First Known Case of Follicular Pancreatitis Mimicking a Mucinous Cystic Neoplasm and Review of Literature
Follicular pancreatitis is a newly described entity of chronic pancreatitis that has never been described in the literature as presenting as a cystic mass. All cases to date have described a solid mass, which is easily confused radiologically for pancreatic adenocarcinoma. We report a case of follicular pancreatitis that presented as an enlarging cystic mass concerning for mucinous cystic neoplasm in a patient undergoing an abdominal pain workup. The patient subsequently underwent distal pancreatectomy, which grossly showed a unilocular cystic mass. Histologic findings, however, were consistent with follicular pancreatitis.
Introduction
Follicular pancreatitis is a rare, fairly new classification of chronic pancreatitis that was once considered to be a variant of autoimmune pancreatitis. Previously called “pseudolymphoma,” this entity is characterized by prominent lymphoid follicles with reactive germinal centers, which was originally described in 2012 by Zen et al. [1], Gupta RK, et al. [2], Hatzitheoklitos E, et al. [3] and can also be seen in the liver [4]. With only a handful of cases having been previously reported, it still remains a newer entity that is not fully understood. All cases to date have been characterized clinically by a discrete pancreatic mass on imaging [2]. Immunohistochemical staining shows Bcl-2-negative germinal centers within a CD21-positive intact dendritic cell network [5]. Herein, we report the first case of follicular pancreatitis presenting as an enlarging cystic mass of the pancreatic tail, consistent with a clinical picture of mucinous cystic neoplasm.
A 69 year old Caucasian female with no prior history presented from an outside hospital with complications from routine colonoscopy. CT scan performed prior to emergent splenectomy showed an incidental cyst in the pancreatic tail, which did not communicate with the main pancreatic duct (Figure 1). Initial endoscopic ultrasound (EUS) of cystic lesion showed an anechoic cystic mass in the pancreatic tail measuring 26.4 mm x 24.1 mm that did not communicate with the pancreatic duct. No tissue samples were taken; however, 10 mL of clear, watery fluid was aspirated, which demonstrated an amylase level of 40 U/L, and a carcinoembryonic antigen (CEA) level of 67.8 ng/mL.
Repeat CT scan the following year showed enlargement of the cyst, now measuring 3.0 x 2.8 cm. Repeat EUS demonstrated similar findings and cyst fluid was aspirated, which now showed decreased amylase levels to 4 U/L and increased CEA levels to 517 ng/mL. The lesion was suspicious for a mucinous cystic neoplasm, and the patient subsequently underwent distal pancreatectomy.

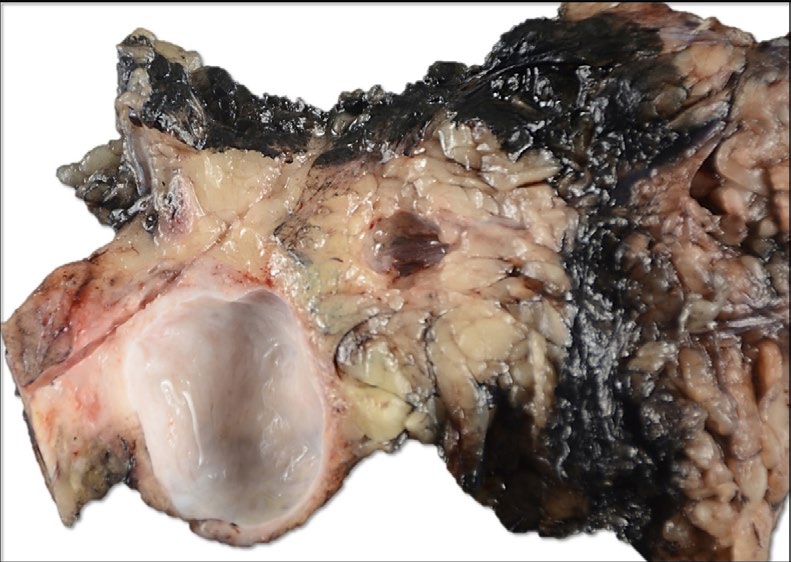
Sectioning through the pancreas demonstrated a 3.0 cm unilocular cystic mass filled with clear, watery fluid and a smooth inner surface (Figure 2), which did not communicate with the main pancreatic duct. The surrounding pancreatic tissue was unremarkable with no additional focal lesions. Figure 2: Gross photograph of distal pancreatectomy. The specimen is bilvalved to reveal a 2.6 cm unilocular cystic mass, which does not communicate with the main pancreatic duct. No discrete masses are seen adjacent to the cyst.
Microscopically, the entirely submitted cyst was lined by a simple cuboidal biliary type epithelium, most consistent with dilated retention cyst. The background pancreas showed a distinct histomorphologic variant of chronic pancreatitis that was characterized by a chronic inflammatory infiltrate and marked follicular type lymphoid hyperplasia with prominent germinal centers. The cyst lining was comprised of simple cuboidal epithelium consistent with biliary type. No storiform fibrosis, obliterative phlebitis, nor granulocytic/ neutrophilic epithelial lesions was noted (Figure 3).
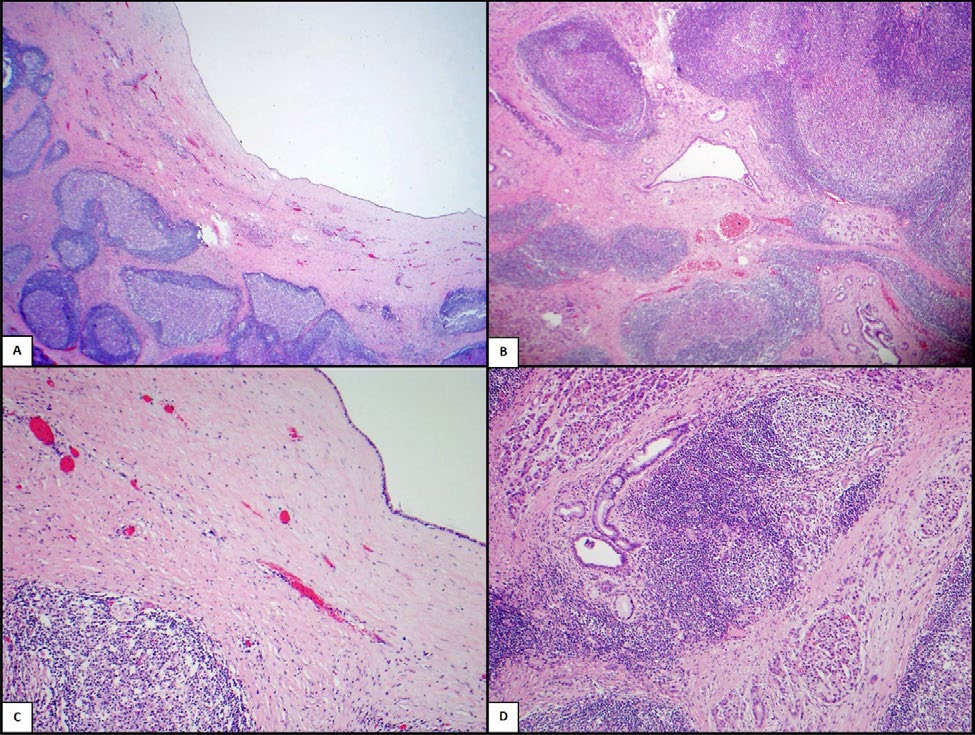
Figure 3: Low power view shows part of the cyst with surrounding lymphoid follicles (A). The reactive lymphoid follicles are located around both ducts and acini. No storiform fibrosis, obliterative phlebitis nor neutrophilic abscesses are seen (B&D). The cyst is lined by simple biliary type epithelium without atypia. No surrounding ovarian-type stroma is seen (C).
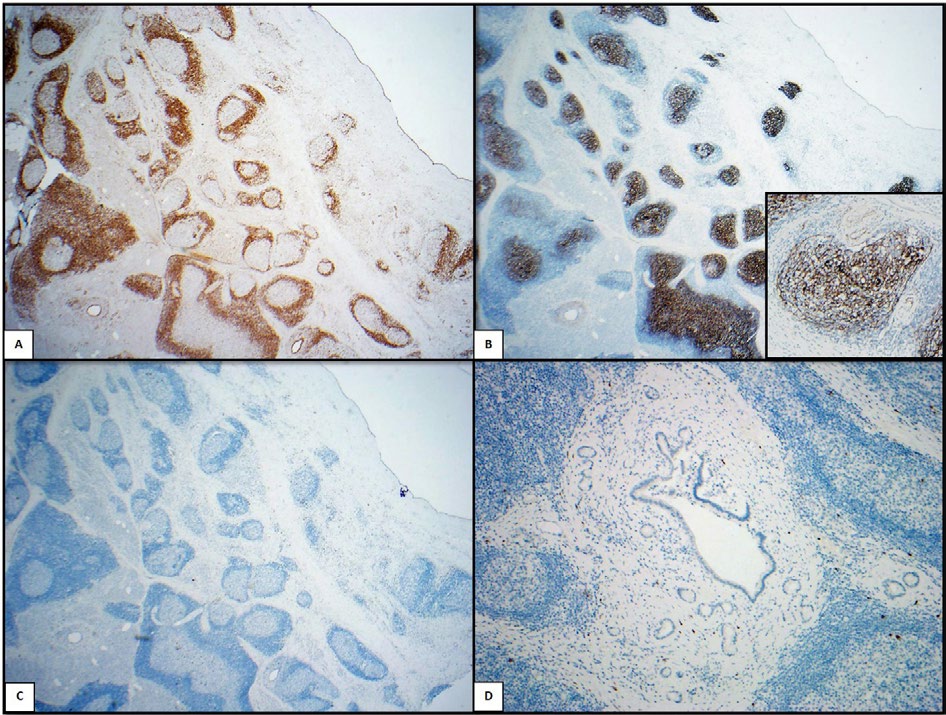
Immunohistochemical staining showed Bcl-2-negative germinal centers. CD21 showed an intact follicular dendritic network within the germinal centers. IgG4 showed very low positivity (Figure 4).
Discussion
Follicular pancreatitis is a newly described variant of chronic pancreatitis, which has been previously described radiologically as a solid mass on CT. Our case is unique in its presentation of a cystic lesion in the tail of the pancreas. To date, this is the only case that has been reported presenting as a cystic lesion located in the pancreatic tail (Figure 1 & 2), and not as a solid mass. Additionally, our mass was located in the tail of the pancreas and not in the head or body, which is the location of all other cases that have been described. Our case is also unique in the fact that cystic fluid aspiration at the time of EUS showed findings consistent with a mucinous cystic neoplasm, which further complicated diagnosis. In hindsight, a diagnosis of follicular pancreatitis may have been able to be made had there been actual tissue taken during the time of EUS, instead of relying solely on fluid aspiration for proper diagnosis. However, the study performed by Gupta et al described cytologic FNA findings that were nonspecific and consisted of scant pancreatic epithelial cells with mild atypia, lymphocytes, and neutrophils with no overt malignant features seen. Current guidelines for biopsy of cystic lesions on EUS are somewhat unclear with no clear consensus. However, recent data has suggested that performing both cyst fluid analyses combined with FNA biopsy may prove to be the best combination to help diagnose cystic lesions of the pancreas [6].
Microscopically our case was similar to previously described cases of follicular pancreatitis, which included the classic morphology of lymphoplasmacytic infiltrate comprised of multiple lymphoid follicles with prominent germinal centers. Additionally, these follicles were found around both ducts and acini (Figure 3). This is different from type 1 autoimmune pancreatitis, which has three main criteria for diagnosis including storiform fibrosis, a lymphoplasmacytic infiltrate, and obliterative phlebitis. In order to diagnose type 1 autoimmune pancreatitis, two of these three criteria must be met [5]. Additionally, our case did not represent type 2 autoimmune pancreatitis due to the lack of neutrophilic epithelial lesion duct change, a hallmark feature seen in type 2 autoimmune pancreatitis [7] (Table 1). Finally, the cyst did not have features of a mucinous cystic neoplasm, which include a columnar, mucin producing epithelium with varying degrees of atypia, and most importantly, no ovarian type stroma, which is essential for diagnosis [5].
| Autoimmune Pancreatitis Type 1 | Autoimmune Pancreatitis Type 2 | Follicular Pancreatitis | |
|---|---|---|---|
| (Lymphoplasmacytic Sclerosing Pancreatitis) | (Idiopathic Duct-Centric Pancreatitis) | ||
| Storiform Fibrosis | Present | Absent | Absent |
| Obliterative Phelebitis | Present | Absent | Rare |
| Lymphoid Follicles with Germinal Centers | Rare, in lobules | Absent | Prominent, mainly periductal |
| Serum IgG4 levels | High | Low (Only 7% shows elevation of serum IgG4 level but less than 2 times the upper limit of normal) | Low |
| Tissue IgG4:IgG levels | High (IgG4+/IgG+ cells > 40% and >10 IgG4+ plasma cells/HPF)* | Low (Few scattered cells) | Low (Few scattered cells) |
| Granulocytic Epithelial Lesions | Absent | Present | Absent |
| Systemic versus Pancreas limited disease | Systemic | Pancreas | Pancreas |
Table 1: Comparison between autoimmune pancreatitis and follicular pancreatitis.
Immunohistochemical staining was also consistent with previously described follicular pancreatitis. While type 1 autoimmune pancreatitis demonstrates an elevated IgG4- to-IgG ratio, our case showed a low number of IgG4 plasma cells, thus maintaining a low IgG4-to-IgG ratio. Bcl-2 negative germinal centers with CD21-positive intact follicular dendritic networks [1] (Figure 4).
Because of the complex nature of hepatobiliary surgeries coupled with the high risk of subsequent complications, it is important to be aware of this entity to manage these patients in a conservative manner [8, 9]. Because there has been no evidence in literature of a malignant transformation of follicular pancreatitis, surgery is likely not necessary. Although rare, it is important to recognize this presentation as a potential diagnostic pitfall. This is crucial in order to properly manage and treat this entity conservatively and avoid surgical intervention and ultimately, the possibility of adverse complications that parallel such extreme surgical modalities.
Conclusion
Follicular pancreatitis is an exceedingly rare variant of chronic pancreatitis with only a handful of confirmed cases reported in the literature [2]. We report the first case of follicular pancreatitis presenting as a cystic mass as opposed to a solid mass and which was also located in the pancreatic tail. This lesion presented with preoperative imaging and cyst fluid analysis concerning for mucinous cystic neoplasm. However, histologically our diagnosis confirmed the benign entity of follicular pancreatitis, which was supported by overall morphology and immunohistochemical staining.
Conflicts of Interest
Authors declare no conflicts of interest
References
-
Zen Y, Ishikawa A, Ogiso S, Heaton N, Portmann B (2012) Follicular cholangitis and pancreatitis - clinicopathological features and differential diagnosis of an under-recognized entity: Follicular pancreatocholangitis. Histopathology 60(2): 261-269.
-
Gupta RK, Xie BH, Patton KT, Mikhail L, Eric B, et al. (2016) Follicular pancreatitis: a distinct form of chronic pancreatitis-an additional mimic of pancreatic neoplasms. Hum Pathol 48: 154-162.
-
Hatzitheoklitos E, Büchler MW, Friess H, Disebastiano P, Bertram; B, et al. (1994) Pseudolymphoma of the pancreas mimicking cancer. Pancreas 9(5): 668-670.
-
Amer A, Mafeld S, Saeed D, Al-Jundi W, Beate H, et al. (2012) Reactive lymphoid hyperplasia of the liver and pancreas. A report of two cases and a comprehensive review of the literature. Clin Res Hepatol Gastroenterol 36(4): e71-e80.
-
Deshpande V, Zen Y, Chan JK, Eunhee E Yi, Yasuharu S, et al. (2012) Consensus statement on the pathology of IgG4-related disease. Mod Pathol 25(9): 1181-1192.
-
Jani N, Hani MB, Schulick RD, Hruban RH, Cunningham SC. Diagnosis and Management of Cystic Lesions of the Pancreas. Diagnostic and Therapeutic Endoscopy 2011: 1-9.
-
Okazaki K, Chiba T (2002) Autoimmune related pancreatitis. Gut 51(1): 1-4.
-
Mizuuchi Y, Aishima S, Hattori M, Yasuhiro U, Akira A, et al. (2014) Follicular pancreatitis, report of a case clinically mimicking pancreatic cancer and literature review. Pathol Res Pract 210(2): 118-122.
-
Umehara H, Okazaki K, Masaki Y, Mitsuhiro K, Motohisa Y, et al. (2012) Comprehensive diagnostic criteria for IgG4-related disease (IgG4-RD), 2011. Mod Rheumatol 22(1): 21-30.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient