COVID-19 Male Patients with Gastrointestinal Symptoms are at Higher Risk of Poor Clinical Outcomes but Not Mortality in Low Prevalence Areas
COVID-19 has been reported to cause gastrointestinal (GI) manifestations. However, there is limited data regarding the association between GI symptoms and clinical outcomes including mortality in low population density. Using TriNetX, a real-time analysis was performed for patients diagnosed with COVID-19 at Penn State Milton S. Hershey Medical Center. Our study, including a cohort of male and female patients (220), showed that the Covid-19 male patients with GI symptoms have higher risk for respiratory failure and hospitalization, but not mortality, compared to male patients without GI symptoms or female patients (with or without GI symptoms). Our study provides unique perspective of the impact of Covid-19-related mortality in low-density areas independent of GI symptoms.
Introduction
Coronavirus infection (COVID-19), caused by SARS- CoV-2, was declared a global pandemic in early 2020. Although primarily a respiratory illness, gastrointestinal intestinal symptoms also appear to play a prominent role in disease pathogenesis [1, 2, 3]. COVID-19 causes a wide range of clinical symptoms, ranging from mild to critical illness, hospitalizations, death by sepsis and acute respiratory distress syndrome (ARDS) [4]. Clinical features of multiple organ failure occur sequentially or together, suggesting that they result from a final common pathway [5, 6]. Our aim in this study was to determine the association between GI symptoms and several clinical outcomes in a cohort of COVID-19 patients at Penn State Milton S. Hershey Medical Center, an academic teaching hospital in the United States located in Dauphin County PA, a region with low local prevalence of COVID-19 infection.
Methods
Using TriNetX (Cambridge, MA, USA), a real-time search and analysis was performed for 220 patients (≥18 year’s age) diagnosed with COVID-19 at Penn State Health. TriNetX (Cambridge, MA, USA), is a global federated health research network providing access to electronic medical records (diagnoses, procedures, medications, laboratory values, genomic information). The TriNetX platform uses aggregated counts and statistical summaries of de-identified patient information. No protected health information (PHI) or personal data is made available to the users of the platform. TriNetX de-identifies and protects patient counts to safeguard protected health information by rounding patient counts in analyses up to the nearest 10.
Patients were stratified into two groups based upon the presence or absence of GI symptoms (diarrhea, infectious gastroenteritis and colitis, vomiting and nausea). Outcomes studied were respiratory failure, hospitalization and mortality, occurring within the 2 weeks after COVID-19 diagnosis.
Description of the Data Source
TriNetX (Cambridge, MA, USA) Penn State HCO Network incorporates COVID-19 specific diagnosis and terminology following the World Health Organization (WHO) and Centers for Disease Control (CDC) COVID-19 criteria. TriNetX uses de-identified clinical data along with the analytics to analyze research questions and aggregates them directly from the electronic medical records of the participating HCO.
Selection of COVID-19 Patients
TriNetX identified potential COVID-19 patients on or after January 20th through May 17th 2020, as per the CDC COVID-19 coding guidelines. These codes included Clinical Modification (ICD-10-CM) codes U07.1 (COVID-19, virus identified), U07.2 (COVID-19, virus not identified 9 WHO), B34.2 (Coronavirus infection, unspecified), B97.29 (Other coronavirus as the cause of diseases classified elsewhere) and J12.81 (Pneumonia due to SARS-2 associated coronavirus). Patients identified with diagnosis code 079.89 (Other specified viral infection) were excluded.
Selection of Patients with GI Symptoms Associated with Clinical Outcomes
Queries for patients who presented with GI symptoms were made using the ICD-10-CM codes R11.0 (nausea), R11.1 (vomiting), R11.2 (nausea and vomiting, unspecified), R19.7 (diarrhea, unspecified), K59.1 (functional diarrheas) and A09 (infectious gastroenteritis and colitis).
Study Outcomes
The time window to estimate all outcomes was up to 14 days from the day of COVID-19 diagnosis. The outcomes examined were the risk of respiratory failure, hospitalization and mortality. Respiratory failure was defined by the following ICD 10 codes: J80 (acute respiratory distress syndrome), J96.0 (acute respiratory failure), J96.1 (chronic respiratory failure), J96.2 (acute and chronic respiratory failure), J18.9 (pneumonia unspecified organism), R06.03 (acute respiratory distress), R06.00 (dyspnea, unspecified), and R06.02 (shortness of breath). Hospitalization was categorized by visit type within TriNetX and included CPT codes 1013659 (hospital inpatient services), 1013729 (clinical care services) and 1013699 (initial inpatient consultation services).
Statistical Analysis
All statistical analyses were performed in real-time using TriNetX. The means and standard deviations were used to describe and compare patient characteristics. Measures of association were computed to determine the risk of experiencing each outcome between the two study cohorts (presence or absence of GI symptoms). The risk difference computed the difference in risk between cohorts (Risk Ratio = Risk for Cohort 1 / Risk for Cohort 2, +/- 95% CI). Kaplan Meier analysis was performed to assess the probability of each study cohort surviving each study outcome.
Results
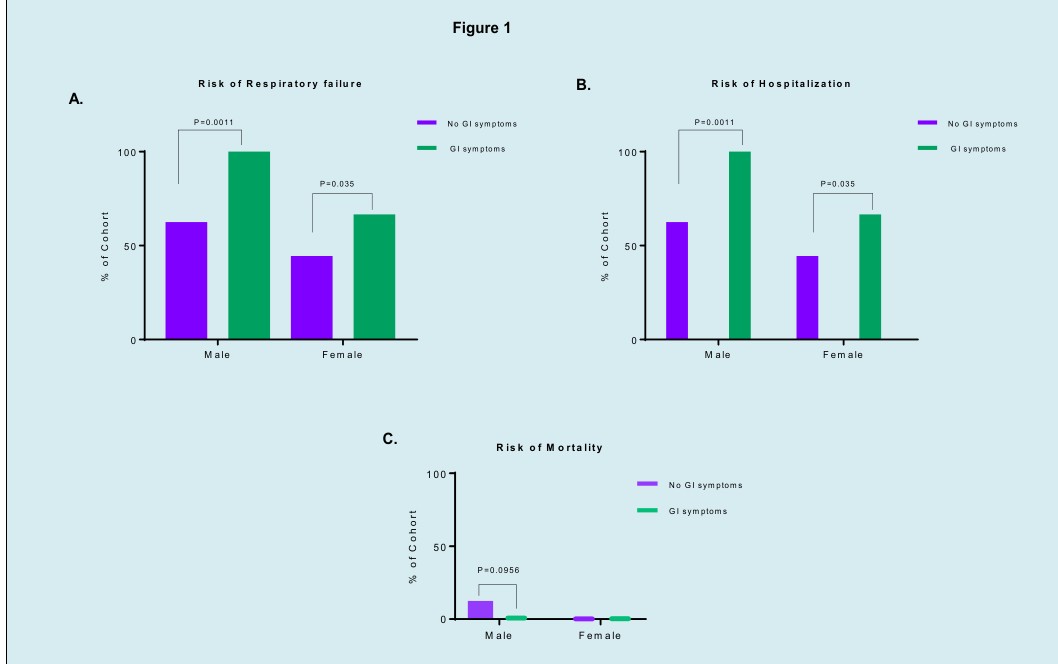
Association analysis was performed to assess differences in outcome between COVID-19 patients with and without GI symptoms. Data from 220 COVID-19 patients (ages 18 and older) (100 males and 120 females) was evaluated (Table 1). 22.7% (50) of cases exhibited GI symptoms (20 males and 30 females), including diarrhea, vomiting and nausea within the 2 weeks before or after COVID-19 diagnosis. Respiratory failure was present in 60% of patients with GI symptoms compared to 52.9% of patients with no GI symptoms (RR 0.882, 95% CI 0.676-1.152, p-value 0.378). A need for hospitalization was present in 60% of patients with GI symptoms compared to 47% of patients without GI symptoms (RR 0.784, 95% CI 0.595-1.034, p-value 0.107). Subgroup analysis based upon gender in each patient cohort (GI vs. no GI symptoms) demonstrated gender- based outcomes differences (Table 2). GI symptoms were more prevalent among female patients (25% vs. 20%). The presence of respiratory failure and need for hospitalization was present in 100% of males with GI symptoms vs. 62.5% without GI symptoms (RR 0.625, 95% CI 0.527-0.741, p-value 0.0011) and in 66.6% of females with GI symptoms vs. 44% without GI symptoms (RR 0.667, 95% CI 0.473-0.939, p-value 0.0350) (Figure 1A & B). Interestingly, mortality risk was greater among males without GI symptoms, 12.5% vs. 0% in males and females respectively (Figure 1C). This finding may be due to the larger number of older male patients in the cohort without GI symptoms (> 75 years old, n=16) compared to male patients in the cohort of GI symptoms (> 75 years old, n=3) (Figure 1).
| Covid-19 with no GI symptoms | Covid-19 with GI symptoms | ||||
|---|---|---|---|---|---|
| NO GI symptoms | With GI symptoms | Measure of Association | |||
| Male | Female | Male | Female | ||
| No. of patients (n or %) | 80/170 (47%) | 90/170 (53%) | 20/50 (40%) | 30/50 (60%) | |
| Mean age | 57.1±19.1 | 55.3±13.7 | 47.9±20.3 | 51.9±19.9 | |
| Race* (%) | |||||
| White | 62% | 66% | 50% | 66% | |
| African American black | 12% | 11% | 50% | 33% | |
| Asian | 12% | 11% | 50% | 33% | |
| Unknown | 25% | 22% | 50% | 33% | |
| Others | 12% | 11% | 0% | 33% | |
| OUTCOMES | Patients with outcomes | Patients with outcomes | Risk Ratio (95% confidence inter- val) | Risk difference (95% confidence interval) | P-Value |
| Males | |||||
| Respiratory Failure | 50/80 (62.5%) | 20/20 (100%) | 0.625 (0.527, 0.741) | -37.5% (-48.109, -26.89%) | 0.0011 |
| Hospitalization | 50/80 (62.5%) | 20/20 (100%) | 0.625 (0.527, 0.741) | -37.5% (-48.109, -26.89%) | 0.0011 |
| Mortality | 10/80 (12.5%) | 0/20 (0%) | 0 | 12.50% | 0.0956 |
| Females | |||||
| Respiratory Failure | 40/90 (44.44%) | 20/30 (66.667%) | 0.667 (0.473,0.939) | -22.22% (-41.97, -2.475%) | 0.035 |
| Hospitalization | 40/90 (44.44%) | 20/30 (66.667%) | 0.667 (0.473,0.939) | -22.22% (-41.97, -2.475%) | 0.035 |
| Mortality | 0/90 (0%) | 0/30 (0%) | 0 | 0% | 0 |
Table 1: Comparison of patient Demographics among COVID-19 male and female patients. *TriNetX platform rounds patient counts in a
Discussion
GI symptoms are common in patients with COVID-19 as reported previously [7, 8]. Our study aimed to characterize the clinical outcomes of COVID-19 patients with GI symptoms and evaluated differences in chosen outcomes between male and female patients. Although the prevalence of females with GI symptoms (25%) in our study was higher than males (20%), males showed a higher risk of poor clinical outcomes, including respiratory failure and hospitalization. We postulate that the gender-related difference in GI symptoms can be explained on the basis of behavioral, hormonal or immunological factors. However, the exact reason for the difference remains elusive. The relative risk of adverse outcomes was markedly higher in male patients than female patients, consistent with recent published reports [9, 10]. Respiratory failure and hospitalization were seen in the vast majority of male patients with GI symptoms as compared to male patients without GI symptoms (RR 0.625, 95% CI 0.527-0.741, p-value-0.0011), suggestive of the presence of SARS-CoV-2 in intestinal tissues. This may be due to the high expression of angiotensin converting enzyme-2 (ACE- 2) receptor in intestinal epithelial cells, as well as in the lung tissues, which has been reported to be the main host cell receptor of SARS-CoV-2 [11, 12]. Additionally, mounting of the Th2 immune responses by SARS-CoV-2 may also contribute to GI symptoms, as has been recently suggested [13]. Gastrointestinal symptoms in COVID-19 patients are significantly associated with dyspnea, which is linked to a Th2 response [13, 14]. Moreover, the GI common symptoms may be an indication of defective intestinal barrier, which leads to bacterial translocation and exacerbating systemic infection and inflammation.
The relatively low local mortality rate of COVID-19 patients independent of GI symptoms and gender is difficult to explain. We postulate that the low local prevalence rates and perhaps easier access to hospitalization and intensive care support may have resulted in patients seen earlier in the course of disease. In addition, a unique contact tracing program utilizing Penn State Hershey Medical Students under faculty supervision and supported by a dedicated COVID-19 clinic was implemented.
Conclusion
Our study is limited by the smaller sample size, is from a single center and results may not be generalizable. However, it provides the unique perspective of the impact of disease related factors in a low prevalence area with low population density. Further, multi-institutional larger studies are needed to validate these findings.
Acknowledgments
We acknowledge Penn State Health System and National Center for Advancing Translational Sciences, National Institutes of Health, through Grant UL1 TR002014 to provide us access, and training to the TriNetX global healthcare network. We also acknowledge the TriNetX (Cambridge, MA, USA) healthcare network for design assistance to complete this project.
Disclosure
Shannon Dalessio, Steven King, Iryna Pinchuk and Rana
Al-Sadi declare that they have no conflict of interest.
Kofi Clarke has the following disclosures; TAKEDA- Speaker’s Bureau for Non Branded Presentations, JANSSEN- Speaker’s Bureau for Non Branded Presentations ABB Vie- Speaker’s Bureau for Non Branded Presentations, PFIZER- Grant Reviewer, and Speaker’s Bureau for Non Branded Presentations
References
-
Pan L, Mu M, Yang P, Sun Y, Runsheng W, et al. (2020) Clinical Characteristics of COVID-19 Patients With Digestive Symptoms in Hubei, China: A Descriptive, Cross-Sectional, Multicenter Study. Am J Gastroenterol 115(5): 766-773.
-
Han C, Duan C, Zhang S, Brennan S, Huiying S, et al. (2020) Digestive Symptoms in COVID-19 Patients With Mild Disease Severity: Clinical Presentation, Stool Viral RNA Testing, and Outcomes. Am J Gastroenterol 115(6): 916-923.
-
Mao R, Qiu Y, He JS, Jin-Yu T, Xue-Hua L, et al. (2020) Manifestations and prognosis of gastrointestinal and liver involvement in patients with COVID-19: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol 5(7): 667-678.
-
Zhou F, Yu T, Du R, Guohui F, Ying L, et al. (2020) Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet 395(10229): 1054-1062.
-
Tay MZ, Poh CM, Renia L, MacAry PA, Lisa FP Ng, et al. (2020) The trinity of COVID-19: immunity, inflammation and intervention. Nat Rev Immunol 20(6): 363-374.
-
Du Y, Tu L, Zhu P, Pingjun Z, Mi M, Runsheng W, et al. (2020) Clinical Features of 85 Fatal Cases of COVID-19 from Wuhan. A Retrospective Observational Study. Am J Respir Crit Care Med 201(11): 1372-1329.
-
Zhou Z, Zhao N, Shu Y, Shengbo H, Bin C, et al. (2020) Effect of Gastrointestinal Symptoms in Patients With COVID-19. Gastroenterology 158(8): 2294-2297.
-
Cheung KS, Hung IFN, Chan PPY, Lung KC, Eugene T, et al. (2020) Gastrointestinal Manifestations of SARS-CoV-2 Infection and Virus Load in Fecal Samples From a Hong Kong Cohort: Systematic Review and Meta-analysis. Gastroenterology 159(1): 81-95.
-
Wong SH, Lui RN, Sung JJ (2020) Covid-19 and the digestive system. J Gastroenterol Hepatol 35(5): 744- 748.
-
Luo S, Zhang X, and Xu H (2020) Don’t Overlook Digestive Symptoms in Patients With 2019 Novel Coronavirus Disease (COVID-19). Clin Gastroenterol Hepatol 18(7): 1636-1637.
-
Ziegler CGK, Allon SJ, Nyquist SK, Ian MM, Vincent NM, et al. (2020) SARS-CoV-2 Receptor ACE2 Is an Interferon- Stimulated Gene in Human Airway Epithelial Cells and Is Detected in Specific Cell Subsets across Tissues. Cell 181(5): 1016e19-1035e19.
-
Lamers MM, Beumer J, van der Vaart J, Kèvin K , Jens P, et al. (2020) SARS-CoV-2 productively infects human gut enterocytes. Science.
-
Roncati L, Nasillo V, Lusenti B, Giovanni R (2020) Signals of Th2 immune response from COVID-19 patients requiring intensive care. Ann Hematol 99(6): 1419- 1420.
-
Chen N, Zhou M, Dong X, Jieming Q, Fengyun G, et al. (2020) Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet 395(10223): 507-513.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient