Comprehensive Liver Cancer Center Approach to Improve Treatment Lag Time in Patients with Hepatocellular Cancer: A Tertiary Center Experience
Background: Hepatocellular carcinoma (HCC) is a leading cause of death among patients with liver disease. A new Comprehensive Liver Cancer Center (CLCC) was established at our institution that adopted a same-day, single-visit approach to formulate a plan of care and expedite interventions. Methods: We retrospectively reviewed charts of patients diagnosed with HCC before and after the establishment of the CLCC. The cohort was divided into two groups: those who received care prior to (group 1) and after (group 2) the establishment of the CLCC. TL-T was calculated from the date of diagnosis to the date of the first therapeutic intervention and compared using a t-test. TL-T was compared using a t-test, other variables were compared using Fisher’s exact, and chi-square tests. Results: From the total cohort: 117 (40%) were in group 1 and 172 (60%) in group 2. Mean distance traveled by patients to seek care was 12.64 vs 16.06 miles, for groups 1 and 2 respectively. A larger number of patients presented within Milan criteria in group 2. Mean TL-T improved significantly after the implementation of CLCC; 152 to 69 days. Despite not reaching statistical significance, there was a decrease in the 1-year mortality in group 2 compared to group 1 (17% vs 11%, p= 0.16) respectively. Conclusion: A multidisciplinary approach is critical in the management of HCC. While the data did not suggest a significant change in secondary outcomes thus far, it demonstrated that our institution’s new CLCC was able to significantly reduce TL-T ensuring potentially better outcomes.
Introduction
Hepatocellular carcinoma (HCC), a common complication of cirrhosis, is the fifth most common malignancy in the world and the third leading cause of cancer-related death worldwide [1]. The disease is accountable for 500,000 deaths annually nationwide, resulting in substantial healthcare resource utilization from HCC-related admissions alone [2, 3]. The one-year survival rate for untreated HCC is less than 20%, but this rate improves to over 75% for patients with limited stage disease who undergo curative treatments in a timely fashion [4, 5]. Up to 30% of patients with HCC present with limited-stage disease, yet despite this prevalence, data suggest disconcerting patterns of underutilization of evidence-based therapies for these patients [6, 7]. HCC is a heterogeneous malignancy, most often arising in a diseased organ, with a vast array of possible therapies that rely upon several clinical factors including hepatic function, tumor stage and burden, functional status and institutional proficiency. Unlike other cancers, diagnosis can be made solely by dynamic imaging, and HCC is the only solid organ tumor for which transplant offers a cure, emphasizing the importance in minimizing treatment lag-time (TL-T).
Due to the complexities involved in the treatment of HCC, a multidisciplinary approach is indicated, consisting of a team of providers with complementary expertise and skillsets: hepatology, diagnostic radiology, interventional radiology, surgery, medical and oncology, and pathology. Multidisciplinary conferences facilitate open communication amongst specialists, however their facilitation alone may not necessarily translate to optimal treatment-lag times (TL-T). Patients are still often required to meet with each individual provider for consultation and work-up (diagnostic imaging, biopsy, etc.) on varying clinic days and sometimes even across various institutions, resulting in substantial delays to potentially curative therapies.
For these reasons, a novel approach was adopted at our tertiary care institution: the formation of a multidisciplinary Comprehensive Liver Cancer Center (CLCC). Akin to multidisciplinary oncology clinics, this model facilitates a same-day, single-visit with multiple providers, allowing rapid organization of treatment plans and subsequent interventions with multidisciplinary consensus. The objective of this study was to retrospectively evaluate the impact of a CLCC on the treatment of HCC at a tertiary care center, as measured by TL-T and patient outcomes such as time to liver transplant and overall mortality, before and after implementation of the CLCC.
Methods
Intervention
The CLCC approach was organized at our institution after several years of administrative planning and resource allocation to ensure feasibility. In this model, newly referred patients meet for consultation with a board-certified hepatologist, surgeon, interventional radiologist, and medical oncologist back-to-back within a shared clinic space during a single hospital visit.
Following the initial encounter, the treating physicians convene for multidisciplinary discussion and establishment of a consensus treatment plan. Pertinent work-up studies are reviewed conjointly, with radiology and pathology available for relevant questions. Following academic discussion, each provider again meets with the patient to relay the finalized treatment plan and address any questions regarding care, still within the same-day hospital visit setting. Any necessary additional studies or follow-up appointments are ordered and coordinated at that time, with the aid of support staff including a trained registered nurse navigator, resident physician, or mid-level practitioner.
Outcomes
Primary outcome included determining TL-T. This was defined as the period from date of diagnosis to date of first therapeutic intervention. TL-T was calculated for each patient and compared among groups via t-test analysis. Several other factors were taken into account: one-year mortality, mean distance traveled by patients to seek therapy, number of patients receiving liver transplant and time to transplant.
Study Population
From the inception of the CLCC, an accompanying prospective database was established and maintained to demonstrate effectiveness of the model. For the present study, follow-up information from patients with HCC was gathered and analyzed from the database through a five-year time period. For comparison, data from patients diagnosed with HCC before the establishment of the CLCC was analyzed from two-year time period. The entire cohort was divided into two groups: Those who received care prior to establishment of the CLCC (Group 1; pre-CLCC) and those who received care after CLCC was established (Group 2; post-CLCC). Patients lost to follow-up or those who enrolled in hospice care were excluded from the study population.
Statistical Analysis
TL-T was calculated for each patient and compared among groups via t-test analysis. Other data for evaluation included baseline demographic characteristics, distance traveled for healthcare (calculated from residence to tertiary care facility), underlying risk factors or HCC, method of diagnosis, transplantation, and one-year mortality. These variables were analyzed using Fisher’s exact and chi-square tests as appropriate. A p-value less than 0.05 were considered statistically significant for all analyses. The institutional review board at our institution approved this study.
Results
Patient Demographics and Clinical Characteristics
A total of 289 patients with HCC were evaluated in a five-year time period at our institution, of which, 117 patients (40%) were in Group 1, and 172 patients (60%) were in Group 2. The study population was approximately 80% male, with mean ages of 59 and 62 years in Groups 1 and 2, respectively. Caucasians comprised the majority of the population in both groups, 52 patients (44%) in Group 1 and 74 patients (43%) in Group 2, followed by African Americans, 40 patients (34%) in Group 1 and 54 patients (31%) in Group 2.
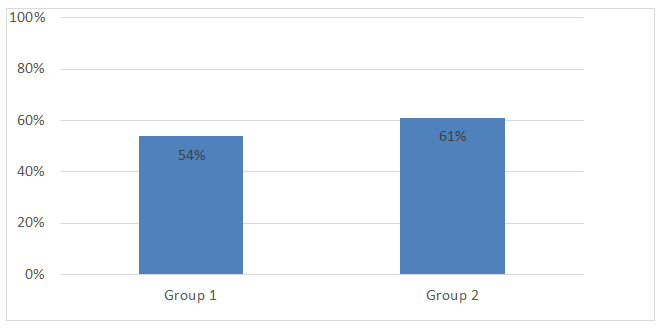
The etiology of HCC in this population was heavily weighted towards viral hepatitis. Majority (n=207, 72 %) developed HCC following hepatitis C virus (HCV) infection (Table 1). A total of 89 patients (76%) in Group 1 and 118 patients (69%) in Group 2 had underlying HCV infection. Other common causes included alcoholic cirrhosis as well as concomitant alcoholic and HCV cirrhosis. The stage of HCC at initial presentation was variably distributed and comparable between both groups. A significantly larger number of patients in Group 2 (n= 105, 61%) presented within Milan criteria versus the number in Group 1 (n=63, 54%) (Figure 1). MRI and CT were both equally useful to establish diagnosis of HCC in Group 1, n=55(47%) and n=56(48%) respectively, while MRI was the more commonly utilized diagnostic modality for HCC diagnosis in Group 2, n=123 (71%) vs n=28(16%).
| Pre- CLCC (117) | Post-CLCC (172) | P-value | |
|---|---|---|---|
| Age mean (SD) | 58.68 (7.24) | 61.63 (8.85) | 0.003 |
| Males | 93 (79.48) | 138 (80.23) | 0.882 |
| Race | |||
| White | 52 (44.44) | 74 (43.02) | 0.355 |
| African American | 40 (34.18) | 54 (31.39) | 0.355 |
| Other | 25 (21.36) | 22 (12.79) | 0.355 |
| Method of Diagnosis | |||
| MRI | 55 (47.00) | 123 (71.51) | <0.001 |
| CT | 56 (47.86) | 28 (16.27) | <0.001 |
| Biopsy | 6 (5.12) | 3 (1.74) | <0.001 |
| Stage at Presentation (within Milan) | 63 (53.84) | 105 (61.04) | 0.227 |
| MELD at diagnosis mean (SD) | 10.61 (3.76) | 12.33 (1.52) | 0.083 |
| Underlying Etiology | |||
| HCV | 89 (76.06) | 118 (68.60) | 0.636 |
| HBV | 3 (2.56) | 11 (6.39) | 0.636 |
| ETOH liver disease | 8 (6.83) | 13 (7.55) | 0.636 |
| ETOH + HCV | 5 (4.27) | 8 (4.65) | 0.636 |
| Cryptogenic | 5 (4.27) | 7 (4.06) | 0.636 |
| Other | 7 (5.98) | 15 (8.72) | 0.636 |
| Procedure | |||
| TACE | 74 (63.24) | 92 (53.48) | 0.051 |
| RFA | 37 (31.62) | 57 (33.13) | 0.051 |
| Resection | 6 (5.12) | 23 (13.37) | 0.051 |
| Treatment Lag mean (SD) | 152.08 (241.27) | 68.85 (57.9) | <0.001 |
| Transplantation | 34 (29.05) | 45 (26.16) | 0.593 |
| Time to Transplant Mean (SD) | 465.5 (273.85) | 419.65 (187.70) | 0.377 |
| Miles traveled to obtain care Mean (SD) | 12.64 (17.98) | 16.06 (22.71) | 0.283 |
| One-year Mortality | 20 (17.09) | 19 (11.04) | 0.161 |
Table 1: Baseline Characteristic and Outcomes of Study Population. Data are presented as N. (%) unless otherwise specified.
Primary Outcomes
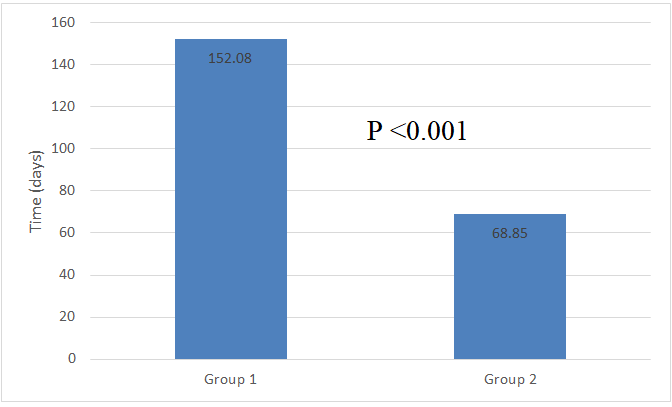
To determine whether the establishment of the CLCC improved HCC patient outcomes at our institution, we compared several metrics including TL-T, one-year mortality, and mean distance traveled by patients to seek therapy, among both groups. TL-T served as a primary outcome in our study. Mean TL-T improved significantly after the implementation of the CLCC: from 152 to 69 days (p<.001) (Figure 2). Despite not reaching statistical significance, there was also a notable decrease in one-year mortality in Group 2 as compared to Group 1 (17% vs. 11%, p=0.16).
Secondary Outcomes
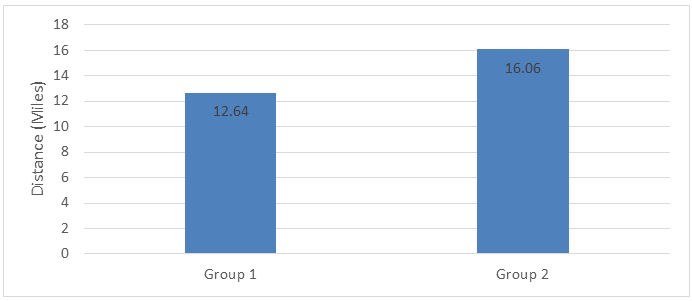
The mean distance traveled by patients to seek care was 12.64 versus 16.06 miles for Groups 1 and 2, respectively (Figure 3) p-value (0.283). Although not statistically significant, there is obvious disparity in the average number of miles traveled for therapy after establishment of CLCC. This served as a measure of interest of the patients in our program. Number of patients receiving liver transplant was comparable in both groups, 45 patients (26%) in Group 1 vs 34 patients (29%) in Group 2. However, shorter time to transplant was noted among patients in Group 2 when compared to Group 1, 419 days (SD 188) vs 465 days (SD 273 days) despite lack of statistical significance (p=0.377). Finally, when one-year mortality was compared between both groups, a notable reduction in mortality was seen in patients post CLCC (11% vs 20%, p=0.161).
Discussion
HCC is an aggressive malignancy which carries a poor prognosis in the absence of therapy. Without treatment, median survival is less than eight months, with five-year overall survival rates approaching zero [8.9]. The incidence of HCC continues to rise in the United States [10, 11] and for cancer patients who do receive treatment, there is a clear correlation between treatment delay (>90 days) and decreased overall survival [12, 13]. Taken together, these figures highlight the significance of reducing TL-T for the ideal management of this disease. However, achieving optimal care can be complex for patients with HCC, for which the rising incidence, genetic heterogeneity, varying etiology and concurrent chronic liver disease make diagnosis, staging, and selection of treatment challenging. A multidisciplinary approach is necessary for the management of these patients, who benefit from the commitment of multiple caregivers supporting them throughout their disease course.
To improve TL-T, associated outcomes, and the patient healthcare experience, our institution adopted a multidisciplinary CLCC model to facilitate HCC-related care. This paradigm entails a same-day, single visit with multiple healthcare providers leading to rapid formulation of a consensus plan and expedition of subsequent work-up and interventions. The present study now demonstrates measurable patient benefits associated with the implementation of a CLCC model. With the adoption of a CLCC approach, mean TL-T for our patients significantly decreased from roughly 5 months (152.08 days) to just 2 months (68.85 days), translating to an average TL-T reduction of nearly 3 months (83 days). These reductions are attributable to the simultaneous presence of all essential providers at the same clinic visit, thereby eliminating unnecessary delays due to scheduling and appointment coordination alone.
Such a model is particularly important for the underserved patient population of our tertiary care institution. The majority of these patients fall into the lower socioeconomic strata, and many lack the means to miss work and travel back-and-forth to our center for multiple appointments. Although not statistically significant, interestingly, the mean distance traveled to seek care was greater for patients in Group 2 (post-CLCC) than for those in Group 1 (pre-CLCC): 16.06 versus 12.64 miles, respectively (p=0.283), suggesting that patients in Group 2 were willing to endure a longer commute to the hospital. The ease and efficiency of the CLCC model may perhaps facilitate healthcare for a larger population which may otherwise be restricted due to logistical constraints such as distance, work responsibilities, and family obligations.
Complementary results have been published from other studies evaluating the treatment of HCC in the multidisciplinary setting [10, 11]. Chang et al, noted that a greater proportion of patients were evaluated at early (and potentially curable) stages of HCC following implementation of a multidisciplinary model [11], likely associated with reductions in referral times with such an approach. In our study, we also found that a greater proportion of patients in Group 2 (post-CLCC) presented within Milan criteria versus that of Group 1 (pre-CLCC): 61% versus 54% (p=0.227) (Figure 1). This difference may be attributed to streamlined screening and efficient work-up following the induction of the CLCC model, as well as increased referral rates from other providers due to publicity of the CLCC following inception.
Finally, while not statistically significant, a trend towards improved survival outcomes in the post-CLCC setting was also noted, with one-year mortality decreasing from 17% to 11% for Groups 1 and 2, respectively (p=0.16). This reduction may reflect improvements in detection and treatment in the modern era, but may also be a product of the significant decrease in TL-T in the post-CLCC setting, given the strong correlation between treatment delay and decreased survival [12, 13].
Conclusion
The CLCC model fundamentally builds on existing standards of care with aim of improving outcomes among patients diagnosed with HCC and patient compliance. The establishment of a CLCC at our tertiary care center has been associated with shorter time to potentially curative treatments with high potential to translate into an improvement in disease outcomes. These data advocate for the increased adoption of multidisciplinary care occurring nationally. Furthermore, multidisciplinary teams are becoming the standard of care globally for treatment of multiple cancers, driven in part by the publication of national guidelines recommending their use and composition [14, 15]. Future studies of the CLCC model can elucidate the cost benefit associated with the CLCC model, and longer follow-up may translate into expected long-term survival and quality- of-life outcomes for these patients.
Summary
- Hepatocellular carcinoma (HCC) is a leading cause of death among patients with liver disease.
- A multidisciplinary approach is critical in the management of HCC.
- Akin to multidisciplinary oncology clinics, Comprehensive liver cancer center (CLCC) facilitates a same-day, single-visit with multiple providers, allowing rapid organization of treatment plans and subsequent interventions with multidisciplinary consensus.
- CLCC can significantly reduce treatment lag time (TL-T) ensuring potentially better outcomes.
- CLCC is particularly important for the underserved patient population. Many patients from lower socioeconomic strata lack the means to travel back-and- forth for multiple appointments.
References
-
Sherman M, Burak K, Maroun J, Metrakos P, Knox JJ, et al. (2011) Multidisciplinary Canadian consensus recommendations for the management and treatment of hepatocellular carcinoma. Current Oncology 18(5): 228- 240.
-
Kim WR, Gores GJ, Benson JT, Therneau TM, Melton LJ (2005) Mortality and hospital utilization for hepatocellular carcinoma in the United States. Gastroenterology 129(2): 486-493.
-
Lang K, Danchenko N, Gondek K, Shah S, Thompson D (2009) The burden of illness associated with hepatocellular carcinoma in the United States. J Hepatol 50(1): 89-99.
-
Cabibbo G, Enea M, Attanasio M, BruixJ, CraxìA, et al. (2010) A meta-analysis of survival rates of untreated patients in randomized clinical trials of hepatocellular carcinoma. Hepatology 51(4): 1274-1283.
-
Pelletier SJ, Fu S, Thyagarajan V, Romero-Marrero C, Batheja MJ, et al. (2009) An intention-to-treat analysis of liver transplantation for hepatocellular carcinoma using organ procurement transplant network data. Liver Transpl 15(8): 859-868.
-
Wong RJ, Corley DA (2009) Survival differences by race/ ethnicity and treatment for localized hepatocellular carcinoma within the United States. Dig Dis Sci 54(9): 2031-2039.
-
El-Serag HB, Siegel AB, Davila JA, Shaib YH, Cayton-Woody M, et al. (2006) Treatment and outcomes of treating hepatocellular carcinoma among Medicare recipients in the United States: a population-based study. J Hepatol 44(1): 158-166.
-
Akashi Y, Koreeda C, Enomoto S, Uchiyama S, Mizuno T, et al. (1991) Prognosis of unresectable hepatocellular carcinoma: an evaluation based on multivariate analysis of 90 cases. Hepatology 14(2): 262-268.
-
Okuda K, Ohtsuki T, Obata H, Tomimatsu M, Okazaki N, et al. (1985) Natural history of hepatocellular carcinoma and prognosis in relation to treatment. Study of 850 patients. Cancer 56(4): 918-928.
-
Yopp AC, Mansour JC, Beg MS, Arenas J, Trimmer C, et al. (2014) Establishment of a multidisciplinary hepatocellular carcinoma clinic is associated with improved clinical outcome. Ann Surg Oncol 21(4): 1287- 1295.
-
Chang TT, Sawhney R, Monto A, Davoren JB, Kirkland JG, et al. (2008) Implementation of a multidisciplinary treatment team for hepatocellular cancer at a Veterans Affairs Medical Center improves survival. HPB (Oxford) 10(6): 405-411.
-
Singal AG, Waljee AK, Patel N, Chan EY, Tiro JA, et al. (2013) Therapeutic delays lead to worse survival among patients with hepatocellular carcinoma. J Natl Compr Canc Netw 11(9): 1101-1108.
-
Richards MA, Westcombe AM, Love SB, Littlejohns P, Ramirez AJ, et al. (1999) Influence of delay on survival in patients with breast cancer: a systematic review. Lancet 353(9159): 1119-1126.
-
Naugler WE, Alsina AE, Frenette CT, Rossaro L, Sellers MT (2015) Building the multidisciplinary team for management of patients with hepatocellular carcinoma. Clin Gastroenterol Hepatol 13(5): 827-835.
-
Murray KF, Carithers RL (2005) AASLD practice guidelines: Evaluation of the patient for liver transplantation. Hepatology 41(6): 1407-1432.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient