Emergency Endoscopic Management of Pediatric Upper Gastrointestinal Tract Foreign Bodies: A North Indian Study
1.1. Introduction: Ingestion of a foreign body (FB) is a common pediatric emergency seen in daily clinical practice all over. Scarce data on this problem is available from this part of the world. 1.2. Methods: We present our experience over four years about the spectrum of foreign bodies presenting to a gastrointestinal endoscopy (GI) centre and their subsequent management. Data was collected from all consecutive patients with FB ingestion presenting to our endoscopy center from January 2015 to December 2018. The demographic data, clinical presentation and endoscopic management was reviewed and analyzed. 1.3. Results: A total of 130 patients with suspected FB ingestion underwent endoscopic management. 130 FBs were found in 130 patients with suspected FB. Scarf pin was most common type seen in 69 % cases followed by coins in 10.7 % cases. Button battery was noted in 7.7 % patients. Most of the FBs were located in the stomach (69 %) followed by esophagus (13.8 %). The majority of patients (94.4 %) were successfully removed with flexible endoscopy with the addition of suitable devices without any serious procedure-related or anesthesia -related complications. 1.4. Conclusion: In this part of the world the pattern and types of Upper gastrointestinal (UGI) tract foreign bodies in pediatric population is unique not seen elsewhere across the globe. Early endoscopic management was found to be highly safe and efficacious.
Introduction
Foreign body (FB) ingestion is a common problem in gastroenterology practice and a very common indication for emergency endoscopy among children [1]. The majority of GI tract foreign bodies are seen in pediatric population with a peak incidence between six months to six years of age [2]. FB ingestion represents a significant clinical difficulty in pediatric gastroenterological practice. In 2000 the American Association of Poison Control Centers documented that 75% of the >116,000 ingestions reported were in children 5 years of age or younger [3].
About 98% of FB ingestion cases are unintentional. Most FBs in children are coins, toys, magnets and batteries [4, 5]. Majority of the FBs that reach the GI tract will pass spontaneously. However 10% to 20% of the cases will require non-operative intervention and 1% or less will need surgery [6].
Most of the cases are brought to the medical attention by the caregivers following a witnessed or reported ingestion. Child may be asymptomatic or may present with refusal to feed, dysphagia, drooling or respiratory signs like wheezing stridor or choking. Older children may be able to localize the sensation of something stuck in the neck or lower chest suggesting the irritation of upper or lower esophagus, respectively.
Management of GIT FBs depends on the facilities and local expertise available at a particular centre. Flexible endoscopy has become the diagnostic and therapeutic approach of choice in the management of FBs in the upper GI tract in both the pediatric and adult population. Clinical presentations vary among different geographical areas because of diversity in culture, lifestyle and dietary habits. Data about this problem is scant from this part of the country.
Here we aimed to analyze the characteristics of FB ingestion in pediatric population presenting to an endoscopy center and their subsequent endoscopic management in a tertiary care hospital setting.
Materials and Methods
This was a prospective observational study carried out in the Department of Gastroenterology at Super specialty hospital which is a tertiary care hospital associated with Government Medical College Srinagar over a period of four years between January 2015 to December 2018. The hospital runs 24 x 7 emergency endoscopy services with round the clock availability of an experienced endoscopy staff.
Study Population
All patients of suspected foreign body were subjected to x-ray neck, chest and abdomen to assess the presence, location, size, configuration, and number of ingested objects. Furthermore, complications such as aspiration, free mediastinal /peritoneal air, or subcutaneous emphysema can be detected. CT scan was done in few selected cases. All the patients were subjected to EGD irrespective of the results of the imaging studies within six hours of presentation. Patients in whom no consent was given for endoscopic procedure were excluded.
All endoscopic procedures were performed by experienced gastroenterologists. Informed consent for endoscopy was obtained by the endoscopy staff before the procedure. EGD was performed per-orally in a standard manner with the patient in the left lateral position. Majority of the procedures were done using intravenous propofol. Endotracheal intubation was done in small number of patients. Intravenous midazolam was used in few cases.
Video endoscope used was GIF Q 150 Olympus optical Co., Ltd., Tokyo, Japan were used. Accessories used for FB retrieval included FB foreceps, Dormia baskets, polypectomy snares, Roth net. Post-procedure patients were kept in recovery ward for observation.
Data extracted from their records included gender, age, indication for the procedure, endoscopic diagnosis and management. Statistical Analysis Collected data was compiled and entered in spread sheet Microsoft excel and exported to Data editor of SPSS computer software, version 20 (SPSS Inc., Chicago, IL, USA). Continuous variables were expressed as mean ± standard deviation and categorical variables were summarized as frequency and percentage.
Results
Age/Sex of Patients
Of the 130 cases with suspected FB ingestion, 88 patients were females (67.7 %). Mean age at diagnosis was approximately 11 years, with a range of 8 months to 18 years.
Type and Location of FB
A total of 130 FBs were diagnosed in 130 cases with suspected FB ingestion. No patient had multiple FBs. FBs were not found in 7 patients (5.4 %) on endoscopy. FB had already passed beyond duodenum. All these patients passed the FB in stool and subsequent X-ray examinations were normal.
The types of FBs were diverse (Table 1): 58.4 % were scarf pins (74 cases), 10.7 % were coins (14 cases), and 9.2 % were knitting needles (12 cases). Button battery was seen in 10 cases (7.7 %). Other FBs included plastic toys, nails. Long sharp metallic FBs were the most common types of FBs.
| Frequency | Percent | |
|---|---|---|
| Nail | 3 | 2.3 |
| Pin scarf | 74 | 58.4 |
| Coin | 14 | 10.7 |
| Needle (knitting) | 12 | 9.2 |
| Screw | 2 | 1.5 |
| Safety pin curved | 3 | 2.3 |
| Bottle cap | 1 | 0.76 |
| Plastic toys | 5 | 3.8 |
| Button battery | 10 | 7.7 |
| Plastic spoon | 1 | 0.76 |
| Pencil battery | 1 | 0.76 |
| Metallic ear ring | 1 | 0.76 |
| Metallic chain (neck) | 1 | 0.76 |
| Plastic brooj | 1 | 0.76 |
| Total | 130 | 100 |
Table 1: Spectrum of FBs found in our study.
Anatomically, FBs were mostly retrieved from stomach (69 %) followed by esophagus 18 (14 %) (Table 2).
| Site of FBs retrieved | Frequency n(%) |
| Cricopharynx | 5 (3.8) |
| Esophagus | 18 (13.8) |
| Stomach | 90 (69.2) |
| Duodenum | 10 (7.7) |
| Normal (no FB seen) | 7 (5.4) |
Table 2: Sites of FB lodgement as on endoscopy.
Clinical Presentation
Majority of the cases presented with just the history of foreign body ingestion. However children with FB impaction in the esophagus presented with irritability and/or refusal to feed. All the cases were accidental in nature.
Outcomes
Out of 130 FBs which were diagnosed in 130 patients on imaging, and endoscopy. 123 FBs could be retrieved successfully endoscopic ally. In 7 patients FBs (7 in number) could not be retrieved either because they had already migrated beyond the reach of upper GI endoscope. All these FBs were ultimately passed with feces uneventfully.
Discussion
Gastrointestinal tract FB ingestion is a common clinical emergency with significant morbidity although low mortality. It can occur at any age, but is more frequent among children aged from six months to four years old [7, 8, 9].
In our study we performed endoscopy in 130 patients in pediatric age group over a period of 4 years who were referred to us with history of foreign body ingestion. The peak prevalence was from age group in the range of 13-18 years old. In related studies, patients involving foreign body ingestion presented with vomiting, drooling, dysphagia, cough, abdominal pain, sensation of something being stuck in the throat, hematemesis, and history of foreign body ingestion [7, 10, 11, 12]. According to the ESPGHAN Guidelines, vomiting and drooling are the predominant symptoms [13].
Majority of cases of FB ingestion in our study were asymptomatic with only history of foreign body ingestion in 102 patients (78.5 %) as majority of them were found in stomach. Only those patients who had FB lodged in esophagus (13.8 %) or cricopharynx (3.8 %) were symptomatic with features of refusal to feed, irritability, foreign body sensation, dysphagia, throat pain, and odynophagia (Table 3&4).
| Design | Present study N =130 Prospective | Khorana J[14] N =194 Thailand Retrospective | W Cheng China [11] N =552 Retrospective | Balekuduru AB[15] India N =120 Retrospective |
|---|---|---|---|---|
| Male: Female (%) | 32:68 | 54:46:00 | 56:44:00 | NA |
| Mean age | 11 years | 43 months | 5.2 years | 8 years |
| (range) years | (8 months -18 years) | NA | (7 months -16 years) | (3 years -18years) |
| Type of FB | Scarf pin 58% | Coin 41% | Coin 49 % | Coin 69 % |
| (MC) | Coin 11% | Food bolus 15% | Fish bone 29 % | Batteries 11% |
| Knitting needle 9% | Button battery 11 % | Metallic objects 13% | Pins 4% | |
| Site of FB | MC:Stomach 69 % | Esophagus 37% | Esophagus : MC | Esophagus 70 % Stomach 16 % |
| Esophagus 14 % | Stomach 29 % |
Table 3: Comparing the results of our study with some other studies. MC: most common; NA: not available.
| Site | When to remove | |
|---|---|---|
| Battery/Sharp pointed/Food bolus with obstruction | Esophagus | Emergently |
| Magnet/Blunt object upto 5 cms | Esophagus | Urgently |
| Battery/Sharp pointed/Magnet/Blunt more than 5 cms size | Stomach/small bowel | Urgently |
| Blunt object upto 5 cms | Stomach/small bowel | Non-urgent |
Table 4: Battery/Sharp pointed.
Table 4: Battery/Sharp pointed.
The most common FB in this study was pins and needles (67.6%) followed by coins (10.7%) which is an uncommon finding in other studies [16, 17]. The type of FB ingested depends on easily available and frequently used objects, that is why toothbrushes, dentures, nails, coins, and toys are the most common FBs found worldwide. The type of FB also varies from country to country [18, 19, 20, 21].The pattern must also be changing from time to time as the readily available things also change from time to time and from place to place. The reason that the pins and needles were common FBs, in our study especially in young girls is clear from the fact that these things are being routinely used by our young girls for tying their head covers and for chain stitching jobs. The above facts can be explained to the basis of the type of the most common FB found in our study that is scarf pin which reflects our religio-cultural setup to wear head cover known locally as scarf. Each scarf remains attached to hair of these young females by many pins. While tying the head cover, these young girls keep many pins under their teeth and if something untoward happens during this time such as sneezing, coughing, someone else pushing from behind or frightening you, there is every chance that these pins may either be swallowed or aspirated. As these pins are commonly used in household in our part of world there is every chance that even young kids finding misplaced pins and while playing with these pins may accidentally swallow them which was the case with our most young cases.
Our study has shown the impact of local prevalent culture on the spectrum of the type of FBs. Similar observation about the local cultural impact was observed by a South China [22] study in which bone ingestion (fish and chicken) constituted almost 75% of the total FBs which was explained by the local culture of using sea food very commonly (Figure 1(A-G)).
Regarding the location of foreign body, at initial presentation, approximately 5% to 10% of patients will have the foreign body lodged in the oropharynx, 20% of foreign bodies will be located in the esophagus, 60% will be located in the stomach and 10% will be located distal to the stomach, usually in the small intestine [23]. In our study also we found most of foreign bodies in stomach (69%) followed by esophagus (13.8%). Location of foreign bodies depends on many factors most important ones are timing of presentation, nature and size of foreign body. Determining or suspecting the location of foreign body is important before planning and deciding about management protocol including endoscopic retrieval. Location of foreign body can be suspected by clinical symptoms and appropriate radiographs before planning endoscopic retrieval. Between60% and 90% of ingested foreign bodies are found to be radiopaque [4, 24].
So location of most of the foreign bodies can be determined on properly taken X ray films before planning a management protocol.
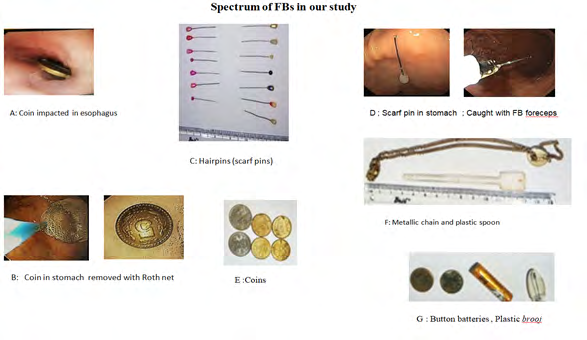
Figures 1(A-G): Spectrum of FBs presenting to our centre.
Various Management guidelines have been put forward for the management of GI foreign bodies. But the pattern and management of FB ingestion varies with the geography of the area, local culture and the facilities at a particular center which vary as per the infrastructure, equipment, manpower and availability of round the clock emergency services. Timing of endoscopic management mainly depends on site and nature of foreign body.
Timing of endoscopic intervention in Table 5 foreign body ingestions as per has been defined by European society of gastrointestinal endoscopy (ESGE) [25] as: Emergent is preferably within 2 hours, but at latest within 6 hours; Urgent, within24 hours; Non-urgent, within 72 hours.
| Frequency | Percent | |
|---|---|---|
| Retrieved | 123 | 94.6 |
| Not Retrieved | 7 | 5.4 |
| Total | 130 | 100 |
Table 5: Result of endoscopic intervention in FB ingestion.
NASPGHAN recommends all FBs in Upper GI tract to be removed either emergently or urgently especially if patient is symptomatic. Elective endoscopic removal for asymptomatic coins and button batteries in stomach. Sharp and long objects should be removed urgently even if asymptomatic.
Three guidelines [8, 13, 26] h regarding foreign bodies in the stomach and duodenum mentioned the size of the object. Any object larger than 2.5 cm in diameter or 6 cm long were removed in every case. On the other hand, the Colorado guidelines defined the need for removal of a long object by a sliding scale of length against age. For a child younger than one year old, an object needing removal is larger than 2 cm in diameter or longer than 3 cm. From one year old and older, the guideline is between 3 and 5 cm. This guideline is also recommended to remove all long objects before the duodenum [12]. We recommend removing a foreign body wider than 2.5 cm and longer than 5 cm in all age groups. The reasoning behind this is that the large object may not pass the pyloric canal and the long object may become stuck in the duodenal sweep. Endoscopic removal of button batteries is recommended in every case due to the uncertainty of the quality of battery. Many guidelines recommend observation by repeated films, with timing to repeat a film dependent on the size and age of the child. All foreign bodies beyond the stomach and duodenum, including the jejunum, ileum, and colon, passed spontaneously in our study.
We believe that the traditional concept that 80-90% of the ingested foreign bodies need not to undergo endoscopic removal needs to be adjusted, as per the spectrum of FBs in a particular geographical region. The most common foreign bodies in our study were long sharp pointed metallic objects like scarf pin and knitting needle. We performed endoscopic management in all the patients with excellent results. Similar spectrum of long sharp FBs was observed in a South China study [22] which had fish bone as most common type of foreign body. These FBs even if asymptomatic can have potentially dangerous complications. In addition other studies, including those from 2 groups in Korea and Italy, reported that higher percentages of patients with foreign bodies were treated endoscopically [27, 28]. Besides our centre has 24x7availability of experienced endoscopy staff available, and the foreign bodies were always extracted oncethey are observed by endoscopists.
Conclusion
We have presented our data about GI tract foreign bodies which has a very unusual spectrum with predominantly long thin sharp objects scarf pin and knitting needle. Majority of them were lodged in the stomach. We have found endoscopy a safe and highly efficacious management modality for these upper gi tract FBs. We recommend early UGI endoscopy in managing these patients.
Acknowledgement
The authors are indebted to the patients and their gusrdians, anaesthesia team gastrointestinal endoscopy staff for all the support.
Conflicts of Interest
All the authors declare that they have no conflict of interest relevant to this article.
References
-
Pfau P (2005) Ingested foreign objects and food bolus impactions. In: Ginsberg GG, Kochman ML, Norton I, et al., (Eds.), Clinical Gastrointestinal Endoscopy, Saunders: Elsevier, pp: 291-304.
-
Hachimi Idrissi S, Corne L, Vandenplas Y (1998) Management of ingested foreign bodies in childhood: our experience and review of the literature. Eur J Emerg Med 5(3): 319-323.
-
Litovitz TL, Klein-Schwartz W, White S, Daniel JC, Youniss J, et al. (2000) annual report of the American Association of Poison Control Centers Toxic Exposure Surveillance System. Am J Emerg Med 19(5): 337-395.
-
Macpherson RI, Hill JG, Othersen HB, Tagge EP, Smith CD, et al. (1996) Esophageal foreign bodies in children: diagnosis, treatment, and complications. AJR Am J Roentgenol 166: 919-924.
-
Waltzman ML, Baskin M, Whpij D (2005) A randomized clinical trial of the management of esophageal coins in children. Pediatrics 116: 614-620.
-
Eisen GM, Baron TH, Dominitz JA, Douglas OF, Jay LG, et al. (2002) Guideline for the management of ingested foreign bodies. Gastrointest Endosc 55: 802-806.
-
Dereci S, Koca T, Serdaroglu F, Akcam M (2015) Foreign body ingestion in children. Turk PediatriArs 50(4): 234- 240.
-
Kramer RE, Lerner DG, Lin T, Manfredi M, Shah M, et al. (2015) Management of ingested foreign bodies in children: A clinical report of the NASPGHAN Endoscopy Committee. J Pediatric Gastroenterol Nutr 60(4): 562- 574.
-
The Royal Children’s Hospital Melbourne (2018) Foreign Body Ingestion.
-
Patmika Jiaravuthisan SC, Niramis R (2010) How to Manage Foreign Bodies in the Alimentary Tract? Thai Pediatric J 17: 16-25.
-
Cheng W, Tam P (1999) Foreign-body ingestion in children: Experience with 1,265 cases. J Pediatr Surg 34(10): 1472-1476.
-
Uyemura MC (2005) Foreign body ingestion in children. Am Fam Physician 72(2): 287-291.
-
Thomson M, Tringali A, Dumonceau JM, Tavares M, Tabbers MM, et al. (2017) Paediatric Gastrointestinal Endoscopy: European Society for Paediatric Gastroenterology Hepatology and Nutrition and European Society of Gastrointestinal Endoscopy Guidelines. J Pediatric Gastroenterol Nutr 64(1): 133- 153.
-
Jiraporn K, Tantivit Y, Phiuphong C, Pattapong S, Siripan S (2019) Foreign Body Ingestion in Pediatrics: Distribution, Management and Complications. Medicina 55(10): 686.
-
Balekuduru AB, Shetty B, Dutta A, Subbaraj SB (2017) Profile of foreign body ingestion and outcomes of endoscopic management in pediatric population. J Dig Endosc 8(1): 17-23.
-
Li ZS, Sun ZX, Zou DW, Xu GM, Wu RP, et al. (2006) Endoscopic management of foreign bodies in the upper GI tract: Experience with 1088 cases in China. Gastrointest Endosc 64(4): 48592.
-
Sahn B, Mamula P, Ford CA (2014) Review of foreign body ingestion and esophageal food impaction management in adolescents. J Adolesc Health 55(2):260266.
-
Proctor MH (19687) Assault by battery. N Engl J Med 316: 554.
-
Sugawa C, Ono H, Taleb M, Lucas CE (2014) Endoscopic management of foreign bodies in the upper gastrointestinal tract: A review World J Gastrointest Endosc 6(10): 475481.
-
Ambe P, Weber SA, Schauer M, Knoefel WT (2012) Swallowed foreign bodies in adults. Dtsch ArzteblInt 109(50): 869875.
-
Emara MH, Darwiesh EM, Refaey MM, Galal SM (2014) Endoscopic removal of foreign bodies from the upper gastrointestinal tract: 5year experience. Clin Exp Gastroenterol 7: 249253.
-
Shenghong Zhang (2010) Endoscopic Management of Foreign Bodies in the Upper Gastrointestinal Tract in South China: A Retrospective Study of 561Cases. Dig Dis Sci 55(5): 1305-1312.
-
Kay M, Wyllie R (2017) Foreign bodies and caustic ingestions in infants and children. In: Sabella C, Cunningham R, (Eds.), The Cleveland Clinic Intensive Review of Pediatrics, 4th (Edn.), Wolters Kluwer, Lippincott, Williams & Wilkins, Philadelphia.
-
Lemberg PS, Darrow DH, Holinger LD (1996) Aerodigestive tract foreign bodies in theolder child and adolescent. Ann Otol Rhinol Laryngol 105(4): 267-271.
-
Michael B, Peter B, Pierre HD, Michael H, Dirk H, et al. (2016) Removal of foreign bodies in the upper gastrointestinal tract in adults: (ESGE) Clinical Guideline. Endoscopy 48: 1-8.
-
Ikenberry SO, Jue TL, Anderson MA, Appalaneni V, Banerjee S, et al. (2011) Management of ingested foreign bodies and food impactions. Gastrointest. Endosc 73(6): 1085-1091.
-
Mosca S, Manes G, Martino R, Amitrano L, Bottino V, et al. (2001) Endoscopic Management of Foreign Bodies in the UpperGastrointestinal Tract: Report on a series of 414 adult patients. Endoscopy 33(8): 692-696.
-
Kim JK, Kim SS, Kim JI, Kim SW, Yanget YS, et al. (1999) Management of foreign bodies in the gastrointestinal tract: an analysis of 104 cases in children. Endoscopy 31(4): 302-304.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient