Isolated Rectal Ganglioneuromatous Polyposis
A 29-year-old man with a history of irritable bowel syndrome presented with intermittent diffuse abdominal pain associated with passage of loose stool over the past several years. He denied weight loss and a history of gastrointestinal carcinoma.
Short Communication
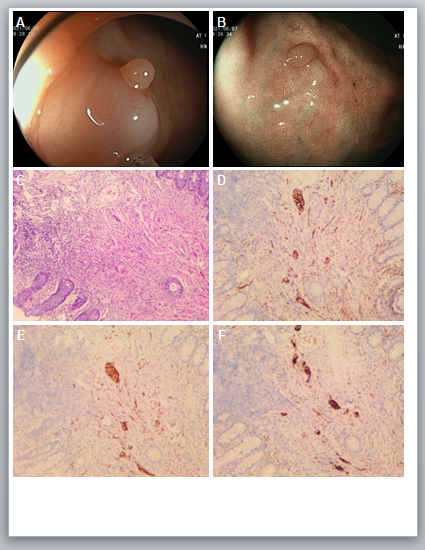
A 29-year-old man with a history of irritable bowel syndrome presented with intermittent diffuse abdominal pain associated with passage of loose stool over the past several years. He denied weight loss and a history of gastrointestinal carcinoma. Physical examination was unremarkable. His abdomen was soft, nondistended, and nontender to palpation. Colonoscopy revealed a sessile polyp in the rectum, in size approximate 5 mm (Figure 1A), which was further defined by flexible spectral imaging color enhancement and blue laser imaging technology (Figure 1B). Endoscopic mucosal resection was performed to remove the polyp. Histologic review of the resected polyp showed enlarged nerve bundles with spindle cells and ganglion cells by hematoxylin and eosin staining (Figure 1C). Positive immunohistochemical staining for S100, SOX-10, and Syn was demonstrated (Figure 1D-F). Endoscopically and histologically, the isolated polyposis was consistent with polypoid ganglioneuromas. Ganglioneuromas are uncommonly encountered in the gastrointestinal tract, arise from a proliferation of ganglionic cells of the sympathetic nervous system, which have no phenotypic characteristics to help distinguish them endoscopically [1]. Ganglioneuromas are typically benign, belong to ectodermal neoplasms, which have characteristic histology to distinguish from Schwann’s cells, ganglion cells, and nerve fibers [2]. Polypoid ganglioneuromas, are usually solitary and small, whose pathophysiology may be related to a complex hyperplasia of cholinergic, peptidergic, and adrenergic neuronal tissue [3]. Because of no clinical guidelines, the optimal clinical management and colorectal surveillance of ganglioneuromatous polyposis are unknown [4]. We plan to repeat colonoscopic surveillance in 1 year for this patient.
Ethical Statement
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Written informed consent was obtained from the patient for publication of this “GI Image”. Board institutional approval was not required.
References
-
Aryan M, Mejbel H, Weber F (2022) A Most Unusual Polyposis. Gastroenterology 162(3): e14-e16.
-
Nazir TM, Friel C, Moskaluk CA (2008) Clinical challenges and images in GI. Ganglioneuromatosis polyposis. Gastroenterology 134(2): 386-646.
-
Abraham G, Prakash SR (2015) Solitary Colonic Ganglioneuroma: A Rare Incidental Finding of Hematochezia. Case reports in gastrointestinal medicine 2015: 794985.
-
Trufant JW, Greene L, Cook DL, McKinnon W, Greenblatt M, et al. (2012) Colonic ganglioneuromatous polyposis and metastatic adenocarcinoma in the setting of Cowden syndrome: a case report and literature review. Hum pathol 43(4): 601-604.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient