Analytical Methods of Compounds in Biological Specimens: Applications in Forensic Toxicology
Toxicology is defined as the study of adverse effects of drugs, chemicals and any other xenobiotics on biological systems. Forensic toxicology is the application of toxicology cases and issues where the results are likely to be used in court. It is a modern science combining disciplines such as analytical chemistry, biology, pharmacology and clinical chemistry to help medical or legal investigations of death, poisoning, and drug use. Most widely, forensic toxicology is applied in postmortem toxicology, human performance, doping control and work place drug testing. The analytical methods and techniques are basically summarized in two categories of forensic tests used to analyze drugs and other unknown substances: Presumptive tests (such as color tests) which give only an indication of which type of substance is present, but they can't specifically identify the substance; Confirmatory tests that are more specific and can determine with precision the identity of the substance. Confirmatory tests include chromatography techniques such as gas chromatography (GC)/mass spectrometry, high performance liquid chromatography (HPLC). In this review, the drugs commonly investigated for forensic purposes, the specimens and samplingare reviewed. The analytical methods and techniques are described enough in order to give a guidance for identifying both qualitatively and quantitatively unknown powders, liquids and pills that may be illicit drugs
Introduction
Forensic toxicology is the study and practice of the application of toxicology to the purposes of the law. It is a modern science combining disciplines such as analytical chemistry, biology, pharmacology and clinical chemistry to help medical or legal investigations of death, poisoning, and drug use [1]. It is not only encompasses the identification or quantification of drugs, but also the meaning of those drugs in the setting of death: postmortem toxicology, human performance, doping control and work place drug testing [2]. Interpretation of forensic toxicology results depend on multiple of factors among them the time since death or intoxication, the possibility of tolerance, the presence or absence of other drugs that may lead to interactions, toxicity even if all of the drugs present are within therapeutic range [3].The half time and volume of distribution when known may help in the interpretation of values obtained. According (Pounder 1990) [4] the volume distribution more than 3L/kg may show significant redistribution, and samples from sites other than peripheral blood may require more scrutiny. Most postmortem cases contain a plethora of specimens available for toxicological analysis, but it is important to know which specimens are most useful for yielding drug concentrations that are practical for interpretation [5]. Not all specimens may be available in all cases. For instance, decomposed bodies may no longer have blood, yet may have vitreous, urine, and tissue. The purpose of this paper review is to assist forensic professionals in gathering the modern technical methods for screening and confirmatory test for supporting evidences when forensic investigations are required.
Common Drugs of Abuse
Most forensic toxicology methods for drug analysis offer a screening test to determine the presence or absence of the majority of significant drugs described in (Table 1).
| Class | Some common effects | Examples | References | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Cannabinoids | Euphoria, altered sensory perception, sleepiness, disrupted coordination | Marijuana, Hashish | (Szabo, 2005; Pertwee, 2005) [6,7] | ||||||||
| Narcotics | General sense of wellbeing, drowsiness, inability to concentrate | Opium, heroin, morphine, methadone, oxycodone | (Health, 2009; Anglin, 1988) [8,9] | ||||||||
| Stimulants | Euphoria, exhilaration, wakefulness, agitation, hostility, hallucinations | Amphetamines, methamphetamines, cocaine | (Police, 1992) [10] | ||||||||
| Depressants | Sleepiness, amnesia, impaired judgement,, confusion, slurred speech, loss of motor coordination | Alcohol, barbiturates, benzodiazepines, GHB, Rohypnol | (Police, 1992) [10] | ||||||||
| Hallucinogens | Altered perception of mood, mild to severe hallucinations | LSD, MDMA, PCP, Ketamine, peyote, mushrooms(Psilocybin) | (McCall, 1986; Kyzar, 2012) [11,12] | ||||||||
| Synthetic drugs | Agitation, irritability, impaired perception of reality, reduced motor control, inability to think clearly | Bath salts( Cathinones), DXM, salivia | (Haynes, 2015) [13] | ||||||||
| Steroids | Mood swings, hostility, impaired judgement, aggression | Human growth steroids, testosterone | (Hartgens, 2004) [14] | ||||||||
| Inhalants | Loss of inhibition, intoxication, slurred speech, decreased coordination, euphoria, disorientation | Ether, nitrous Oxide, butane, cyclohexyl nitrite, amyl nitrite | (Dutta, 2017; Hassan, 2017) [15,16] |
Table 1: Drugs of abuse and their common effects.
Types of Specimens and their Utility
In Guidelines, 2006 [17] it stated as following: The proper selection, collection and submission of specimens for toxicological analysis is of paramount importance if analytical results are to be accurate and their subsequent interpretation is to be scientifically sound and therefore useful in the adjudication of forensic case. Each specimen provides different information about time and extent of use and likelihood of impairment. Some of these specimens (e.g., urine and oral fluid) can even be analyzed with simple on-site, non-instrumented testing devices, as well as through standard laboratory methods [18]. A wide variety of body fluid specimens have been utilized for analysis for the presence of drugs of abuse. Urine has been and remains the most widely used body fluid specimen for routine testing for drugs of abuse, but several alternative specimens are establishing their place as suitable for drug testing [18]. The purpose of this section is to give a brief overview of the types of specimens available, the utility of the each specimen, and the collection criteria as mentioned by Suzuki, 2005 [19].
Blood: Blood is widely regarded as the specimen offering the best correlation between drug levels and likely dosing and likely concomitant pharmacological, cognitive, and psychomotor effects. There have been many controlled dosing studies examining blood levels of drugs and concomitant effects. The majority of data reported regarding the therapeutic and toxic concentrations of drugs was obtained from blood specimens [20]. Blood is a relatively easy sample to obtain and store. For postmortem studies, peripheral blood is more desirable than central blood as it is less affected by postmortem redistribution. It is usually recommended that femoral blood be obtained preferentially, followed by subclavian, heart and, lastly, cavity blood. Unfortunately, in cases of severe trauma or decomposition, blood may not be available. Urine: Urine is 95% water, with sodium chloride and urea in about equal amounts as the main dissolved substances, and with much smaller amounts of a wide variety of other constituents [21]. Urine is attractive as a specimen because it can be conveniently provided as a normal waste product in relatively large volumes. Typical urine production rates are about 1 mL/min during waking hours, so collection of a specimen of sufficient volume for both initial screening by immunoassay as well as any subsequent confirmation testing is generally not problematic. Furthermore, the large specimen volume allows the option of splitting the specimen into two portions at the time of collection for assurance of proper chain of custody and specimen integrity in the event of adversarial challenges to the test results. Drugs and their metabolites are reasonably stable in urine when specimens are refrigerated or frozen. As far as specimen handling is concerned, urine is generally not considered infectious unless visibly contaminated with blood. In most of guidelines of drugs testing, the urine is used to test five drugs of abuse: cannabinoids (marijuana), cocaine metabolites, opiates, amphetamines, and phencyclidine [22, 23]. In spite of the well-established place of urine as a specimen for drug testing, its use is not without any challenges: - One issue is the potential invasion of privacy involved in specimen collection. Most workplace and other drug- testing programs do not allow direct observation of specimen collection, except under special circumstances. It involves the privacy in specimen collection; - Without direct observation, the opportunity for specimen adulteration and substitution exists.
Oral fluid: Oral fluid is an exciting alternative matrix for monitoring drugs of abuse in workplace, clinical toxicology, criminal justice, and driving under the influence of drugs (DUID) programs [24]. Although saliva has been the commonly used term to describe fluid specimens from the oral cavity, this fluid, as collected by current simple swabbing or absorbent pad devices, is really a complex mixture of several different oral fluids, including saliva. Accordingly, the broader term oral fluid is preferred. Oral fluid represents a mixture of not only the saliva from the three oral salivary glands (parotid, submandibular, and submaxillary), but other oral fluids as well (e.g., gingival crevicular fluid) [25]. Oral fluid has been used for a wide variety of analytes, including steroids, hormones, enzymes, antibodies, DNA typing, therapeutic drugs, and drugs of abuse [26]. The mechanism by which drugs are found in saliva is passive diffusion, although there are examples of active secretion (e.g., lithium). The major factors affecting drug entry into saliva are lipid solubility and degree of ionization at saliva pH. Unfortunately, oral fluid has not proven very sensitive for detection of cannabis use, as it appears that cannabinoids are not secreted from the blood into oral fluid. Hair: Hair testing has gained interest because of its ability to provide a history of drug use. The advantage of the sample material hair in comparison to blood, urine, sweat, or oral fluid is the extended time window, allowing the retrospective detection of chronic consumption up to years. Hair specimens from ancient mummies have been demonstrated to contain cocaine. Several famous deceased persons have also had their hair analyzed for drug exposure [27]. Drugs have been demonstrated to remain in hair for extended periods of time, and even decades of years [28]. The simplest model proposed for drug incorporation into hair is the simple passive transfer [29, 30]. In this model chemicals move by passive diffusion from the bloodstream into the growing hair cells at the base of the follicle and then during subsequent keratogenesis they become tightly bound in the interior of the hair shaft. The incorporation is dependent on the drug concentration in blood, which depends on the ingested drug dose. The best collection site for hair is from the vertex posterior on the back of the head. It is important to label the hair with a rubber band, twist tie, or string to clearly differentiate the end that is closest to the scalp. Strands of hair, approximately 200mg should be cut as close to the scalp as possible and placed in aluminum foil, an envelope, or plastic collection tube [31]. Storage at ambient temperature is sufficient. Nails removed from the fingers or toes are stored in similar conditions to hair samples. The main issues facing hair testing is distinguishing environmental exposure/contamination of the hair from drug incorporation in the hair shaft from use or abuse. Sweat: Drugs of abuse and their metabolites have long been known to be excreted in sweat [32]. The criminal justice community has shown great interest in sweat-patch testing for drugs of abuse. The patch offers the primary advantage of constantly monitoring for any drug use over a period of approx. one week obviating the need for multiple urinalyses to effectively monitor for any drug use over that period. The development and patenting of a sweat patch collection device [33] in the 1990s has allowed for the ready detection of drug use over a period of about one week.
Tissue Specimens
Tissue samples are usually readily available in large quantities; however, interpretation of drug concentration can be difficult since data is not often available for comparison. Tissue concentrations may also be elevated in oral overdoses and chronically administered drugs. Following are some tissue specimens: Muscle: Muscle is a preferred tissue sample as research has shown very good correlation between drug concentrations found in muscle with those found in blood [34]. The distribution of drugs into muscle depends on a number of factors among them blood flow, the partition coefficient of the drug between blood and the muscle, the degree of ionization of the drug at the pH of plasma, the molecular size and the extent of tissue and plasma protein binding [35]. Liver: In most postmortem toxicology cases, a liver sample is usually the most valuable tissue specimen [33]. Liver has long been used as a secondary sample when blood is not available. Since most drugs and poisons are metabolized in the liver, both the parent compound and its metabolites may be present in high concentrations in this tissue. Additionally, quantitative analysis of a liver specimen may assist in differentiating acute overdoses from therapeutic use of drugs that have a narrow therapeutic index. To minimize the effect of drug diffusion from the small bowel and stomach on quantitative findings, the sample should be from deep within the right lobe of the liver. Approximately 25-50g of tissue should be collected [36]. Among published studies, liver probably has the most data available for comparison of postmortem drug concentrations [34]. Some drugs, such as tricyclic antidepressants, are sequestered in the liver, resulting in higher levels than in the blood. Liver concentrations may also be higher if the drug was taken orally or if it undergoes hepatic metabolism. In cases of hepatic metabolism, higher concentrations of the metabolites will often be seen in comparison to lower concentrations of the parent drug, which may indicate chronic use versus an acute overdose [37]. Kidney: Kidney specimens may be used as any other tissue specimens, although the utility of the kidney specimens is mainly in heavy-metal testing as metals often accumulate in the kidney [38]. Brain: Since the brain is the primary site of action of many drugs, it becomes a useful specimen particularly for lipophilic substances such as halogenated hydrocarbons, narcotics, and antidepressants [39]. While drug and poison concentrations may have significant variance in different regions of the brain, current data do not suggest that one portion should be collected over another. When collected, a minimum of 25g of unfixed brain should be provided. Lungs: Lung is a useful tissue specimen for inhaled toxins such as volatile compounds including the halogenated hydrocarbons. The lungs often contain high concentrations of drugs and poisons in cases of inhalation and intravenous exposure. The apex of either lung (25- 50g) is the best choice of specimen for STA [40, 41].Exhaled breath has also been developed as a possible specimen for drug testing based on the collection of aerosol particles originating from the lung fluid [42].
Other Specimens
A wide variety of additional body specimens have been analyzed for drugs of abuse. These are not widely used, but a few will be discussed briefly and for details, the reader is referred to (Jenkins, 2013) [43]. Meconium: Meconium is a newborn’s first stool. It is formed over the last trimester of pregnancy, and thus can represent exposure to drugs over 16–20 weeks prepartum. Meconium is collected from the neonate’s diaper and extracted with solvents. Breast milk: Drugs and alcohol have also been detected in mother’s breast milk, with implications for healthcare concerns about neonatal exposure. It has been demonstrated that alcohol is eliminated in breast milk, and that newborns can detect the flavor of alcohol in breast milk and actually suck harder but obtain less milk as a result of alcohol’s inhibition of prolactin secretion, thereby inhibiting milk release. More dramatically, methamphetamine and cocaine have been found in mother’s breast milk and linked to adverse neonatal health effects. Semen: Semen has been demonstrated to have measurable levels of drug after drug use. It is occasionally proposed as a basis to explain positive drug tests as a result of exposure to drugs through sexual relations. However, the absolute amount of drug present in semen is very low and could not account for significant exposure. Vitreous humor: Vitreous humor is the gel that fills the eye. It is obtained at autopsy and analyzed for drugs. Spleen: Spleen is often utilized as an alternative source for blood in cases of carbon monoxide poisoning. Adipose tissue: Fat is an excellent specimen for pesticide poisonings and volatile analysis. Stomach contents: Stomach contents are often collected in cases where an oral drug over dose is suspected. Concentrations of drugs in the stomach, however, do not accurately represent the concentration of the drug in the body. The presence of a drug in gastric material, even at elevated concentrations, may not indicate that the drug contributed to death. Stomach contents may be useful in specifying that the blood should be analyzed for a particular drug, which may have been overlooked or not seen without special testing.
Drugs Testing
Drug detection in the forensic context requires numerous analytical techniques. Depending on locally adopted standard procedures, different techniques are used for handling and screening samples for potential illicit substances [19]. Generally, in forensic toxicology, there are two types of tests: screening tests and confirmatory tests [44]. Samples are usually first screened for the presence of medications and/or intoxicating substances, then a more specific, confirmatory test is performed to determine the exact substance and, often, concentration. A confirmatory test should be a different methodology from the screening test and should be run on a different sample/specimen, if possible.
Sample Preparation
Prior to testing of any sort, the first step is sample preparation. For many methodologies, the drugs must be separated from the organic matrix in which they are suspended. This can be accomplished by heat, protein precipitation, liquid–liquid extraction, or solid phase extraction. In the postmortem setting, protein precipitation and liquid–liquid extractions are the most commonly used techniques. Depending on matrix where drug is suspended, details for each case can be found in Moffat, 2004 [45].
Screening tests
Color tests: Color tests expose an unknown drug to a chemical or mixture of chemicals. What color the test substance turns can help determine the type of drug that's present (Table 2).
| Type of Test | Chemicals | What the Results Mean | References | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Marquis Color | Formaldehyde and concentrated sulfuric acid | Heroin, morphine and most opium-based drugs will turn the solution purple. Amphetamines will turn it orange-brown. | (Manura, 1978) [46] | ||||||||
| Cobalt thiocyanate | Cobalt thiocyanate, distilled water, glycerin, hydrochloric acid, chloroform | Cocaine will turn the liquid blue. | (Haddoub, 2011; O’Neal, 2000) [47,48] | ||||||||
| Dillie-Koppanyi | Cobalt acetate and isopropylamine | Barbiturates will turn the solution violet-blue. | (O’Neal, 2000) [48] | ||||||||
| VanUrk | P-dimethylaminobenzaldehyde, | LSD will turn the solution blue- | (Scott, 2007; Moffat, |
- hydrochloric acid, ethyl alcohol purple
- 2004) [49,44]
- Duquenois-Levine
- Vanillin, acetaldehyde, ethyl
- Test alcohol, chloroform
- Scott tes
- T
Table 3: Presumptive color test of drugs of abuse
detection and identification of drugs and poisons. Around that time, the use of GC/MS started in the field of medicine [62]. Therefore, an ideal procedure for analysis of drugs and poisons was considered to be the screening by TLC, followed by the final identification and quantitation by GC/MS.
Tin layer Chromatography (TLC)
TLC is a method of chromatography in which a thin- layer made of silica gel, alumina, florisil or cellulose is coated on glass or aluminum plates. Numerous types of TLC ready for use without the need of pretreatments are commercially available. An extract fluids is spotted onto a bottom area of a plate. After drying the spot, the plate is developed with a mobile phase consisting of various ratios of organic solvents, acids and/or water [63]. During the development with a mobile phase, a compound spotted moves at a certain speed towards the top. The movement of a compound to be analyzed is usually expressed by Retention factor (_R_f) values. This number that represents how far a compound travels in a particular solvent. It is determined by measuring the distance the compound traveled and dividing it by the distance the solvent traveled. Detailed TLC conditions are described in Cooper, 2013 [34].
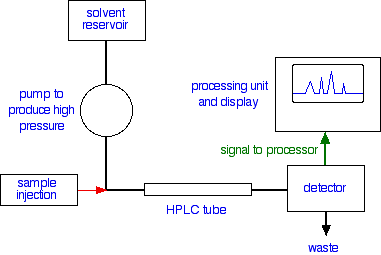
High-performance liquid chromatography (HPLC)
When combined with a detector, can be used as a screening test for a large number of drugs. Basic Principle: Drugs are dissolved into a liquid mobile phase, which is then passed through a stationary phase in a column allowing for separation and isolation of the constituents of the sample. The time taken to traverse the column is recorded by a paired detector and compared to an internal standard, allowing for detection of each component within the sample.
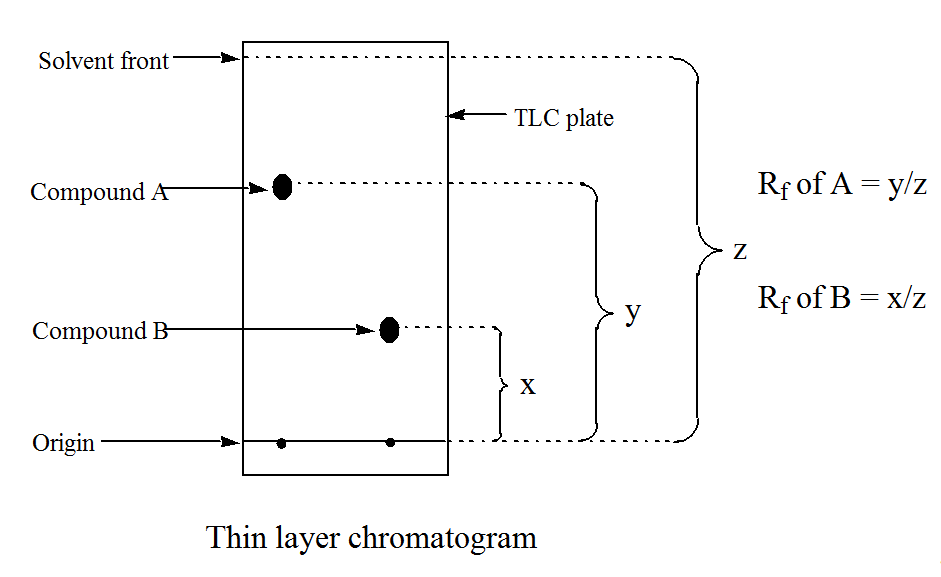
Figure 2: Principle and System Configuration of HPLC. (source: http://chemistry.tutorvista.com/analytical- chemistry/biomolecules.html, 15 October 21017) There are mainly three steps in HPLC: 1) Injection of the sample: Sample injected to column under high pressure is very easy and automated. 2) Retention time: The time taken by a certain compound to travel through the column to detector is called as Retention time. Retention times depend on various factors like the pressure in column, the particles size and nature of the stationary phase; The composition of the solvent used in column and temperature 3) The detector: Various detectors used for detecting the substance that has passed through the column. Generally ultra-violet absorption is used by using UV- detector and the output is recorded in the form of peaks.
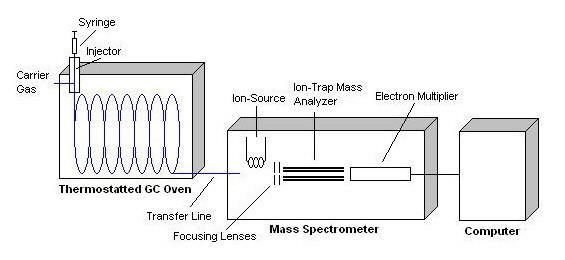
Gas Chromatography (GC)
GC was previously called “gas-liquid chromatography”. It is based on separation by partition between gaseous and liquid phases for vaporized compounds flowing together with a carrier gas (Nitrogen or Helium) inside a GC column at relatively high temperatures [64]. Therefore, GC is not suitable for analysis of non-volatile or thermolabile compounds, but is superior in separation ability, because of the high number of theoretical plates; the reproducibility of the method is excellent, because of the simple structure of the instrument. GC is now being indispensable for drug analysis. Usually paired with a flame ionization detector or nitrogen phosphorous detector for identification, (Table 3).
GC or LC paired with mass spectrometry (MS) is the gold standard for confirmatory testing in forensic toxicology. This paired method allows for mass spectral analysis of analytes after they have been separated and isolated by chromatography. Mass spectrometry is accomplished by fragmenting a molecule by a barrage of electrons and then analyzing the relative abundance of the fragments (electron ionization) or by ionizing molecules and analyzing the charge transference (chemical ionization).
| Applicable | ||||||||
|---|---|---|---|---|---|---|---|---|
| Type of Detector | D | etection Limi | t | |||||
| Samples | ||||||||
| Mass Spectrometer (MS) | Tunable for any sample | .25 to 100 pg | ||||||
| Flame Ionization (FID) | Hydrocarbons | 1 pg/s | ||||||
| Thermal Conductivity (TCD) | Universal | 500 pg/ml | ||||||
| Electron-Capture (ECD) | Halogenated hydrocarbons | 5 fg/s | ||||||
| Atomic Emission (AED) | Element-selective | 1 pg | ||||||
| Chemiluminescence (CS) | Oxidizing reagent | Dark current of Photomultiplier tubes(PMT) | ||||||
| Photoionization (PID) | Vapor and gaseous Compounds | .002 to .02 µg/L |
Table 4: Typical gas chromatography detectors and their detection limits. Mass Spectrometer (MS) detectors are most powerful of a
Table 3: Typical gas chromatography detectors and their detection limits. Mass Spectrometer (MS) detectors are most powerful of all gas chromatography detectors. In a GC/MS system, the mass spectrometer scans the masses continuously throughout the separation [65]. When the sample exits the chromatography column, it is passed through a transfer line into the inlet of the mass spectrometer. The sample is then ionized and fragmented, typically by an electron-impact ion source. During this process, the sample is bombarded by energetic electrons which ionize the molecule by causing them to lose an electron due to electrostatic repulsion. Further bombardment causes the ions to fragment. The ions are then passed into a mass analyzer where the ions are sorted according to their m/z value, or mass-to-charge ratio. Most ions are only singly charged [66].
Conclusion
Sample collection, analysis and interpretation are the key factors influencing biological specimen selection. Most forensic toxicology methods for drug analysis offer about five basic screening tests to determine the presence or absence of the majority of significant drugs. These are the amphetamines (amphetamine and methamphetamines), cocaine, cannabinoids (marijuana), narcotic (morphine, codeine and others) and Phencyclidine).The screening tests of illegal drugs is primary focused in determining what type of banned drugs a person may have taken in a variety of situations [67]. The techniques of drug analysis have continually evolved to HPLC, GC/MS, and LC/MS improving sensitivity and reducing samples sizes, thus allowing effective analysis of additional specimens such as breast milk and meconium that were previously inaccessible. For drug analysis, the process of interpretation should include consideration of all aspects of the investigation, including the analysis of multiple specimens.
References
-
Eaton DL (1996) Principles of toxicology.
-
Cooper GA Paterson S, Osselton MD (2010) The United Kingdom and Ireland association of forensic toxicologists: forensic toxicology laboratory guidelines. Sci Justice 50(4): 166-176.
-
Flanagan RJ (1998) Guidelines for the interpretation of analytical toxicology results and unit of measurement conversion factors. Annals of clinical biochemistry 35: 261-267.
-
Pounder DJ, Jones GR (1990) Post-mortem drug redistribution-a toxicological nightmare. Forensic science international. Forensic Sci Int 45(3): 253-263.
-
Dinis Oliveira RJ, Carvalho F, Duarte JA, Remião F, Marques A, et al. (2010) Collection of biological samples in forensic toxicology. Toxicol Mech Methods 20(7): 363-414.
-
Szabo B, Schlicker E (2005) Effects of cannabinoids on neurotransmission. Cannabinoids 327-365.
-
Pertwee RG (2005) Pharmacological actions of cannabinoids. Handb Exp Pharmacol 168: 1-51.
-
Health WHODoM (2009) Guidelines for the psychosocially assisted pharmacological treatment of opioid dependence.
-
Anglin MD, George S (1988) Narcotics use and crime: A multisample multimethod analysis. Criminology 26 (2): 197-233.
-
Police IAoCo (1992) Stimulants and Depressants.
-
McCall RB (1986) Effects of hallucinogenic drugs on serotonergic neuronal systems. Pharmacology Biochemistry and Behavior 24(2): 359-363.
-
Kyzar EJ, Collins C, Gaikwad S, Green J, Roth A, et al. (2012) Effects of hallucinogenic agents mescaline and phencyclidine on zebrafish behavior and physiology. Progress in Neuro-Psychopharmacology and Biological Psychiatry 37(1): 194-202.
-
Haynes A (2015) Synthetic Drugs Of Abuse.
-
Hartgens F, Kuipers H (2004) Effects of androgenic- anabolic steroids in athletes. Sports medicine 34(8): 513-554.
-
Dutta A, Uno H, Holman A, Lorenz DR, Wolinsky SM, et al. (2017) Long-term nitrite inhalant exposure and cancer risk in MSM. AIDS 31(8): 1169-1180.
-
Hassan A (2017) Inhalant Use Disorders. Substance and Non substance Related Addiction Disorder: Diagnosis and Treatment: 136.
-
Guidelines FTL (2006) Forensic Toxicology Laboratory Guidelines.
-
Wong RC (2007) Drugs of abuse: body fluid testing. Sl: Springer Science & Business Media.
-
Suzuki O (2005) How to handle biological specimens. Drugs and Poisons in Humans 1-7.
-
Schulz M, Iwersen-Bergmann S, Andresen H, Schmoldt A (2012) Therapeutic and toxic blood concentrations of nearly 1,000 drugs and other xenobiotics. Critical Care 16(4): R136-R136.
-
Kirchmann H, Pettersson S (1994) Human urine- chemical composition and fertilizer use efficiency. Nutrient Cycling in Agroecosystems 40(2): 149-154.
-
Dolan K, Rouen D, Kimber J (2004) An overview of the use of urine, hair, sweat and saliva to detect drug use. Drug and alcohol review 23(2): 213-217.
-
Kadehjian LJ (2005) Specimens for drugs-of-abuse testing. Drugs of abuse 11-28.
-
Bosker WM, Marilyn A. Huestis (2009) Oral fluid testing for drugs of abuse. Clinical chemistry 5(11): 1910-1931.
-
de Almeida PDV (2008) Saliva composition and functions: a comprehensive review. J Contemp Dent Pract 9(3): 72-80.
-
Drummer OH (2006) Drug testing in oral fluid. Clinical Biochemist Reviews 27(3): 147-159.
-
Báez H, Castro MM, Benavente MA, Kintz P, Cirimele V, et al. (2000) Drugs in prehistory: chemical analysis of ancient human hair. Forensic Science International 108(3): 173-179.
-
Boumba VA, Ziavrou KS, Vougiouklakis T (2006) Hair as a biological indicator of drug use, drug abuse or chronic exposure to environmental toxicants. International Journal of Toxicology 25(3): 143-163.
-
Cone EJ (1996) Mechanisms of drug incorporation into hair. Therapeutic drug monitoring 18(4): 438- 443.
-
Kronstrand R (2007) Drug incorporation into hair. Analytical and practical aspects of drug testing in hair: 1-23.
-
Kelly RC, Mieczkowski T, Sweeney SA, Bourland JA (2000) Hair analysis for drugs of abuse Hair color and race differentials or systematic differences in drug preferences?. Forensic Science Inter 107(1): 63-86.
-
Kidwell DA, Holland JC, Athanaselis S (1998) Testing for drugs of abuse in saliva and sweat. Journal of Chromatography B Biomed Sciences and Applications 713(1): 111-135.
-
Eckenhoff JB (1988) Sweat collection patch.
-
Drummer OH (2004) Postmortem toxicology of drugs of abuse. Forensic Science Inter 142(2-3): 101-113.
-
Cooper G (2013) Clarke's analytical forensic toxicology. Pharmaceutical Press.
-
Skopp G (2010) Postmortem toxicology Forensic science medicine and pathology 6(4): 314-325.
-
Jenkins AJ, Levine BS, Smialek JE (1995) Distribution of ethanol in postmortem liver. Journal of Forensic Science 40(4): 611-613.
-
Ashraf W (2005) Accumulation of heavy metals in kidney and heart tissues of Epinephelus microdon fish from the Arabian Gulf. Environmental Monitoring and Assessment 101(1-3): 311-316.
-
McCann UD, Szabo Z, Scheffel U, Dannals RF, Ricaurte GA (1998) Positron emission tomographic evidence of toxic effect of MDMA (“Ecstasy”) on brain serotonin neurons in human beings The Lancet 352(9138): 1433-1437.
-
Hakim M, Yoav Y, Broza†, Orna Barash†, Nir Peled, et al. (2012) Volatile organic compounds of lung cancer and possible biochemical pathways. Chemical reviews 112(11): 5949-5966.
-
Ligor M, Ligor T, Bajtarevic A, Ager C, Pienz M, et al. (2009) Determination of volatile organic compounds in exhaled breath of patients with lung cancer using solid phase microextraction and gas chromatography mass spectrometry. Clinical chemistry and laboratory medicine 47(5): 550-560.
-
Beck O (2014) Exhaled breath for drugs of abuse testing - evaluation in criminal justice settings. Sci Justice 54(1): 57-60.
-
Jenkins AJ (2013) Forensic drug testing. Principles of forensic toxicology 2.
-
Anderson C (2005) Presumptive and confirmatory drug tests. J Chem Edu 82(12):1809.
-
Moffat AC (2004) Clarke's analysis of drugs and poisons.
-
Manura J, Chao JM, Saferstein R (1978) The forensic identification of heroin. Journal of Forensic Science 23(1): 44-56.
-
Haddoub R, Daniel Ferry,a Philippe Marsala , Olivier Siri (2011) Cobalt thiocyanate reagent revisited for cocaine identification on TLC. New Journal of Chemistry 35(7): 1351-1354.
-
O Neal CL, Crouch DJ, Fatah AA (2000) Validation of twelve chemical spot tests for the detection of drugs of abuse. Forensic Science International 109(3): 189- 201.
-
Scott P (2007) Analysis of ergot alkaloids-A review. Mycotoxin Research 23(3): 113-121.
-
Fochtman FW, Winek CL (1971) A note on the Duquenois-Levine test for marijuana. Clinical toxicology 4(2): 287-289.
-
F Kelly J, Krishna Addanki, Omar Bagasra (2012) The non-specificity of the Duquenois-Levine field test for marijuana. Open Forensic Science J 5: 4-8.
-
Marcelo MCA (2016) Scott test evaluation by multivariate image analysis in cocaine samples. Microchemical J 127: 87-93.
-
Darwish IA (2006) Immunoassay Methods and their Applications in Pharmaceutical Analysis: Basic Methodology and Recent Advances. International Journal of Biomedical Science: IJBS 2(3): 217-235.
-
Moody DE (2006) Immunoassays in Forensic Toxicology. Encyclopedia of Analytical Chemistry.
-
Allen LV J, Stiles ML (1981) Specificity of the EMIT drug abuse urine assay methods. Clin Toxicol 18(9): 1043-1065.
-
Maragos C (2009) Fluorescence Polarization Immunoassay of Mycotoxins: A Review. Toxins 1(2): 196-207.
-
Lyons TP, Okano CK, Kuhnle JA, Bruins MR, Darwin WD, et al. (2001) A Comparison of Roche Kinetic Interaction of Microparticles in Solution (KIMS®) Assay for Cannabinoids and GC-MS Analysis for 11- nor-9-Carboxy-Δ9-Tetrahydrocannabinol. J Analytical toxicology 25(7): 559-564.
-
Engvall E (1980) Enzyme immunoassay ELISA and EMIT. Methods Enzymology 70: 419-439.
-
Elie MP (2006) Microcrystalline Tests in Forensic Drug Analysis Encyclopedia of Analytical Chemistry.
-
Penders J (2006) Laboratory guidelines and standards in clinical and forensic toxicology. Accreditation and quality assurance 11(6): 284-290.
-
Curling J (2007) Process chromatography: Five decades of innovation. America 3: 4.
-
Liu SY, Woo SO, Koh HL (2001) HPLC and GC–MS screening of Chinese proprietary medicine for undeclared therapeutic substances. J Pharmaceutical and Biomedical Analysis 24(5-6): 983-992.
-
Sherma J (2003) Handbook of thin-layer chromatography.
-
GC (2015) Principles of Instrumental Analysis.
-
Schauer N, Steinhauser D, Strelkov S, Schomburg D, Allison, et al. (2005) GC–MS libraries for the rapid identification of metabolites in complex biological samples. FEBS letters 579(6): 1332-1337.
-
Ross SA (2000) GC-MS analysis of the total δ9-thc content of both drug-and fiber-type cannabis seeds. J Analytical toxicology 24(8): 715-717.
-
(2006) FTLG. Forensic toxicology laboratory guidelines. SOFT and AAFS.
- Narcotics and Digital Forensics: Bridging Crimes in the Digital Age
- Ethics in Forensic Psychiatry: Principles, Dilemmas, and Human Rights
- Impact of Acute Stress on Attentional Orienting to Social Cues
- Head Injury and Intracranial Hemorrhage in Western Region of Libya
- A Forensic Study on Handedness: Examination of Handwriting Features in Right and Left Handed Writers
- Techniques for Latent Fingerprint Development Using Natural and Synthetic Powders: A Review