A Case of Large Gastric Trichobezoar in the Corona Era: Case Report and Review of Literature
Background: Trichobezoars are uncommon cases of concretions of swallowed hair retained within the digestive tract, most commonly the gastric outlet and duodenum. Despite being reported in many ages, they predominate in young females during childhood and adolescence diagnosed with bezoars and are usually associated with psychiatric illness. These usually develop insidiously and hence at presentation are large in size and the patient complains of acquired alopecia. In this report, we present a covid-19 positive case of a young female patient diagnosed with trichophagia with large 17.5 × 12.2 × 5 cm trichobezoar that had to be surgically removed.
Introduction
Trichobezoars were first described by Baudomant in 1779, consisting of a compact mass of hair, occupying the gastric cavity to a various extent. The term “bezoar” is thought to be derived from the Arabic word for antidote – “bazahr” or “badzehr”, because stones obtained from the stomach or intestines of animals were thought to have medicinal properties [1]. Bezoars can be classified in four types: phytobezoar (vegetable), trichobezoar (hair), lactobezoar (milk/curd) and miscellaneous (fungus, sand, paper, etc). They are usually found in the stomach, but they may also be found in the duodenum and other parts of the intestine. The most frequent type of bezoar in adults is phytobezoar, while trichobezoars are more often found in children and teenage girls. The pathogenesis of bezoars is not consensual. It is believed that the smooth surface of hair does not allow for its propagation through peristalsis, getting trapped in the mucosa. However, the stomach of normal individuals is able to clear even large foreign bodies in up to 80 to 90% of the cases, which may imply that bezoar formation occurs in the presence of both altered gastric anatomy or physiology and continued ingestion of the offending substance. When the trichobezoar is seen extending from the stomach to various lengths of the intestine is called “Rapunzel Syndrome”, for its resemblance to a tail [2].
Trichobezoars present with signs and symptoms of acute abdomen and gastric tract obstruction. These include abdominal pain, nausea, bilious vomiting, hematemesis, anorexia, early satiety, weakness, weight loss and abdominal mass, depending on the degree of obstruction. The diagnosis of trichobezoars is based on imagiologic evidence. Ultrasonography is effective in detecting an epigastric mass, although CT-scan is more accurate in revealing a characteristic bezoar image and allowing the identification of the presence of additional gastrointestinal bezoars. The definite diagnosis is established by endoscopy. Trichobezoars demand aggressive treatment, often implying surgical intervention, without which mortality rates may be high [3, 4]. Trichobezoars are usually described in the context of an underlying psychiatric disorder, trichotillomania in particular which is also implicitly taken as cause of it, and usually accompanied by characteristic features such as signs of alopecia [2, 3]. Although trichobezoars are well described in terms of surgical diagnosis and procedure, there are only but scarce reports on psychiatric literature. This case report describes the case of a 14- year-old female patient diagnosed with a trichobezoar who had a previous similar diagnosis without any psychiatric evaluation or management.
Case Presentation
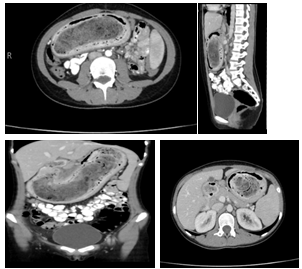
A 14-year-old girl female patient who weighed 40 kg was referred to the King Abdallah University Hospital in Jordan as a case of Repunzal syndrome confirmed by CT scan. She was complaining of weight loss, nausea and early satiety for 6 months after sudden dying of her father due to a road traffic accident, also sometimes nausea developed into vomiting with an abdominal epigastric pain which was the chief complaint she came with. Her mother reported that her daughter is generally active, did not have any medical or surgical illnesses, but she had trichophagia. On examination, It revealed that the patient had looked pale, ill, thin, below average total body weight with large non-pulsatile mobile epigastric mass extending towards to the umbilicus was noticed .There was no sign of trichotillomania. An Abdomen and pelvis CT scan with oral and IV contrast that confirmed the diagnosis of the patient as a trichobezoar ,stated that There is a large heterogenous intraluminal mass with mottled gas pattern in the stomach, extending through the pylorus up to the first part of duodenum ,it seemed to be separable from the gastric wall .It left a small area of the gastric lumen and encroached upon posterior abdominal structures, compressing the IVC and 3rd part of the duodenum decreasing SMA-Aortic angel. So the overall findings were highly suggestive for trichobezoar/Rapunzel syndrome with possible fluid collection and extraluminal foci of gases in the lesser sac and multiple enlarged gastro hepatic lymph nodes with the largest one measuring about 1.2 cm.
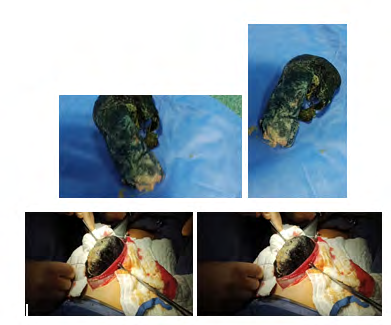
After the admission and referral, the psychiatric team was consulted for her case and further after she underwent a number of Laboratory investigations including CBC, KFT, LFT, Amylase, Lipase, COVID-19 and barium follow through was ordered. The results revealed she is COVID-19 +Ve and had low Hb (10.5 g\dl, due to chronic malnutrition) other biochemistry and serology tests were normal including Tumor markers, Thyroid Stimulating Hormone, and free T4 levels. Thus, till she recovered from covid -19, she was discharged, so the surgery was postponed and she was readmitted after 3 week. Laparotomy and subsequent gastrostomy were performed to extract a large hairy compact 17.5 × 12.2 × 5 cm mass from the stomach and duodenum. The post-operative recovery was smooth, and she was able to eat on the 3rd post-operatively and was discharged on the day 4. After 2 weeks, she was seen in the outpatient clinic, was doing well and the wound was clean and healed. Her mother was advised to continue the psychiatric follow- up with a related planned therapeutic regimen to prevent recurrence this condition (Figures 1 & 2).
Discussion
Trichobezoar is a hairy deposition in the gastrointestinal tract [3]. It most usually occurs in the stomach, although it can spread to the duodenum and small bowel in a condition known as “Rapunzel Syndrome” [4]. Human hair resists digestion and peristalsis due to its enzyme-resistant characteristics and slippery surface. As a result, it collects between the stomach mucosal folds. With prolonged swallowing of hair, it becomes impacted with food, mucus, and air, producing a cemented mass known as trichobezoar [5]. The usual patient of such condition is a teenage girl with long hair [3], although this does not exclude out other age groups or sexes, as described by Sood, et al. [6, 7]. As shown by EL Castrillon Pena, et al. [8], it might occur from any type of maltreatment, resulting in nervous behaviors, emotional and psychological harm. Because trichobezoars are essentially a hair mass entangled with undigested food in the digestive tract, they are normally asymptomatic unless they reach a significant size, such as a huge trichobezoar reaching [6]. 200 grams reported by Hamidi, et al. [9] or induce blockage of the GIT. When symptomatic, the most prevalent symptom, accounting for more than 80% of instances, is palpable abdominal mass. Other symptoms are epigastric discomfort, which accounts for around 80% of cases, abdominal pain accounts for up to 70%. Approximately 65% of patients present with nausea and vomiting, 38% with malaise and weight loss, and 33% with diarrhea or constipation [10]. Trichobezoars can cause major consequences such peritonitis, gastric or duodenal perforation, acute pancreatitis, obstructive jaundice, subphrenic abscess, gastrointestinal bleeding, fistulas, intussusception, mal absorption, and iron deficiency anemia if left untreated [5].
Imaging modalities aid in the diagnosis of a trichobezoar. According to Ripolles, et al. [11] ultrasound, while it may be the first line of treatment due to its accessibility and affordability, has many limitations, including diagnosing a bezoar located far from the surface of the abdomen, diagnosing multiple bezoars due to the impossibility of viewing the entire bowel loops, and distinguishing bezoars from ectopic lithiasis and/or fecal material. Furthermore, it has a low sensitivity in identifying stomach bezoars due to the fact that hair is extremely echogenic, as well as the existence of trapped air bubbles and other acoustic reflections [10]. Upper gastrointestinal endoscopy is useful because it can differentiate between different types of bezoars, which is important when deciding on a treatment strategy since phytobezoars, for example, can be softened by enzymatic disintegration. Trichobezoars, on the other hand, require an anterior gastrotomy [11]. In our case, an upper endoscope could not have removed such a large trichobezoar. A laparoscopic surgery would have been recommended solely for aesthetic reasons. Otherwise, it is ineffective since it is complicated, time-consuming, and adds to the difficulties of evaluating and palpating the whole intestine for the existence of further bezoars. Not to mention that it will predispose the patient to additional anesthetic difficulties [10]. In our patient, endoscopic interpretation of the bezoar was that it was finn, calcified, intertwined, and of sufficient size that fragmentation was impossible. Gastric trichobezoars can be easily extracted through a small gastrotomy; the duodenum and jejunum should be palpated carefully for hair balls that may have broken off from the primary mass. In the presence of an intestinal bezoar discovered at laparotomy, the prevalence of a concurrent gastric bezoar is 20%.
Conclusion
To conclude up, although trichobezoar is an uncommon occurrence in clinical practice, It is critical to suspect and diagnose trichobezoar as it is associated with various complications and significant mortality.
References
-
Lamanna A, Sidhu A, Foo J, Aly A (2018) A Case of Large Gastric Trichobezoar: Case Report and Review of Literature. Archives of Clinical and Medical Case Reports 2: 101-105.
-
Tiago S, Nuno M, Joao A, Carla V, Goncalo M, et al. (2012) Trichophagia and trichobezoar: case report. Clin Pract Epidemiol Ment Health 8: 43-45.
-
O’sullivan MJ, McGreal G, Walsh JG, Redmond HP (2001) Trichobezoar. J R Soc Med 94(2): 68- 70.
-
Gorter RR, Kneepkens CMF, Mattens ECJL, Aronson DC, Heij HA (2010) Management of trichobezoar: Case report and literature review. Pediatr Surg Int 26(5): 457- 463.
-
Lyons D (2019) Large gastric trichobezoar causing failure to thrive and iron deficiency anaemia in an adolescent girl: A case report emphasising the imaging findings and review of the literature. BJR Case Rep 5(2): 20180080.
-
Sood AK, Bahl L, Kaushal RK, V K Sharma, N Grover (2000) Childhood trichobezoar. Indian J Pediatr 67(5): 390-391.
-
Pace AM, Fearne C (2003) Trichobezoar in a 13-year- old male: A case report and review of literature. Malta Medical Journal 15(1): 39-40
-
Pena ELC, Moreno MFE, Torres JCB, Nino EEF (2019) Gastroduodenal Trichobezoar in school age: Case report. Arch Argent Pediatr 117(3): e284-e287.
-
Hamidi H, Muhammadi M, Saberi B, Sarwari MA, (2016) A rare clinic entity: Huge trichobezoar. International Journal of Surgery Case Reports 28: 127-130.
-
Basem B, Awad S, Al-Share M, Abu-Jeyyab M, Al-Asbahi H, et al. A Massive Gastric Trichobezoar in A Young Female, A Case Report. Clin Surg J 5(2): 60-65.
-
Ripolles T, Garcia-Aguayo J, Martinez MJ, Gil P (2001) Gastrointestinal bezoars: Sonographic and CT characteristics. AJR Am J Roentgenol 177(1): 65-69.
- Management of Gallbladder Perforations: A Review
- From The Mouth to the Gut: The Oral Microbiome's Role in Promoting Gastrointestinal Disease
- Case Report: Intraductal Papillary Mucinous Neoplasm (IPMN) Complicated by Portal Vein Plaquing and Biliary Obstruction Mimicking Pancreatic Metastatic Malignancy
- Management of Non-Cirrhotic Portal Hypertension during Pregnancy: A Review
- Effectiveness of Omeprazole versus Pantoprazole for Symptomatic Relief of Gastro-Esophageal Reflux Disease (GERD)/ Acid Peptic Disease (APD): A Real-World Evidence (RWE) Study
- Case of Splenic Infarction; A Rare Presentation of Complicated Enteric Fever in a Pediatric Patient