Orbital Myositis Revealing Crohn’s Disease
Orbital myositis (OM), defined by the inflammation of one or more of extra ocular muscles was exceptionally reported in Cohn’s disease (CD) especially as initial presentation before the development of intestinal manifestations. We report a case of OM preceding CD. Through our observation and a review of the literature, we specify the epidemioclinical, therapeutic and evolutionary characteristics of this rare entity.
Introduction
Extra intestinal signs of Cohn’s disease (CD) are various including rheumatologic manifestations, cutaneous, ophthalmologic and hepato-biliary involvements. Ocular manifestations are infrequent with prevalence less than 10%. They are mainly represented by: episcleritis, uveitis and scleritis. Orbital myositis (OM), defined by the inflammation of one or more of extraocular muscles was exceptionally reported in CD even more as initial presentation before the development of intestinal manifestations [1, 2]. Herein we report a case of OM preceding CD.
Observation
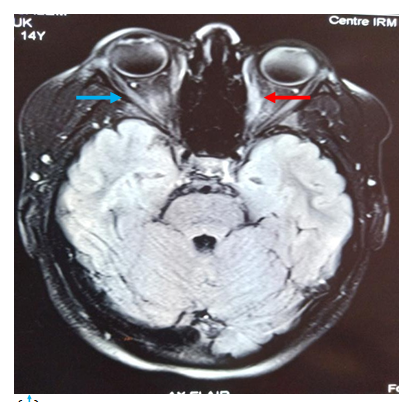
A 19-year-old female with no significant medical history presented to the hospital in October 2015 with acute convergent strabismus and double vision. She was hospitalized in ophthalmology department and underwent orbital magnetic resonance imaging (MRI) at emergency that was consistent with orbital myositis (Figure 1). Cerebral and medullar MRI was otherwise normal.
The patient received high doses of corticosteroids (2mg/kg/day) for 6 weeks then she was referred to internal medicine department for further investigations. At her admission she had no ophthalmologic or systemic complaints. In her initial biological assessment we found: hemoglobin at 11.5 g/dl, erythrocyte sedimentation rate (ESR): 16mm (H1); C-reactive protein (CRP): 9 mg/l, Creatinin kinase (CK): 42 U/l, LDH: 211 AST/ALT 18 /18 U/l. Infectious investigations were negatives including HSV(herpes simplex virus), HCV(hepatitis C virus), HBV(hepatitis B virus), HIV(human immunodeficiency virus), EBV(Epstein Barr virus), CMV(cytomegalovirus), VZV(varicella zoster virus), ParvoB19, VDRL-RPR,, bartonella, rickettsia, toxoplasmosis and tuberculosis. Thyroid function tests including thyroid stimulating hormone (TSH), thyroid peroxidase autoantibodies (TPO), thyroglobilin auto antibodies, TSH- receptor auto antibodies were negatives. Immunologic analysis revealed negative results (antinuclear antibodies (ANA), anti-neutrophil cytoplasmic autoantibody (ANCA), anti cardiolipin antibodies and kit- myositis). Her orbital finding was attributed to idiopathic orbital myositis and the patient received 6 months of steroids then progressively stopped. One month after stopping corticosteroids, on May 2016 the evolution was marked by the recurrence of myositis which became bilateral. Biopsy of internal orbital muscle showed myofiber regeneration with necrotic lesions, and prominent endomysial inflammatory infiltrate (Figure 2).
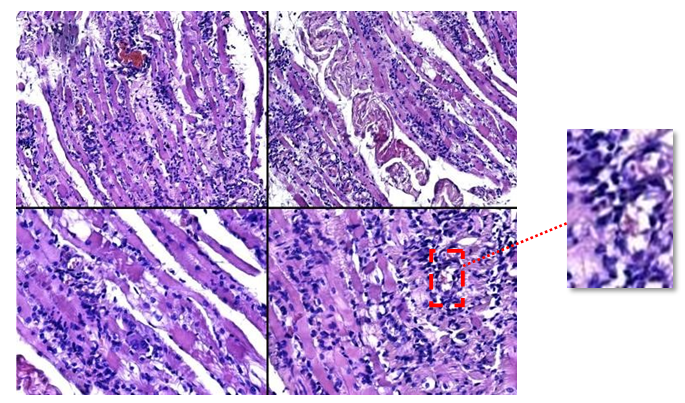
Those findings were concordant with orbital myositis. Therefore, adjunction of azathioprin has been started (2.5 mg/kg/day) with good progress and it was maintained for 3 years. On April 2019 decision was to stop azathioprin and maintain low doses of steroids. On her follow-up, in December 2020, she presented diffuse abdominal pain with constipation. Then she was referred to gastroenterology department for endoscopic explorations. At her admission, physical examination found tenderness on palpation of the iliac right fossa. Perianal and rectal examination was normal.
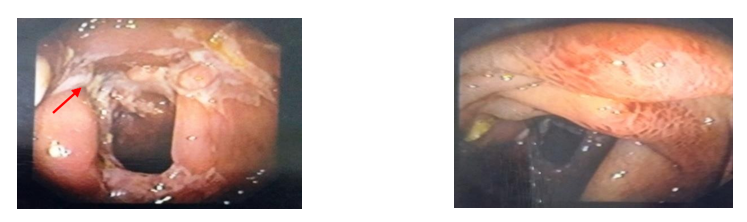
Laboratory analysis showed anemia with haemoglobin at 9.9 g/dl with mean corpuscular volume (MCV) at 74 fl and elevated CRP at 131 mg/l. The patient underwent ileocolonoscopy revealing ulcerative ileocecal valve with stenosis and two fistulous paths (Figure 3). Colonic mucosa was normal. Histologic examination showed important acute and chronic inflammation with ulcerations of the Bauhin’s valvula and the anal canal. There is no evidence of necrotizing vasculitis or granulomas. The upper endoscopy was also practiced revealing antral follicular gastritis and erosive bulbous duodenitis. Biopsy of the Duodenum was normal with preservation of villous architecture and no increase intraepithelial lymphocytes. Biopsy of gastric antrum / body didn’t reveal histopathologic abnormalities. The MR enterography showed active fistulizing Cohn’s (Figure 4).
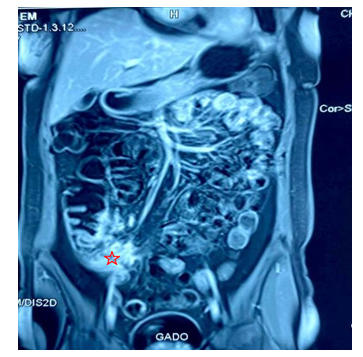
MR Enterography showing active fistulizing Cohn’s disease: bowl wall thickening of the terminal ileum extended over 6 cm ileum, multiple fistulous paths without abscesses, jejunal wall thickening extended over 18 cm, sclerolipomatosis. Diagnosis of Crohn disease was retained and orbital myositis had been attached to inflammatory bowel disease. The patient was treated by combined treatment face to her young age and fistulizing character of the luminal disease. Double therapy was based on azathioprine associated with TNF alpha inhibitor. The initial evolution was favorable (current follow-up of 1 month).
Discussion
Ocular manifestations occur in 2-5% of patients with crohn’s disease and can precede luminal diseases [3]. The most common oribitary manifestations are: episcleritis, anterior uveitis with a frequency between 2 -4% and scleritis occurring in 1% of cases [3]. Orbital myositis is a very rare extra intestinal manifestation of crohn‘s disease, with only few cases reported in the literature [4]. Pathogenesis is unidentified, but is possibly correlated to underlying immune- mediated processes. In our case the diagnosis of CD was retained after 5 years than the ocular myositis. Coming
back to our investigations showed negative findings and ruled out all causes of OM (viral, bacterial, vascular, trauma, lupus, and sarcoidosis). Then OM couldn’t be explained by another cause other than CD. The evaluation of the few cases of CD with OM found female predominance, in half OM precedes the onset of CD and the involvement was bilateral in also 50% of cases [5]. As you noticed in the observation, ocular signs respond well to corticosteroids and azathioprine as in the majority of patients who were evaluated in literature reviews [6].
Conclusion
We report a rare case of orbital myositis that precedes gastro intestinal manifestations in Cohn’s disease. This observation is original for two reasons: the rarity of this type of ocular involvement during IBD and its occurrence several years before the appearance of the digestive localization.
References
-
Montagnese F, Wenninger S, Schoser B (2016) “Orbiting around” the orbital myositis: clinical features, differential diagnosis and therapy. J Neurol 263(4): 631-640.
-
Verma S, Kroeker KI, Fedorak RN (2013) Adalimumab for orbital myositis in a patient with Crohn’s disease who discontinued infliximab: a case report and review of the literature. BMC Gastroenterol 13: 59.
-
Bernstein CN, Blanchard JF, Rawsthorne P, Yu N (2001) The prevalence of extraintestinal diseases in inflammatory bowel disease: a population-based study. Am J Gastroenterol 96(4): 1116-1122.
-
Durno CA, Ehrlich R, Taylor R, Buncic JR, Hughes P, Griffiths AM (1997) Keeping an eye on Crohn’s disease: orbital myositis as the presenting symptom. Can J Gastroenterol 11(6): 497-500.
-
Culver EL, Salmon JF, Frith P, Travis SPL (2008) Recurrent posterior scleritis and orbital myositis as extra-intestinal manifestations of Crohn’s disease: Case report and systematic literature review. J Crohn’s and Colitis 2(4): 337-342.
-
Önder Ö, Bilgin RR, Köşkderelioğlu A, Gedizlioğlu M (2016) Orbital Myositis: Evaluating Five New Cases Regarding Clinical and Radiological Features. Noro Psikiyatr Ars 53(2): 173-177.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient