Ischemic Proctitis: A Rare Clinical Situation
Acute ischemic proctitis is an extremely rare clinical entity. It occurs most often in hemodynamic instability in patients with atherosclerosis and those with cardiovascular risk factors. Many patients will need proctectomy as a definitive treatment, especially for gangrenous proctitis. We present the case of acute ischemic proctitis in a 54-year-old man followed for a valvular disease who presented with rectal bleeding as a tell-tale sign and who fully recovered with conservative management. We also review the literature on ischemic proctitis.
Introduction
Ischemic proctitis is a rare emergency because the rectum is very well vascularized [1, 2]. As in ischemic colitis, a spectrum of severity exists and ranges from superficial ischemia to total necrosis and perforation. Early recognition of this entity is of vital importance to avoid complications [3].
We present in this article the case of ischemic proctitis in a 45-year-old man and we discuss in the light of data from the literature the diagnostic and therapeutic dilemma of this nosological entity.
Case Report
A 54-year-old man presented to the hospital with low-abundance rectal bleeding for 5 days associated with moderate proctalgia without fever. He had no similar episode in the past or notion of recent travel. He was followed for mitral valve stenosis with tricuspid insufficiency under acenocoumarol 2 mg / day. He was also followed for arterial hypertension under ramipril 5 mg / day and asthma under symptomatic treatment.
On admission, his temperature was 37.1°C, blood pressure 150/91 mm Hg, heart rate 92 beats per minute, and oxygen saturation 98% in ambient air. Her abdominal examination revealed an undistended abdomen tender in the suprapubic area with no signs of peritoneal irritation. The digital rectal exam was painful and the finger cot was stained with blood.
An initial blood test revealed normal white blood cell count (8,320 / mm3), hemoglobin level of 14.7 g/dL with a hematocrit of 44% and platelets at 263,000/mm3. The C-reactive protein was 4.3 mg/l, the prothrombin level was 16.3% and the INR was 4.23. The remainder of the blood work was within normal limits.
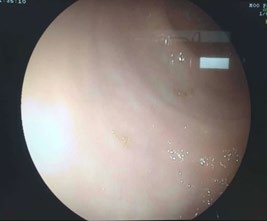
Colonoscopy revealed an erythematous and edematous mucosa growing in one piece from the lower and middle rectum with a clear line of demarcation from the rest of the recto-colic mucosa which appears normal (Figure 1).
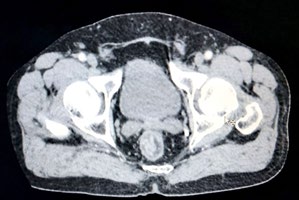
Abdomino-pelvic CT angiography revealed wall thickening of the middle and lower rectum with target enhancement after injection of contrast material (Figure 2). He also revealed atherosclerotic calcifications of the infra- renal abdominal aorta and its primary iliac dividing branches. Histological examination of the rectal biopsies confirmed the diagnosis of ischemic proctitis.


Our patient started oral antibiotic treatment with Metronidazol 1500 mg / day for 7 days with rehydration. He also benefited from a cardiology consultation with therapeutic adjustment.
Discussion
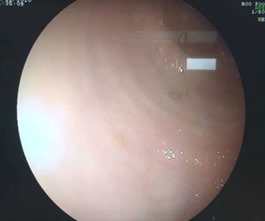
Ischemic proctitis is a rare entity due to the rich vascularization of the rectum. It is estimated at 2% for The course was marked by the disappearance of clinical symptoms from the tenth day. A follow-up colonoscopy performed on the 14th day revealed a normal-looking rectal mucosa (Figure 3). The patient is always followed regularly in consultation.
pure rectal locations and 10% for lesions associated with the sigmoid [1, 4]. Ischemic proctitis can be caused by acute vascular obstruction (usually after aortic surgery or radiologic intervention), severe vascular disease, or a low flow condition [4, 5, 6]. Other causes include radiation therapy, vasculitis, and myointimal hyperplasia of the mesenteric vein [7, 8]. It often occurs in elderly patients during significant hemodynamic disturbances (aortic surgery, states of shock). The clinical picture is often severe with a risk of progression to gangrene during the acute phase and then to chronic forms (stenosis, ulcerations) if this phase is passed [1, 4].
The clinical symptoms of patients with ischemic proctitis are often nonspecific and misleading. Patients often present with lower abdominal pain, diarrhoea with rectal bleeding and proctalgia. These presentations are nonspecific and are frequently seen in inflammatory bowel disease, pseudomembranous colitis or even colorectal tumor. Therefore, the distinction between these pathological entities is sometimes difficult [9, 10, 11].
The diagnosis must be evoked with the scanner in front of the existence of a segmental, circumferential and symmetrical wall thickening of the rectal wall in favor of a submucosal edema, with enhancement “in target” of the wall after injection testifying to a process. Acute [12] Fat infiltration and poor peritoneal fluid effusion are possible [13].
Colonoscopy is the test of choice for the diagnosis of ischemic proctitis. It allows visualization of mucosal lesions; to assess their severity and extent and to perform biopsies [14]. It should be done with caution, without excessive insufflation [15]. The segmental character is suggestive of an ischemic origin. The lesions are clearly defined and rapidly evolving. As in ischemic colitis, a spectrum of severity exists and ranges from superficial mucosal ischemia to necrosis with perforation. Three endoscopic stages are described: stage 1: edema and erythema of the mucosa, stage 2: non- necrotic ulcerations, based on an edematous mucosa, stage 3: extensive necrosis with gray-black appearance of the colon [16].
The therapeutic management of ischemic proctitis depends on its aetiology and the severity of the clinical picture and the results of endoscopy [14]. Early restoration of blood volume and optimization of cardiac output is essential. Conservative management is the rule for the majority of cases with non-severe ischemic proctitis [2]. Broad-spectrum antibiotics may be prescribed [1, 17]. The presence of gangrenous proctitis or perforation requires urgent surgery and in most cases complete proctectomy is necessary [18].
Conclusion
Ischemic proctitis is a rare entity. It should be considered in elderly patients with cardiovascular risk factors.
Conservative management should be favored in cases of superficial proctitis. Emergency surgery is the rule in cases of gangrenous proctitis.
References
-
Bharucha AE, Tremaine WJ, Johnson CD, Batts KP (1996) Ischemic proctosigmoiditis. Am J Gastroenterol 91(11): 2305-2309.
-
Sharif S, Hyser M (2006) Ischemic proctitis: case series and literature review. Am Surg 72(12): 1241-1247.
-
Silva M, Peixoto A, Albuquerque A, Rodrigues S, Gaspar R, et al. (2017) Clinical features and outcome of acute ischemic proctocolitis. Gastroenterol Hepatol 40(1): 28- 31.
-
Nelson Rl, Briley S, Schuler JJ, Abcarian H (1992) Acute ischemic proctitis. Report of six cases. Dis Colon Rectum 35(4): 375-380.
-
Nelson RL, Schuler JJ (1982) Ischemic proctitis. Surg Gynecol Obstet 154(1): 27-33.
-
Jaeger HJ, Mathias KD, Gissler HM, Neumann G, Walther LD (1999) Rectum and sigmoid colon necrosis due to cholesterol embolization after implantation of an aortic stent-graft. J Vasc Interv Radiol 10(6): 751-755.
-
Savoie LM, Abrams AV (1999) Refractory proctosigmoiditis caused by myointimal hyperplasia of mesenteric veins: Report of a case. Say Colon Rectum 42(8): 1093-1096.
-
Reissman P, Weiss EG, Teoh TA, Lucas FV, Wexner SD (1994) Gangrenous ischemic colitis of the rectum: A rare complication of systemic lupus erythematosus. Am J Gastroenterol 89(12): 2234-2236.
-
Ritchie JK, Lennard-Jones JE (1976) Crohn’s disease of the distal large bowel. Scand J Gastroenterol 11(5): 433- 436.
-
Brandt LJ, Boley SJ, Mitsudo S (1982) Clinical characteristics and natural history of colitis in the elderly. Am J Gastroenterol 77(6): 382-386.
-
Brandt LJ, Katz HJ, Wolf EL, Mitsudo S, Boley SJ (1985) Simulation of colonic carcinoma by ischemia. Gastroenterology 88(5): 1137-1142.
-
Cuénod Ca, Wind P, Siauve N, Clément O, Bénichou J, et al. (1999) Diagnosis of acute abdominal emergencies of digestive origin in adults. Contribution of imagery. Gastroenterol Clin Biol 23: 1170-1186.
-
Balthazar EJ, Yen BC, Gordon RB (1999) Ischemic colitis: CT evaluation of 54 cases. Radiology 211(2): 381-388.
-
Gandhi SK, Hanson MM, Vernava AM, Kaminski Dl, Longo WE (1996) Ischemic colitis. Dis Colon Rectum 39(1): 88- 100.
-
Brandt LJ, Boley SJ (1992) Colonic ischemia. Surg Clin North Am 72(1): 203-229.
-
Aubert A, Fritsch J (1997) Ischemic colitis. Endoscopic diagnosis. J Chir 134: 94-96.
-
Abhishek K, Kaushik S, Kazemi MM, El-Dika S (2008) An unusual case of hematchentia: acute ischemic proctosigmoiditis. J Gen Intern 23(9): 1525-1527.
-
Khawaja A, Raphaeli T (2013) Acute ischemic gangrene of the rectum: Report of 3 cases and review of literature. International Journal of Surgery Case Reports 4(12): 1120-1123.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient