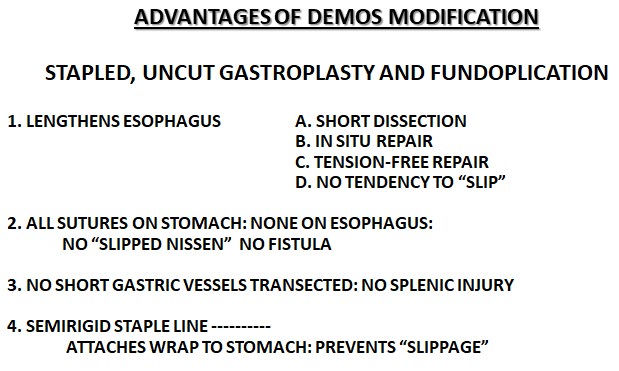
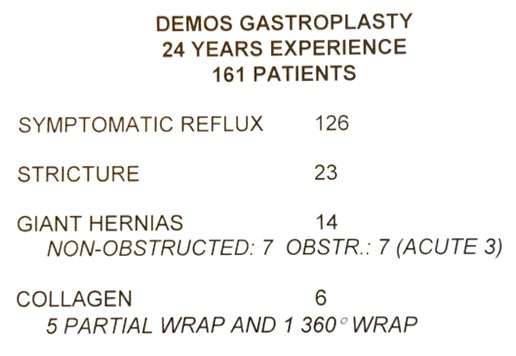
We introduced stapling of the fundus instead of transecting and suturing (Figure 1). Stapling saves time and is less likely to lead to leakage of the sutured edges. Figure 2 shows a partial fundoplication in a patient with abnormal esophageal peristalsis. Figure 3 shows the multiple advantages of the stapled, uncut gastroplasty. Our 24 years experiences with 161 patients with severe reflux and/or stricture revealed only one death, an emergency operation, and two symptomatic occurrences (Figure 4&5).
The Mayo Clinic has used this gastroplasty as the main procedure for reflux and its complications, (S. Payne, personal conversation, 1989). Our gastroplasty has been used through the chest or abdomen [4, 5]. A group of 24 patients were successfully operated upon using the video assisted technique [6].
The second procedure devised by us concerns recurrent achalasia with reflux and stricture. In three such patients we performed a Y-V Plasty and partial Fundoplicaton (Figures 6 & 7). This technique had been previously employed by Moschel and coworkers to correct pyloric stenosis, 8. Five year follow-up by our three patients revealed no dysphagia, reflux or esophagitis [7].
Our third anti-reflux procedure concerns patients with surgical absence of the cardia. Skinner and Belsey declared that “recurrent gastroesophageal reflux and stenosis is the most important late complication to follow reconstruction by intrathoracic esophagogastrostomy [8]. In fact, Wang and associates followed 368 patients after esophagogastrostomy and found that 5% if patients had succumbed fatally to pulmonary aspiration and 26% more suffered severely from reflux and aspiration [9].
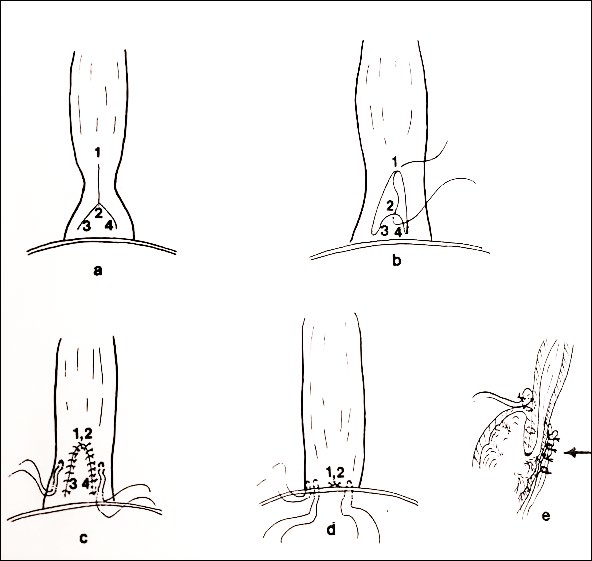
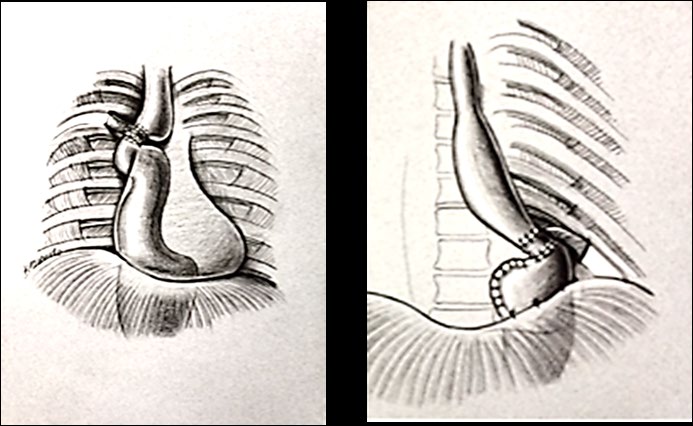
We thought a muscular pedicle around the esophagogastrostomy might provide protection form reflux. In my early resident years, I assisted our mentor, William J. Poth, construct a thigh muscular pedicle inserted subcutaneously around the anus to correct anal incontinence in young children [10, 11]. Indeed, an intercostal myo- nuerovascular pedicle did the work of a new cardia in patients with esophagogastrostomy, (Figure 8).
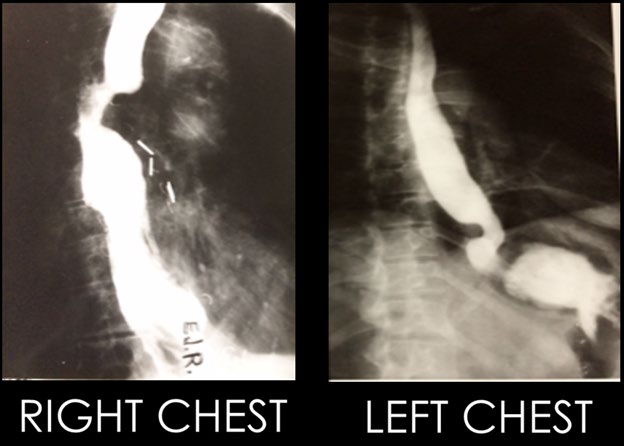
Technically, the pedicle procedure takes about 15 minutes to dissect thus adding very little to the much longer esophagogastrectomy, 17. The resulting pictures on the esophagus, Figure 5, are convincing as to the result of the pedicle. Certainly the 24-year study of our patients is convincing [12, 13, 14, 15, 16, 17].
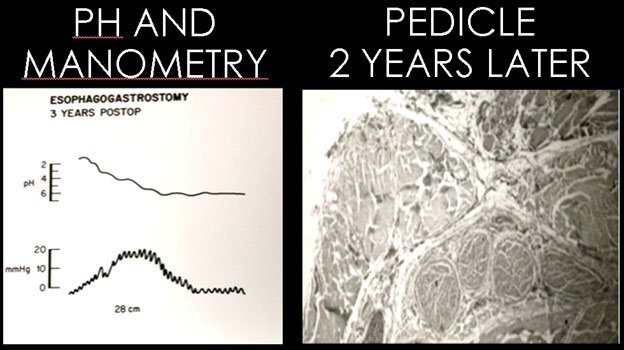
We believe that it’s not all pedicle, at least the majority of them continue to be viable. In one patient, dying of heart disease two years after the pedicle operation, the autopsy biopsy of the pedicle revealed viable muscle, nerves and vessels. Moreover, nanometric studies performed three years postoperatively active sphincteric pressure and acid to neutral pH changes at the “new cardia” level (Figure 9).
In my retirement, I can that we now have procedures to treat and protect our patients from the suffering of acid gastroesophageal reflux and its catastrophic or disabling complications.
References
-
Nissen R (1956) A simple operation for control of reflux esophagitis. Schweiz Med Wochenschr 86 (Suppl 20): 590-592.
-
Collis JL (1957) An Operation for Hiatus Hernia with Short Oesophagus. Thorax 12(3): 181-188.
-
Orringer MB, Orringer JS (1982) The Combined Collis-Nissen Operation: Early Assessment of Reflux Control. The Annals of Thoracic Surgery 33(6): 534-539.
-
Demos NJ (1999) The stapled, uncut gastroplasty for hiatal hernia: 24 years’ follow-up. Diseases of the Esophagus. 12(1): 14-21.
-
Demos NJ (1987) Transabdominal nissen fundoplication and stapled uncut gastroplasty. Surgical Rounds, pp: 114-116.
-
Demos NJ, Kulkarni VA, Arago A (1994) Video assisted transthoracic hiatal hernioplasty using stapled uncut gastroplasty and fundoplication. Surgical Rounds, pp: 427-436.
-
Demos N (1983 Y-V cardioplasty for recurrent achalasia. The American Surgeon 49(5): 282-284.
-
Skinner D, Belsey RHR (1988) Management of esophageal disease. PA: Saunders, Philadelphia.
-
Wang LS, Huang MH, Huang BS, Chien KY (1992) Gastric substitution for resectable carcinoma of the esophagus: An analysis of 368 cases. The Annals of Thoracic Surgery 53(2): 282-288.
-
Potts WJ (1959) The surgeon and the child. PA: WD Saunders, Philadelphia.
-
Pickrel K, Georgiade N, Richard EF, Morris F (1959) Gracilis muscle transplant for the correction of neurogenic rectal incontinence. Surgical Clinics of North America 39(5): 1405-1415.
-
Demos NJ, Kulkarni VA, Port A, Micale J (1992) Control of postresection gastroesophageal reflux; the intercostal pedicle esophagogastropexy experience of 26 years. American Gastroenterologic Association Am Surg.
-
Demos NJ, Kulkarni VA, Port A, Micale J (1993) Control of postresection gastroesophageal reflux; the intercostal pedicle esophagogastropexy experience of 26 years. The American Surgeon 59(3): 137-148.
-
Demos NJ, Kulkarni VA, Taha S (1995) Control of post- resection gastro-esophageal reflux by intercostal pedicle esophagogastropexy. Diseases of the Esophagus 8(2): 142-144.
-
Moschel DM, Walske BR, Newmayer F (1958) A new technique of pyloroplasty. Surgery 44(5): 813.
-
Demos NJ, Fowler B, Timmer JJ, Di Bianco J (1969) The intercostal pedicle method for the control of reflux esophagitis.. Clinical Research 17: 301.
-
Demos NJ, Biele RM (1980) Intercostal pedicle method for control of postresection esophagitis. The Journal of Thoracic and Cardiovascular Surgery 80(5): 679-685.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient