Development and Evaluation of a Meloxicam Topical Ointment for Localized Drug Delivery
The introduction of this research paper sheds light on the background and significance of employing topical drug delivery methods to enhance the localized effects of NSAIDs, such as meloxicam. The introductory section underscores the potential benefits of utilizing skin penetration enhancement techniques to augment the efficacy of the ointment. The materials and techniques section comprehensively outlines the constituents employed in the study, including meloxicam and excipients. Special attention is dedicated to ensuring the stability and compatibility of the formulation components, with thorough investigations into drug-excipient interactions. Following the formulation’s development, a meticulous characterization of the ointments is conducted, encompassing their physicochemical attributes and drug release profiles. Concurrently, in vitro skin permeation experiments elucidate meloxicam’s capability to permeate the skin and elicit its therapeutic effects. The resultant characterization data yield valuable insights into the physical characteristics of the ointments. In conclusion, this thesis study substantially advances our comprehension of meloxicam topical ointment formulation development and evaluation for localized drug delivery. The findings gleaned from this study provide invaluable insights into the feasibility and effectiveness of employing a meloxicam-infused ointment. Such an approach holds the promise of offering a compelling alternative to conventional systemic administration, mitigating systemic side effects, and concurrently maximizing the localized therapeutic advantages of meloxicam.
Introduction
Meloxicam, classified as a nonsteroidal anti-inflammatory drug (NSAID), serves as a therapeutic intervention for osteoarthritis and rheumatoid arthritis in adults, along with juvenile rheumatoid arthritis in the pediatric population. It effectively alleviates diverse forms of pain emanating from musculoskeletal ailments, osteoarthritis, and rheumatoid arthritis [1]. Benefiting from an extended half-life surpassing that of many other NSAIDs, meloxicam presents itself as a favourable choice for individuals seeking the convenience of once-daily dosing. The versatility of meloxicam is reflected in its availability across oral, transdermal, and intravenous formulations. Distinguished as a selective COX-2 inhibitor, it is purportedly positioned to diminish the likelihood of adverse effects on the gastrointestinal tract. Nonetheless, it is crucial to note that this aspect remains a contentious topic, generating ongoing debates and discussions [2, 3].
Chemical Taxonomy
• Classification: This compound falls within the category of organic compounds referred to as benzothiazines. These compounds are characterized by the presence of a benzene ring fused to a thiazine ring, which consists of a six-membered structure comprising four carbon atoms, one nitrogen atom, and one sulfur atom.
- Kingdom: Organic compounds
- Super Class: Organoheterocyclic compounds
- Class: Benzothiazines
- Substituents: 2,5-disubstituted 1,3-thiazole / Alpha- amino acid or derivatives / Aromatic heteropolycyclic compound / Azacycle / Azole / Benzenoid / Benzothiazine / Carbonyl group/ Carboxamide group / Carboxylic acid derivative
- Molecular Framework: Aromatic heteropolycyclic compounds
- External Descriptors: monocarboxylic acid amide, 1,3-thiazole, benzothiazine Molecular Weight
- Average: 351.401
- Monoisotopic: 351.034747299
- Chemical Formula: C14H13N3O4S2
Indications
Meloxicam finds its clinical indication in the symptomatic management of arthritis and osteoarthritis. Furthermore, it serves as a treatment option for both the pauciarticular and polyarticular manifestations of Juvenile Rheumatoid Arthritis (JRA) in patients aged 2 years and older [4]. Meloxicam is occasionally employed for off-label purposes, encompassing the alleviation of dental or post- surgical pain. Beyond its established indications, meloxicam has garnered attention through investigations into its potential for managing neuropathic pain [1]. The combined administration of meloxicam and bupivacaine holds an indication for postsurgical analgesia among adult patients, extending for a period of up to 72 hours subsequent to surgical procedures involving the foot and ankle, small-to- medium open abdominal regions, as well as lower extremity total joint arthroplasty [5].
Pharmacodynamics
Prostaglandins are bioactive compounds that play a significant role in promoting and mediating the inflammatory response within the body [6]. This medication additionally demonstrates a selective impact on COX-2, potentially mitigating the gastrointestinal effects that could arise from its use [7].
In human studies, meloxicam has exhibited the capacity to lower the erythrocyte sedimentation rate (ESR) in individuals with rheumatoid arthritis. Moreover, it has demonstrated the ability to reduce not only ESR but also C-reactive protein (CRP) levels, alongside a decrease in aquaporin-1 expression [1]. In human subjects, meloxicam has exhibited the capability to diminish the erythrocyte sedimentation rate (ESR) among individuals with rheumatoid arthritis. Furthermore, it has displayed the potential to reduce both ESR and C-reactive protein (CRP) levels, along with a concurrent decrease in the expression of aquaporin-1 [4].
Due to its selective inhibition of COX-2, meloxicam is believed to induce comparatively lower gastrointestinal irritation in comparison to other NSAIDs. However, it’s important to note that meloxicam still entails a potential risk of instigating gastric inflammation, bleeding, and ulceration [3, 4].
Mechanism of Action
Meloxicam acts as an inhibitor of prostaglandin synthetase enzymes (both cylooxygenase 1 and 2), resulting in a reduction in the synthesis of prostaglandins. These molecules typically play a role in mediating the distressing symptoms associated with inflammation [6]. Prostaglandins have the capacity to sensitize neuronal pain receptors, and by impeding their synthesis, a cascade of analgesic and anti-inflammatory effects is induced. Meloxicam exhibits a preference for inhibiting COX-2, yet it also demonstrates certain activity against COX-1, resulting in a potential for gastrointestinal irritation [1, 4].
Pharmacokinetics
Absorption: In a specific pharmacokinetic investigation, the absolute bioavailability of oral capsules following a dose was determined to be 89%. The peak plasma concentration (Cmax) was achieved approximately 5 to 6 hours subsequent to the administration of a solitary dose, specifically following the first meal of the day. Notably, the Cmax exhibited a twofold increase when the drug was administered under fasting conditions. Remarkably, despite this observation, meloxicam retains the advantage of being suitable for ingestion without necessitating consideration of food intake, setting it apart from numerous other NSAIDs [1, 4].
Meloxicam, when formulated for instillation alongside bupivacaine, yielded diverse systemic outcomes subsequent to a single administration of varying strengths. In patients undergoing bunionectomy, an administration of 1.8 mg meloxicam led to a maximum plasma concentration (Cmax) of 26 ± 14 ng/mL, a median time to reach peak concentration (Tmax) of 18 hours, and an area under the concentration- time curve (AUC∞) of 2079 ± 1631 ng*h/mL.
Conversely, for a 9 mg dose administered during herniorrhaphy, the corresponding figures were 225 ± 96 ng/ mL for Cmax, a Tmax of 54 hours, and the AUC∞ was not specified. Lastly, in the context of total knee arthroplasty, a 12 mg dose yielded values of 275 ± 134 ng/mL for Cmax, a Tmax of 36 hours, and a substantially higher AUC∞ of 25,673 ± 17,666 ng*h/mL [5]. Volume of Distribution (VD): Meloxicam exhibits a volume of distribution within the range of 10 to 15 liters. Due to its substantial affinity for binding to albumin, it is anticipated to be distributed predominantly in highly perfused tissues, with notable emphasis on organs such as the liver and kidneys [1]. Following an oral dose, the concentrations of meloxicam in synovial fluid are estimated to reach approximately 40% to 50% of the concentrations observed in the plasma [4]. This medication is recognized to traverse the placental barrier in humans [8]. Plasma Protein Binding (PPB): Meloxicam is about 99.4% protein bound, primarily to albumin [1, 4, 7]. Metabolism: Meloxicam undergoes nearly complete metabolic transformation. The primary enzyme accountable for the metabolism of meloxicam is CYP2C9, [1, 9] with minor contributions from CYP3A4 [4]. Meloxicam generates four prominent metabolites, each devoid of determined activity. Approximately 60% of the administered dose undergoes metabolism to produce 5’- carboxy meloxicam, facilitated by hepatic cytochrome enzymes, through the oxidation of an intermediate metabolite known as 5’-hydroxymethylmeloxicam [9, 10]. It is plausible that two additional metabolites are generated through a process of peroxidation [4, 9].
Meloxicam → 5’-hydroxymethyl meloxicam → 5’-carboxy meloxicam Route of Elimination: The principal route of elimination for meloxicam is through metabolic processes. Its resultant metabolites are subsequently eliminated via both renal and fecal routes [7]. A minute fraction, specifically less than <0.25%, of the administered dose is excreted unchanged in the urine [4]. Approximately 1.6% of the parent drug is eliminated through fecal excretion [1]. Half-life (T1/2): The half-life of meloxicam is approximately 20 hours [7]. Its duration of action notably surpasses that of numerous other NSAIDs. As a result, there is no requisite for the utilization of slow-release formulations when dosing meloxicam [1]. When administered concurrently with bupivacaine for postsurgical analgesia, meloxicam displayed a median half- life ranging from 33 to 42 hours, contingent upon the specific dose and site of application [5] Clearance: Following oral administration, the total clearance of meloxicam ranges from 0.42 to 0.48 L/h. [1, 7] As per the FDA label, the plasma clearance of meloxicam is documented within the range of 7 to 9 mL/min. Notably, adjustments in dosing are unnecessary for individuals with mild to moderate renal or hepatic impairment. However, it’s important to acknowledge that the utilization of meloxicam among patients with severe renal or hepatic impairment remains unexamined. In alignment with the FDA prescribing information, it is advised against under such circumstances [4]. Adverse Effects: The utilization of meloxicam carries the potential for gastrointestinal toxicity and bleeding, as well as the occurrence of headaches, rash, and the presence of very dark or black stool, which serves as an indication of intestinal bleeding. It’s important to note that meloxicam exhibits a comparatively lower incidence of gastrointestinal side effects when compared to diclofenac [11], and perhaps all other NSAIDs which are not COX-2 selective.
In October 2020, the U.S. Food and Drug Administration (FDA) required the drug label to be updated for all nonsteroidal anti-inflammatory medications to describe the risk of kidney problems in unborn babies that result in low amniotic fluid. They recommend avoiding NSAIDs in pregnant women at 20 weeks or later in pregnancy [12, 13].
- Cardiovascular: Similar to other NSAIDs, the utilization of meloxicam is linked to an elevated risk of cardiovascular events, including incidents such as heart attacks and strokes [14]. While meloxicam does inhibit the formation of thromboxane A, it seems to achieve this effect at levels that do not significantly interfere with platelet function [15, 16]. In a comprehensive analysis that pooled data from various randomized, controlled studies spanning meloxicam therapy for a duration of up to 60 days, noteworthy findings emerged. Meloxicam showcased a statistically significant decrease in the occurrence of thromboembolic complications compared to the NSAID diclofenac, with rates of 0.2% and 0.8%, respectively. However, when juxtaposed with naproxen and piroxicam, meloxicam exhibited a comparable incidence of thromboembolic events [17]. Individuals with pre-existing conditions such as hypertension, elevated cholesterol levels, or diabetes are particularly vulnerable to experiencing cardiovascular side effects. Moreover, those with a family history of heart disease, heart attack, or stroke are advised to inform their attending physician, as the potential for severe cardiovascular side effects is noteworthy and warrants significant attention [18].
- Gastrointestinal: NSAIDs contribute to and escalate the likelihood of encountering severe gastrointestinal adverse events, encompassing issues like bleeding, ulceration, and perforation within the stomach or intestines, which can culminate in fatal outcomes. Elderly patients, in particular, face an elevated risk of experiencing these grave gastrointestinal events [19]. Toxicity: The oral LD50 in rats is 98 mg/kg [20]. An overdose of meloxicam can manifest through various signs and symptoms, including shallow breathing, seizures, diminished urine output, gastrointestinal irritation, nausea, vomiting, gastrointestinal bleeding, as well as the presence of black, tarry stools [21]. In the event of an overdose, the recommended approach involves providing supportive treatment while also They classified as given in Table No. 1 considering the removal of gastrointestinal contents. Notably, cholestyramine has demonstrated the capacity to augment the elimination of meloxicam and could be considered as a potential intervention [20]. Specific populations (Geriatrics): The utilization of meloxicam is cautioned against in individuals with peptic ulcer disease or an elevated risk of gastrointestinal bleeding. This pertains particularly to those aged 75 years and above, as well as those concurrently taking medications linked to an increased bleeding risk. It’s worth noting that adverse events related to meloxicam have been observed to be contingent upon the dosage and duration of treatment [22].
Experimental/ Methodology
The Meloxicam having 98% of purity was purchased from the online manufacturer and seller, having the info as following
- ID: CH-RDDFP91
- CAS Number: 71125-38-7
- Sub Category: Active Pharmaceutical Ingredients (API) Purity Percentage: 98%
- Country: India City: Mumbai
Physicochemical Properties of API (Meloxicam)
- IUPAC nomenclature: 4-hydroxy-2-methyl-N-(5- methyl-1,3-thiazol-2-yl)-1,1-dioxo-1λ6,2- benzothiazine- 3-carboxamide
- Classification: NSAID & Oxicames
| S No. | Physical & Chemical Properties | |
|---|---|---|
| 1 | Molecular weight | 351.4 g/mol |
| 2 | Physical appearance | Pastel yellow solid |
| 3 | Melting point | 254oC |
| 4 | Solubility | Very slightly soluble in methanol; Freely soluble in strong acid and bases; practically insoluble in water |
| 5 | Octanol/water partition, coefficient | 1.9 |
| 6 | Presence of ring | Benzothiazine, thiazole |
| 7 | Number of chiral centers | Not present |
Table 1: g- gram mol- mole, 0C- Degree Celcius.
• Mechanism of Action: Meloxicam operates through selective inhibition of the COX-2 enzyme, leading to a reduction in prostaglandin synthesis. This mechanism endows it with anti-inflammatory and analgesic properties. While meloxicam does exert minimal effects on COX-1, which can trigger gastrointestinal irritation and other side effects, its primary action on COX-2 is pivotal to its therapeutic profile.
- Structure Activity Relationship: General SAR for Oxicams can be summarized as follows:
- Substitution on the nitrogen atom of the thiazine ring gives optimum activity.
- Substitution on the caboxamide with aryl group gives compounds with greater activity than when substituents are alkyl groups.
- N-heterocyclic compounds are more acidic than N-aryl
carboxamides.
- Primary carboxamides are more potent than secondary carboxamides.
- M-substituted derivatives are more potent than p-substituted derivatives.
- Maximum activity is found with m-Cl substituent in the aryl series.
- Substitution on the carboxamide Nitrogen with heteroaryl group gives compound with seven fold greater anti-inflammatory activity than the aryl group substitution [23].
Method of Synthesis
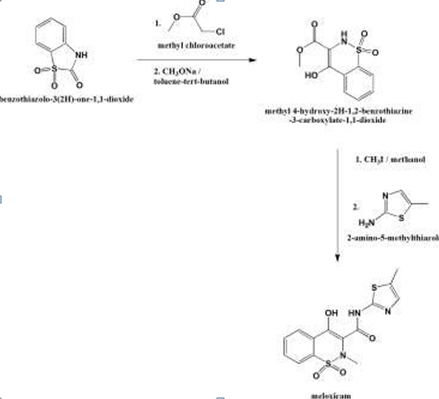
- Reaction of benzothiazolo-3-(2H)-one-1,1-dioxide with methyl chloroacetate to produce methyl-2(3H)-acetate derivative.
- Isomerization with sodium methoxide in toluene-tert- butanol to give methyl-4- hydroxy-2H-1,2-benzothiazine- 3-carboxylate-1,1-dioxide.
- Methylation with methyl iodide in methanol to produce 2-methylcompound.
- Treatment with 2-amino-5-methylthiazole in xylene to get meloxicam [24].
Pre-Formulation Studies
Physical Characteristics: The organoleptic properties of the meloxicam Active Pharmaceutical Ingredient (API) were assessed, encompassing attributes such as color, odor, and texture. Solubility Studies: Solubility studies played a pivotal role in guiding the choice of excipients for the formulation. Qualitative determination of meloxicam’s solubility was conducted in various solvents, including liquid paraffin, propylene glycol, span 20, tween 20, isopropyl alcohol, and water.
For each solvent, approximately 20 mg of meloxicam was individually added to 20 mL of the chosen solvent within 50 mL volumetric flasks. This procedure was performed to assess the solubility characteristics of meloxicam in each specific solvent.
Compatibility between Meloxicam and the Proposed Excipients: Upon analyzing the acquired FTIR spectra of the binary mixtures, no discernible alterations or chemical interactions between the meloxicam API and each individual excipient were detected. The prominent peaks evident in the meloxicam API spectrum remained consistent within the spectra of the binary mixtures. Any slight modifications observed in the spectra were attributed to the overlapping of the API and corresponding excipient peaks.
This analysis suggests a lack of interaction between the drug and excipient, signifying their compatibility in terms of physicochemical attributes.
Authentication of Meloxicam
- Experimental: Shimadzu UV-1800 with 1cm matched quartz cells was used for the spectra measurements. All chemicals employed in the study were of analytical reagent grade, ensuring a high level of purity. Furthermore, all reagents were meticulously prepared using distilled water, contributing to the accuracy and reliability of the experimental procedures.
- Assay Procedure: A stock solution of meloxicam was prepared by accurately weighing 100 mg of meloxicam and transferring it into a previously calibrated 100 ml volumetric flask. The weighed meloxicam was then dissolved in 40 ml of solvent through shaking for a duration of 10 minutes. The volume was subsequently brought up to 100 ml with 0.1N NaOH, resulting in a final concentration of 1 mg/ml (referred to as Solution A).
From Solution A, a 10 ml aliquot was withdrawn, and this aliquot was further diluted to a final volume of 100 ml using 0.1N NaOH solution. This subsequent dilution led to the creation of a solution with a concentration of 100 µg/ml (designated as Solution B).
From Solution B, aliquots of 1.0 ml, 2.0 ml, 3.0 ml, 4.0 ml, and 5.0 ml were pipetted into separate 10 ml volumetric flasks that had been previously calibrated. These aliquots were then diluted to a final volume of 10 ml using 0.1N NaOH solution. This process resulted in the creation of solutions with concentrations of 10 µg/ml, 20 µg/ml, 30 µg/ml, 40 µg/ ml, and 50 µg/ml, respectively.
To assess the absorbance of these solutions, measurements were taken at a wavelength of 269 nm using a UV Spectrophotometer. The absorbance readings were obtained by comparing the solutions against a blank solution composed of 0.1N NaOH. This procedure enabled the determination of the concentration-dependent absorbance of meloxicam at the specified wavelength [25, 26].
• Observations i. The spectrum of Meloxicam API was as follows Fig. 3
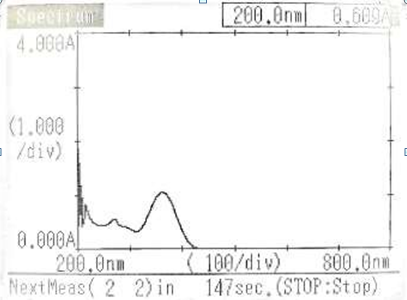
ii. The absorbance shown by Meloxicam is as Table 2 follows.
| λ (nm) | Absorbance (Abs) |
| 470 | -0.001 |
| 362 | 1.049 |
| 270 | 0.558 |
| 247 | 0.436 |
Table 3: Nm- Nanometer.
The standard UV absorbance for Meloxicam is typically observed at 354 nm. However, in the case of our API, it exhibited a peak at 362.00 nm. This variance is attributed to internal impurities present in the specific sample.
Formulation of Meloxicam Ointment
The formulation procedure is followed as per Table 3. We made the two batches varying in concentration of the API i.e. Meloxicam.
| Ingredient | Batches | |
|---|---|---|
| F1 | F2 | |
| Meloxicam | 0.1 gm | 0.2 gm |
| Emulsifying wax | 6 gm | 6 gm |
| White soft paraffin | 10 gm | 10 gm |
| Liquid paraffin | 4 gm (4.65 gm) | 4 gm (4.65 gm) |
| Rose Oil | 0.06 ml | 0.06 ml |
| Amaranth | --- | 0.02 gm |
| Saffron | 0.02 gm | --- |
Table 2: We made the two batches varying in concentration of the API i.e. Meloxicam.
Step 1: Preparation of Emulsifying Ointment Base The preparation process followed a specific formula. Initially, a quantity of 6 g of emulsifying wax was weighed and placed in a porcelain dish. The dish was then heated in a water-bath until the wax melted at a temperature of 70°C. Subsequently, 10 g of white soft paraffin was introduced into the porcelain dish and allowed to melt as well.
Following this, 4.65 ml of liquid paraffin was meticulously incorporated into the mixture within the porcelain dish. The dish containing the mixture was then carefully taken out of the water- bath, and the contents were left to solidify. During this stage, continuous stirring was employed to ensure the attainment of a homogenous mixture. This process resulted in the desired final product as per the designated formula.
Step 2: Formulation of Ointment
- The specific quantity of Meloxicam as per given in above table is weighed. Ointment base is also measured approximately 10 gm.
- The mixing of the Meloxicam and ointment base is performed by the levigation method.
- After the proper mixing of Meloxicam and ointment base colouring agent i.e. Amaranth for one batch and saffron for other batch is added.
- After colouring agent flavouring agent is added i.e. rose oil as per given quantity [27].
Evaluation of Ointment
Organoleptic Parameters: The evaluation of the creams encompassed a comprehensive assessment that took into account their organoleptic attributes, including appearance, texture, and odor. Furthermore, an analysis of the creams’ physicochemical properties was conducted to ensure a thorough evaluation of their overall quality. Homogeneity: The formulated ointments underwent an evaluation process to determine their homogeneity, which was assessed through both visual inspection and tactile examination. To assess homogeneity and texture, a small amount of the formulated creams and gels were pressed between the thumb and index finger. This allowed for the assessment of the consistency of the formulations as well as the detection of any coarse particles. The overall texture and homogeneity of the formulations were inferred based on these observations.
After Feel: Emolliency and greasiness of the ointments were assessed by applying a finger-tip unit of the ointment onto the skin. This evaluation aimed to gauge the ointment’s ability to provide a soothing and moisturizing effect (emolliency) as well as its tendency to impart a greasy sensation on the skin.
Determination of PH: The ointments were transferred into a beaker for the purpose of conducting a pH test. A pH meter was employed to measure the pH of the ointments, and the recorded pH readings were documented for further analysis.
Spreadability: Spreadability of the formulation was determined using a modified apparatus based on Multimer’s suggestion. The apparatus consists of a wooden block with a pulley attached at one end, along with a fixed glass slide on the block. To initiate the test, an excess of ointment (3 g) was placed on a ground plate.
The ointment was then layered between this ground plate and another glass plate, which shared the dimensions of the fixed ground plate and was equipped with a hook. Applying uniform pressure, a 1 kg weight was positioned atop the two plates for duration of 5 minutes. This step served to eliminate air and establish a consistent film of ointment between the plates. Any surplus ointment at the edges was subsequently removed.
Following the previous steps, the top plate was subjected to a poll of 240 g. A spring connected to the hook facilitated this process. The time taken by the top plate to travel a distance of 10 cm was recorded. A shorter time interval denoted enhanced spreadability of the ointment. This methodology provided insights into the ointment’s ability to spread effectively.
Spreadability was calculated using the following formula $$ S = M \times \frac {L}{T} $$ Where, S = Spreadability M = Weight in the pan (tied to the upper slide) L = Length moved by the glass slide and T = Time (in seconds) taken to separate the slide completely each other.
Loss on Drying: Loss on drying was determined by placing ointment in petri dish on water bath and dried for 105ᴼC Extrudability: A straightforward methodology was employed for this investigation. Once the ointments had solidified within the containers, they were transferred into collapsible tubes. The study focused on evaluating the extrudability of various ointment formulations.
To assess extrudability, the weight in grams necessary to extrude a 0.5 cm ribbon of ointment over a span of 10 seconds was measured. This measurement provided insights into the ease with which the ointment could be dispensed from the tubes, offering a valuable indication of the formulation’s practical application and user-friendliness.
Irritancy Study: During this assessment, the ointment underwent a comprehensive examination encompassing various attributes. These included observations related to its color, odor, texture, and overall state. The test procedure involved marking a designated area (1 cm) on the dorsal surface of the left hand. Subsequently, the ointment was applied to this marked area, and the time of application was recorded.
Following the application, the area was closely monitored for any indications of irritancy, such as erythema (redness) or oedema (swelling), over duration of up to 24 hours. Any observed reactions were meticulously documented and reported. This testing process offered insights into the potential irritant effects of the ointment on the skin.
Results
| S No | Parameter | Observation | ||
|---|---|---|---|---|
| S No | Parameter | F1 | F2 | |
| 1 | Colour | Flamingo | Cerise | |
| 2 | Odour | Rose | Rose | |
| 3 | Consistency | Smooth | Smooth | |
| 4 | pH | 6.7 ±0.5 | 6.8 ±0.5 | |
| 5 | Spreadability | 9.7 | 9.6 | |
| 6 | Extrudability | 15 gm | 15 gm | |
| 7 | Irritancy | Non-irritant | Non-irritant | |
| 8 | Stability | Stable | Stable |
Table 4: Gm- gram, pH- Acidity and basicity.
The table above illustrates that both formulations exhibit a pH within the range of 6.7-6.8. This pH range signifies that these topical formulations are well-suited for application on the skin surface. Notably, the ointment demonstrates favorable spreadability, contributing to minimized friction and the establishment of a suitable layer on the skin.
Stability testing revealed that the ointment remains stable within the temperature range of 25- 35°C, affirming the satisfactory stability conditions. The inclusion of rose oil imparts a pleasant odor reminiscent of roses, enhancing the user experience. Additionally, the incorporation of colorants Amaranth and Saffron contributes to the ointment’s distinctive pinkish hue, providing it with its characteristic color. These attributes collectively contribute to the formulation’s suitability for skin application.
Discussion
Opting for the skin as a target for drug delivery offers a range of advantages over oral administration. Notably, this approach serves to circumvent the initial hepatic metabolism that affects drugs with limited oral bioavailability. Furthermore, employing the skin as a delivery site presents distinct advantages over hypodermic injections. Injections often lead to discomfort, generate potentially hazardous medical waste, and elevate the likelihood of disease transmission through needle reuse. This highlights the skin as a safer, more efficient, and patient-friendly Avenue for drug delivery [28]. Furthermore, skin-based delivery systems offer a non-invasive approach that can be conveniently self-administered by individuals. This user- friendly characteristic adds to their appeal. These systems are capable of facilitating sustained and controlled drug release, which in turn leads to a consistent plasma profile. This controlled release mechanism contributes to the mitigation of systemic side effects, thereby enhancing the safety and efficacy of drug delivery via the skin [29]. Despite the advantages, the development of approved drugs targeting the skin remains relatively limited. This constraint can be attributed to the formidable barrier properties exhibited by the outermost layer of the skin, known as the stratum corneum (SC). The SC serves as the primary impediment to the penetration of drugs. Consequently, overcoming the formidable barrier posed by the stratum corneum has posed a challenge in expanding the range of drugs that can effectively target the skin for delivery [30].
Indeed, the delivery of topical agents to and through the skin presents challenges owing to the specific physicochemical characteristics of these agents. The properties of topicals often do not align with the optimal physicochemical attributes desirable for efficient skin delivery. Ideal drug candidates for skin delivery are characterized by specific physicochemical properties that enable effective penetration through the skin. In this context, the physicochemical properties of topical drugs, such as those characterized by zwitterionic behavior with dual pKa values (pKal = 1.09, pKa2 = 4.18), pose complexities for successful skin delivery. The comparison of these properties against the requirements for effective skin delivery highlights the potential obstacles and intricacies involved in developing formulations that can achieve efficient transdermal delivery of such drugs [31]. Indeed, many zwitterionic drugs exhibit certain challenging physicochemical properties. These properties include relatively high melting points, low solubilities, and poor lipophilicities. These characteristics can complicate the formulation and delivery of such drugs, especially when attempting to achieve effective transdermal delivery through the skin. The combination of these factors can influence the overall feasibility and success of developing transdermal delivery systems for zwitterionic drugs.
The continuous evolution and diversification of both conventional and novel formulation approaches for enhancing skin permeation hold the potential to significantly broaden the horizon of drug administration through the skin. This expansion of strategies makes it feasible to target a wider array of drugs that may not conform to the ideal prerequisites for successful skin permeation. As a result, the development of innovative approaches grounded in formulation strategies can pave the way for effective delivery of topical agents through the skin. This avenue of research and development offers the promise of overcoming challenges and advancing the field of transdermal drug delivery.
The field of transdermal drug delivery has witnessed a growing fascination with the advancement of physical enhancement methods. These techniques aim to overcome the formidable barrier presented by the skin by employing external energy sources. Among these approaches, iontophoresis and electroporation have garnered substantial attention, with their applications even reaching commercialization stages. Iontophoresis, for instance, has demonstrated its potential by achieving a remarkable 19.56-fold increase in the cumulative amount of topical salts permeating over a 12-hour period when compared to passive controls. Additionally, the combination of iontophoresis with electroporation has yielded significant enhancements in the in vitro permeation of topical salts. These findings underscore the promising impact of these techniques in enhancing transdermal drug delivery, which holds considerable potential for advancing drug administration strategies [32].
The administration of nonsteroidal anti-inflammatory drugs (NSAIDs) is consistently associated with the occurrence of side effects, notably encompassing gastrointestinal, cardiovascular, and renal adverse events. The manifestation of these adverse effects is often influenced by factors including dosage, treatment duration, and the patient’s age. These considerations underscore the importance of cautious and individualized use of NSAIDs to mitigate the risk of these potential complications [32].
Given the well-documented side effects associated with systemic NSAID administration, there exists a compelling conjecture that the transdermal delivery of NSAIDs holds significant potential in the market. This approach offers the advantage of potentially minimizing the systemic exposure and associated adverse events. Furthermore, the compatibility of meloxicam (MX) with the skin appears to be favorable when compared to other NSAIDs like piroxicam, ketoprofen, indomethacin, diclofenac, and ibuprofen. This distinction in compatibility further supports the viability of meloxicam-based transdermal formulations, potentially positioning them as a more skin-friendly and safer option for localized drug delivery [33].
Conclusion
This research serves as a comprehensive guide for the utilization of Meloxicam in the treatment of Rheumatoid Arthritis and Joint pain, with a focus on achieving minimal to no side effects. The study presents a successful formulation approach for creating a Meloxicam NSAID ointment, which holds promise as an effective treatment option for these conditions. Incorporating carefully chosen colorants has not only enhanced the aesthetic appeal of the ointment but also exhibited no adverse impact on its stability. The investigation also offers valuable insights into the optimal composition of ingredients, influencing both the physical properties of the ointment formulations and their acceptance by consumers. The evaluation of the prepared ointment formulations under various parameters yielded results that fell well within the prescribed limits, ensuring their quality and efficacy. Notably, the pH levels of all formulations indicated an alkaline nature. Furthermore, the formulations displayed pseudo- plastic flow behaviour based on viscosity measurements. The ointments containing Meloxicam as the active ingredient exhibited commendable attributes such as strength, viscosity, and spreadability. Importantly, these formulations demonstrated no signs of skin irritation upon application. Additionally, the incorporation of paraben showcased both economic and functional benefits, leading to a reduction in the required quantity of hard wax compared to beeswax. The significance of this work extends to its potential to inspire further research and instill confidence in the utilization of natural active ingredients in the pharmaceutical industry. Overall, this research contributes to advancing pharmaceutical science and fostering greater exploration of innovative formulations for improved patient care.
References
-
Bekker A, Kloepping C, Collingwood S (2018) Meloxicam in the management of post- operative pain: Narrative review. J Anaesthesiol Clin Pharmacol 34(4): 450-457.
-
Katz JA (2013) COX-2 inhibition: what we learned--a controversial update on safety data. Pain Med 14(1): S29-S34.
-
Seddik H, Rabhi M (2013) Meloxicam-induced colitis revealed by acute abdominal pain. Ann Pharm Fr 71(2): 119-22.
-
FDA approved products: Mobic (meloxicam) oral tablets.
-
FDA Approved Drug Products: ZYNRELEF (bupivacaine and meloxicam) extended-release solution for injection.
-
Ricciotti E, Fitz Gerald GA (2011) Prostaglandins and inflammation. Arterioscler Thromb Vasc Biol. 31(5): 986-1000.
-
Turck D, Roth W, Busch U (1996) A review of the clinical pharmacokinetics of meloxicam. Br J Rheumatol 1: 13- 16.
-
Carl PW, Clifford M (2019) Drugs for Pregnant and Lactating Women. In: 3rd (Edn.), Elsevier.
-
Chesne C, Guyomard C, Guillouzo A, Schmid J, Ludwig E, et al. (1998) Metabolism of Meloxicam in human liver involves cytochromes P4502C9 and 3A4. Xenobiotica 28(1): 1-13.
-
Prasad GS, Srisailam K, Sashidhar RB (2016) Metabolic inhibition of meloxicam by specific CYP2C9 inhibitors in Cunninghamella blakesleeana NCIM 687: in silico and in vitro studies. Springerplus 5: 166.
-
Hawkey C, Kahan A, Steinbruck K, Alegre C, Baumelou E, et al. (1998) Gastrointestinal tolerability of meloxicam compared to diclofenac in osteoarthritis patients. International MELISSA Study Group. Meloxicam Large- scale International Study Safety Assessment. Br J Rheumatol 37(9): 937-945.
-
(2020) FDA Warns that Using a Type of Pain and Fever Medication in Second Half of Pregnancy Could Lead to Complications. U.S. Food and Drug Administration.
-
(2017) NSAIDs may cause rare kidney problems in unborn babies. U.S. Food and Drug Administration.
-
Stamm O, Latscha U, Janecek P, Campana A (1976) Development of a special electrode for continuous subcutaneous pH measurement in the infant scalp. Am J Obstet Gynecol 124(2): 193-195.
-
Zeidan AZ, Al Sayed B, Bargaoui N, Djebbar M, Djennane M, et al. (2013) A review of the efficacy, safety, and cost-effectiveness of COX-2 inhibitors for Africa and the Middle East region. Pain Practice 13(4): 316-331.
-
Gates BJ, Nguyen TT, Setter SM, Davies NM (2005) Meloxicam: a reappraisal of pharmacokinetics, efficacy and safety. Expert Opin Pharmacother 6(12): 2117- 2140.
-
Singh G, Lanes S, Triadafilopoulos G (2004) Risk of serious upper gastrointestinal and cardiovascular thromboembolic complications with meloxicam. Am J Med 117(2): 100-106.
-
(2014) Meloxicam. MedlinePlus.
-
(2010) Meloxicam official FDA information, side effects, and uses.
-
Medsafe NZ (2023) Mobictab (meloxicam) oral tablets. Data Sheet.
-
American College of Cardiology: Meloxicam, CardioSmart.
-
(2019) American Geriatrics Society 2019 Updated AGS Beers Criteria® for Potentially Inappropriate Medication Use in Older Adults. J Am Geriatr Soc 67(4): 674-694.
-
Lemke TL, Williams DA, Roche VF, Zito SW (2013) FOYE. S Principles of Medicinal Chemistry. In: 7th (Edn.), Lippincott Williams, USA.
-
(2003) Ullmann’s Encyclopedia of Industrial Chemistry. In: 6th (Edn.), Federal Republic of Germany: Wiley-VCH Verlag GmbH & Co 1: V3-51.
-
Reddy MN, Murthy TK, Rajita K, Shankar DG (2003) New spectrophotometric methods for the determination of meloxicam. Indian J Pharm Sci 65(6): 655-658.
-
Seedher N, Garg A, Bhatia S (2003) Spectrophotometric method for estimation of some COX-2 inhibitors in pure form and in pharmaceutical formulations. Indian J Pharm Sci 65(7): 685-688.
-
Sinodukoo EO, Christiana OA, Chisom CO (2020) Formulation and evaluation of antimicrobial herbal creams from aqueous extract of Moringa Oleifera Lam seeds. Nigerian Journal of Science and Environment 18(1).
-
Miller MA, Pisani E (1999) The cost of unsafe injections. Bull World Health Organ 77(10): 808-811
-
Rausnitz MR, Langer R (2008) Transdermal drug delivery. Nat Biotechnol 26(11): 1261-1268.
-
Wiechers JW (1989) The barrier function of the skin in relation to percutaneous absorption of drugs. Pharm Weekbl Sci 11(6): 185-198.
-
Luger P, Daneck K, Engel W, Gunter T, Klaus W (1996) Structure and physicochemical properties of meloxicam, a new NSAID. European Journal of Pharmaceutical Sciences 4(3): 175-187.
-
ltman RD, Barthel HR (2011) Topical therapies for osteoarthritis. Drugs 71(10): 1259-1279.
-
Stei P, Kruss B, Wiegleb J, Trach V (1996) Local tissue tolerability of meloxicam, a new NSAID: indications for parenteral, dermal and mucosal administration. Br J Rheumatol 35(1): 44-50.
- Superposition of Cryo-EM and AlphaFold Predictions of Dengue Antigen-Antibody Complexes
- Jugular-Applied Coherent Low-Level Laser Therapy Enhances Systemic Mitochondrial Metabolic Function and Antioxidant Response
- Role of OMC32 Polypeptide in Acrosin-Mediated Exocytosis during the Bovine Sperm Acrosome Reaction
- Association of Galectin-3 but not Laminin in Tamoxifen-Induced Growth Suppression in Breast Cancer MCF-7 Cells
- Effect of Different Wavelengths of Light on the Rate of Photosynthesis
- Nutritional, Therapeutic, and Environmental Effect of Oyster Mushrooms: An Editorial