Sudden Death Associated with Propofol Infusion Syndrome
In forensic practice, PRIS is considered as the comorbid disease. The project was devoted to the study of PRIS signs in 38 cases of sudden death after surgical interventions. Archival forensic material of “medical cases” for the period from 2011 to 2020 was studied. The clinical and laboratory features of PRIS are summarized. It was found that the most common symptoms were lactic acidosis, hyperkalemia, and progressive heart failure. Optimization of standard forensic chemical study was carried out, in which it was established that the hydrolysis stage must be included in the urine sample preparation procedure for the determination of propofol. When conducting forensic chemical study of biological objects for the content of propofol, the analytical technologies used must have the sensitivity for detecting propofol in the blood at the level of 0.01 μg/ml or lower. Solid-phase extraction method on cartridges with mixed hydrophobic-anion exchange properties with sorbent such as Oasis MAX Cartridge 3cc, /60 mg/60μm companies Waters (USA) is 17% more effective than the routine liquid-liquid extraction method of propofol from blood. The preparation of TMS derivatives of propofol, increases the efficiency of chromatographic separation and provides the possibility for the analytical study of extracts from blood over a longer period of time (up to 24 hours).
Introduction
Propofol infusion syndrome (PRIS) is described as rare, but potentially fatal disease caused by the anesthetic use of propofol during surgery. Currently, PRIS as the cause of death is diagnosed in both children and adults [1]. The most characteristic signs and symptoms of PRIS, according to the literature, are bradycardia, arrhythmias, metabolic acidosis, hyperkalemia, rhabdomyolysis, and progressive heart failure that is resistant to therapy [2]. The risk of developing PRIS increases, when the maximum permissible duration of propofol administration (48 hours), and its single dose of more than 4 mg/kg/hour are exceeded, as well as in critical health conditions of patients due to severe previous injuries, diseases, and individual predisposition [3, 4].
In forensic medical practice, PRIS is encountered when there is suspicion that it may have caused the death of patients after surgery using propofol. When investigating such cases, forensic medical examination is prescribed to determine the mistakes made by the attending physicians. Examinations are carried out with the participation of clinical specialists. All available medical documents are analyzed.
Examination reports show that in cases of sudden death, PRIS is considered to be the comorbid disease. Propofol is a short-acting anesthetic drug used to induce and maintain general anesthesia. Its undeniable advantages are the rapid restoration of psychomotor and cognitive functions without unpleasant sensations upon awakening [5, 6]. In medical practice, registered dosage form is used, which involves an emulsion for intravenous administration that contains 10 mg/ml of propofol, regardless of the produced volume and trade names of the drug. The sedative effect begins to appear when the propofol content in the blood is between 0.001–0.004 μg/ml. For sedation during intensive care, the target blood concentration of propofol is between the range of 0.2–2.0 μg/ml. For induction of general anesthesia, the average dose of propofol in adults is between the range 2-2.5 mg/kg body weight. Propofol in the blood between 3 and 6 μg/ml maintains sufficient level for general anesthesia. The propofol concentration in the blood, decreases slowly due to its redistribution from adipose tissue [7, 8]. There is no significant accumulation of propofol during surgical procedures [9, 10].
Goal of the Work
To identify the frequency of PRIS and its characteristics in the conclusions of forensic medical examinations. To adapt methodology for the forensic chemical determination of propofol in the blood and urine of the deceased using gas- liquid chromatography methods.
Materials and Methods
We studied archival materials of forensic medical examinations performed in Moscow and Moscow Oblast during the period from 2011 to 2020. The study group of observations included 38 deaths of patients who underwent surgery, with the administration of propofol, and then PRIS developed.
The materials contained clinical examination data and laboratory test results from the medical records (medical histories) of the deceased, as well as the results of post- mortem forensic examinations. The sampling took into account characteristic PRIS features: metabolic acidosis, hyperkalemia, rhabdomyolysis, renal failure, cardiac arrhythmias, and progressive heart failure [11, 12]. The doses of propofol used, and the duration of anesthesia were determined from the medical documents. The study took into account the number of deaths by gender and age, and the distribution of cases by year. The occurrence frequency of PRIS, and symptoms were determined as the percentage relative to the total number of observations.
During the forensic chemical examination of the blood and urine from the examined corpses, an improved technique for the analysis of biological objects were used, which included the use of solid-phase extraction for blood, acid hydrolysis and liquid-liquid extraction for urine, obtaining TMS derivatives during derivatization for analysis of the obtained extracts on the Agilent 7890B/5977A chromotomass spectrometer with autosamplerG4513A and a capillary column HP-5MS 30 m x 0.25 mm, phase - 0.25 µm.
Study Results
The annual distribution of PRIS cases is presented in Table 1.
| Years | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 |
|---|---|---|---|---|---|---|---|---|---|---|
| Number of Observations | 2 | 4 | 3 | 4 | 3 | 3 | 4 | 5 | 4 | 6 |
Table 1: Frequency of PRIS During the Period 2011-2020.
The age of the deceased ranged from 6 to 67 years. The number of men and women was seen in a ratio of 17/21.
The number of cases with established excess dose of administered propofol was 15.8%. The number of cases where the infusion duration was used that exceeded the permitted 48 hours was 18.4%.
As can be seen from the table above, the most frequently identified signs & symptoms in the studied observation group were: progressive heart failure, cardiogenic shock, hyperkalemia, and increased blood lactate, which indicates progressive metabolic acidosis. Rhabdomyolysis was mentioned in almost half of the cases studied. Information on increased triglycerides levels and increased creatine kinase activity in the blood occurred in 1/3 of the studied cases. The combination of the above signs and symptoms , indicated multiple organ dysfunction syndrome.
Histological examination revealed chronic inflammatory and destructive changes in the liver and kidneys. Such findings were observed in 32 observations, which amounted to 84.2% of the total number of the studied cases with PRIS.
Conditions were established for adapting the methodology for forensic chemical testing of propofol in cadaveric blood and urine.
The frequency of PRIS characterizing signs is presented in Table 2.
| 1. | Metabolic acidosis (blood lactate> of 5 mmol/l) | 58.9 |
|---|---|---|
| 2. | Hyperkalemia (> 6.5 mmol/l) | 78.9 |
| 3. | Rhabdomyolysis | 44.7 |
| 4. | Hypertriglyceridemia (2.3–5.6 mmol/l) | 31.6 |
| 5. | High blood creatine kinase activity (>195 U/l) | 36.8 |
| 6. | Acute renal failure (blood creatinine >500 µmol/l) | 23.7 |
| 7. | Cardiogenic shock | 86.8 |
| 8. | Elevated levels of liver transaminases | 47.4 |
| 9. | Low glycogen | 78.9 |
| 10. | Hypotension | 26.3 |
| 11. | Bradycardia | 68.4 |
| 12. | Arrhythmia | 31.6 |
| 13. | Progressive heart failure | 94.7 |
| 14. | Electrocardiogram changes | 50 |
| 15. | Fever | 34.2 |
Table 2: Frequency of signs and symptoms characteristic for PRIS (%).
Chemicals and Reagents (Reagents, Chemicals and Standards)
All reagents were highly purified (HPLC grade solvents) and stored according to the manufacturer’s and supplier’s requirements. Propofol Analytical Standard 1 mg/ml in methanol (Lot# FN01251702) and thymol substance from the company Sigma-Aldrich. Solid phase extraction cartridges 3cc/60 mg/60μm Oasis MAX Cartridge from the company Waters (USA).
Sample Preparation for Gas Chromatography- Mass Spectrometry Analysis GC/MS (Sample Preparation and Extraction Procedure)
Working propofol solutions for constructing the calibration curve were prepared from the analytical standard in concentrations of 0.01, 0.05, 0.10, 0.50, 1.00, 5.00, 10.00, and 20.00 µg/ml. A thymol internal standard (IS) solution at a concentration of 10.00 μg/ml was prepared in methanol, using the mass-volume method. When preparing model mixtures, 1 ml glass vial was filled with 0.90 ml of blank blood plasma was added with 0.10 ml of propofol methanol solution to achieve the appropriate concentration, which was then mixed on a shaker for 1 minute.
Solid Phase Extraction for Blood
A preliminary comparison of the propofol extraction process from model blood mixture with a concentration of 10,000 ng/ml using C8, C18, and combined MAX cartridges showed that the extraction on a cartridge with a sorbent having mixed hydrophobic - anion exchange properties MAX (> 90%) higher and cleaner in terms of noise level in instrumental analysis, before and after the peaks of propofol and thymol. Solid phase extraction cartridges Oasis MAX Cartridge 3cc, /60 mg/60 μm from the company Waters (USA) were subsequently used for solid-phase extraction. The activation scheme for the Oasis MAX 3cc solid phase extraction cartridge was carried out by sequentially passing 1.0 ml of methanol and 1.0 ml of water through the cartridge. Then, without allowing the cartridge to dry out, 1.0 ml of blood sample was added and passed through the cartridge at the speed of 0.5 ml/min, followed by cleaning it with 1 ml of 0.1% aqueous solution of formic acid. Elution from the cartridge was carried out twice with 0.5 ml of acidified methanol (0.1% methanol solution of formic acid).
The obtained eluate was dried at 40°C in a slow flow of nitrogen. Samples were restored with 1.0 ml of methanol and 100 μl of thymol was added at a concentration of 10.00 μg/ ml. The coefficient for the extraction (yield) of propofol from model blood mixture with a concentration of 100 ng/ml was
92.9%, and at 10 µg/ml it was 98.2%. Hydrolysis: per 1 ml of urine, 1 ml of 5 M HCl was added, and hydrolysis was carried out at 100–105ºC for 1 hour. After cooling, the mixture was filtered, alkalinized with 10 M NaOH solution to pH 8-9, according to a universal indicator, and adjusted to 3 ml with phosphate buffer with pH 8.0. Liquid-liquid Extraction: added to 1.0 ml of blood or neutralized hydrolyzed urine was 0.1 ml of methanol solution of thymol (10 μg/ml). Samples were extracted with 3 ml heptane/dichloromethane/ethyl acetate (4:4:2 ratio) with continuous shaking for 15 minutes. The separation was carried out by centrifugation at 3,000 rpm for 10 minutes. The top organic layer was collected and dried at 40°C in slow nitrogen flow. Samples were reconstituted with 100 μL ethyl acetate, and 1 μL aliquot was injected into the instrument. The extraction ratio of propofol from the model blood mixture with concentration of 100 ng/ml was 76.2%, 10 µg/ml – 75.2%. Although in the routine practice of forensic chemical studies, the most widely used is the liquid- liquid extraction method. On the other hand is the extraction of propofol use solid-phase extraction, by using the Oasis MAX Cartridge 3cc, / 60 mg from a model blood mixture with concentration of 100 ng/ml, showed an increase by almost 17%.
Derivatization Obtaining TMS Derivatives
The derivation method was used, if it was necessary to analyze the extracts obtained from forensic blood test samples, longer time range than 4 hours. In addition, TMS derivatives of propofol are stable throughout the day and have more pronounced peaks in chromatograms, due to the closure of the active hydroxyl group; the detection process is affected, by changes in molecular weight values. TMS derivatives of propofol and thymol were obtained by adding 50µl of N, O-b is (trimethylsilyl) trifluoroacetamide (BSTFA) with 1% TMCS (Trimethylchlorosilane) to the dry residue after extraction, and evaporating in slow nitrogen stream at 40°C. Mixture was incubated at 60°C for 30 minutes, 1 µl aliquots were added to the instrument.
Chromotography Equipment and Conditions
Agilent 7890B/5977A chromatography-mass spectrometer with an autosampler G4513A, capillary column HP-5MS 30 m x 0.25 mm, and phase - 0.25 µm. The initial column temperature of 80°C, exposure for 1.5 minutes, rise at the speed of 40°C/min up to 135°C/min, exposure for 1 minute, rise 10°C/min up to 175°C, then 40°C/min up to 280°C, exposure 2 minutes; carrier gas helium, speed 0.9 ml/min in constant flow mode; injector thermostat 250°C, septum airflow 3 ml/min, injector mode – pulse without division, pulse pressure 30 psi up to 0.8 min, purge flow 50 ml/min after 1 minute, gas saving 20 ml/min after 3 min; MSD interface set to 280°C , MSD operating mode. The source and quadrupole temperatures were set to 230°C and 150°C, respectively. There was the solvent delay for 3 minutes. The total analysis time was 12.5 minutes. Range of recorded masses in SCAN mode, from 40 to 500 Da. In SIM mode, ions were selected by intensity: for propofol – m/z 163, 178, 117 and m/z 235, 250, 73 for TMS-propofol; thymol – m/z 135, 115, 151, and m/z 252, 267 and 73 for TMS-thymol.
Method Validation
Validation is based on the Guideline on Bioanalytical Method validation (2011, EMEA/CHMP/EWP/192217/2009 Rev. 1 Corr. 2). Model mixtures of blood prepared for analysis as described in the section “solid-phase extraction” (without derivatization), were used as the matrix for validation. Selectivity was examined by analyzing 10 ng/mL blood blank, and positive control samples (Figure 1).
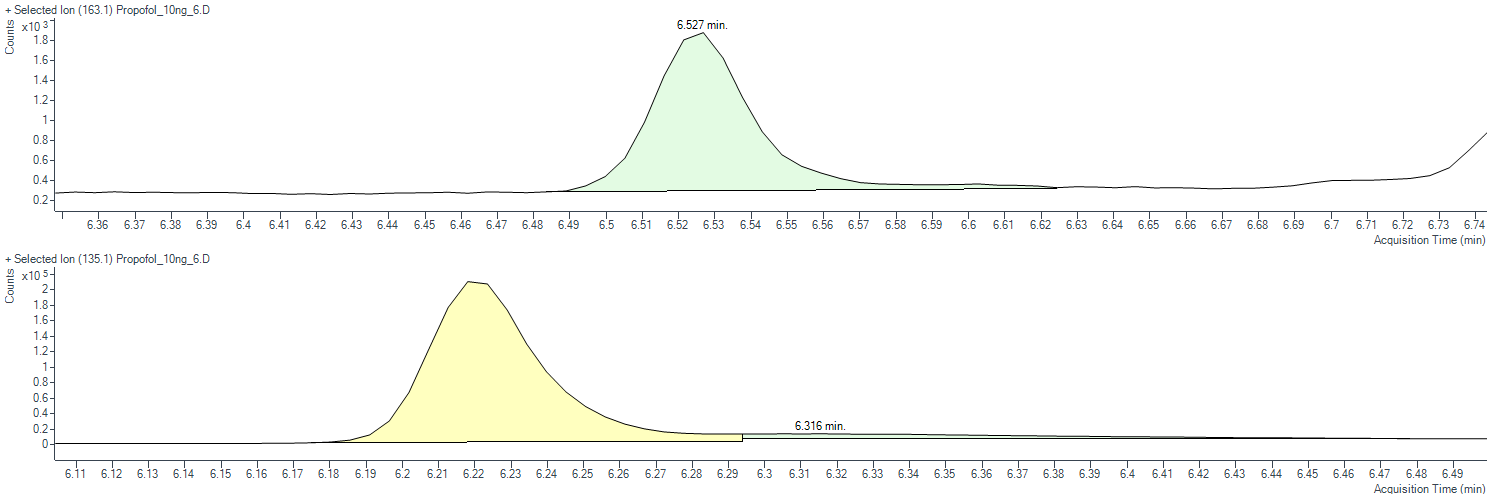
The ratio of peaks detected at retention times, corresponding to propofol, and thymol (internal standard), were at least 5 times smaller or absent altogether. Precision and accuracy were assessed using 4 control blood samples, with propofol concentrations of 0.01, 0.05, 0.50, and 15.00 μg/ml. The coefficient determination of the calibration curve was 0.9987. When determining the accuracy, the level of detected propofol concentration was between the range of 92.6% – 112.5% (N=6), and the precision error was 0.7% – 5.0% (N=6), which did not exceed the permissible criterion of 15.0%. The calibration curve was linear over the entire range of measured concentrations (0.01 – 20.00 μg/ml), and the sample transfer after the injection of the control with high propofol concentration did not exceed 1.60% (N=3).
The yield when extracting blood sample with concentration of 0.10 μg/ml was 92.9% (N=3). The matrix effect was completely compensated by the internal standard. In the control blood samples studied, propofol was completely stable within 4 hours at the temperature of +20 – 25°C and after freezing-thawing cycles, its opening level was90.18% -107.30% (N=3), and 93.93% – 111.78% (N=3), respectively, with an acceptable error criteria of15%.
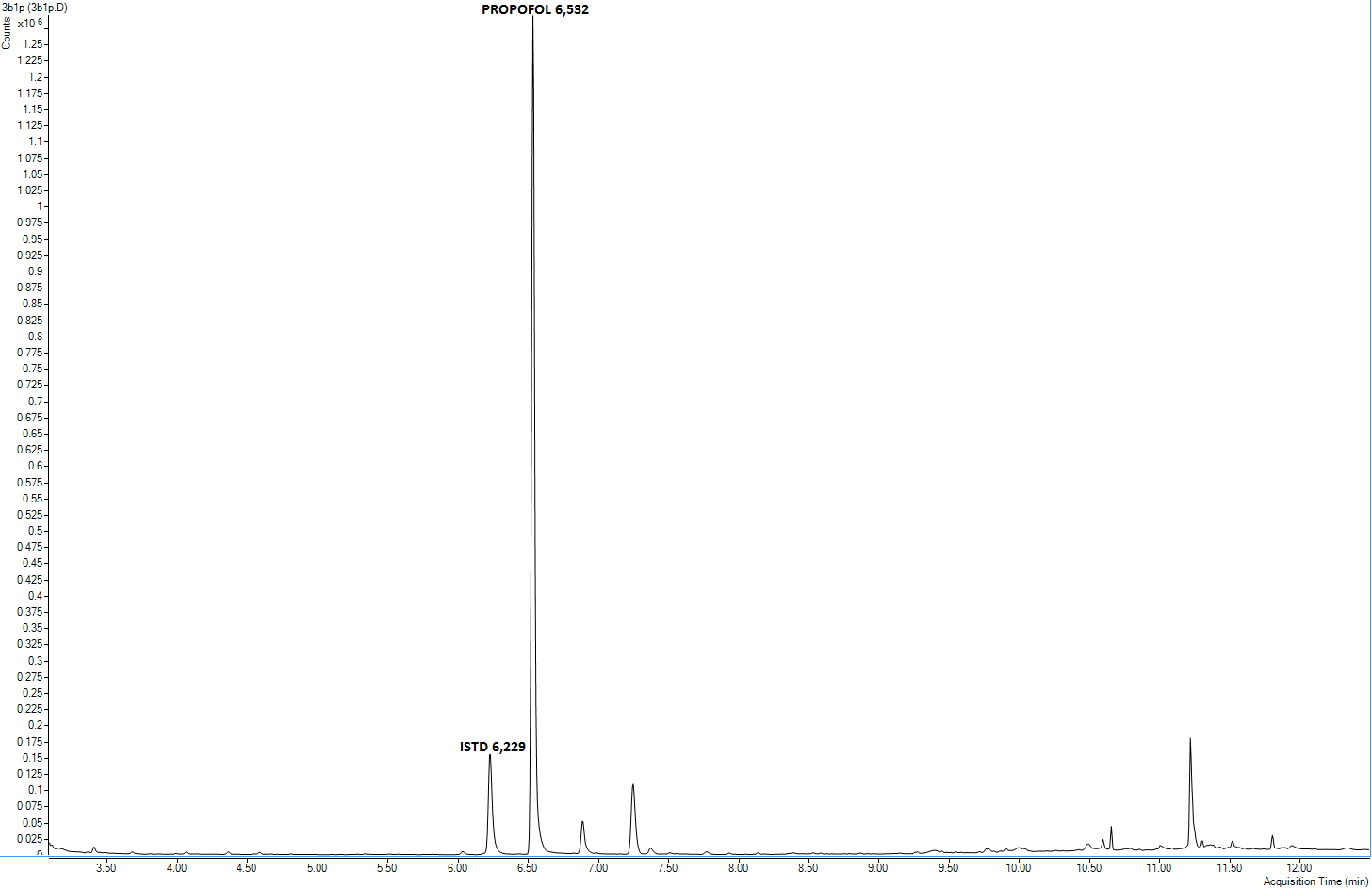
During practical expert analyzing the blood samples for the presence of propofol, clear isolated peaks of propofol and thymol were revealed in the chromatograms. The chromatogram obtained from the analysis of an expert blood sample is presented in Figure 2.
Results Discussion
Propofol infusion syndrome is rare, but remains potentially fatal complication of propofol use in anesthesia. Our study during the period from 2011 to 2020 confirmed the regularity occurrence of deaths, associated with PRIS [13]. Over the 10-year period, the number of postoperative deaths associated with PRIS increased. In 2020, the number of such cases doubled compared with 2011. In our study, cases of postoperative sudden death associated with PRIS were more common in the age between group 21–52 years (65.8%). In men, PRIS was established less frequently than in women (55.3%).
Progressive heart failure, hyperkalemia and increased metabolic acidosis level (ketoacidosis) were more frequently encountered. The changes we obtained are consistent with literature data [14].
Rhabdomyolysis was mentioned in almost half (44.7%) of the studied cases. Other signs and symptoms that may be associated with the onset of death in the early stages of the PRIS development. In the event of sudden death, pronounced disturbances in oxidative cellular respiration do not have enough time to develop [15].
Exceeding the duration propofol infusion administration longer than 48 hours, was detected in 7 cases (18.4%). Therefore, to reduce the risk of unfavorable outcome, when PRIS signs and symptoms appear, further administration of propofol should be discontinued. Based on the data in the literature [16], and the results we obtained, it should be assumed that the pathophysiological mechanism of PRIS development, is the destructive effect of propofol on the respiratory chain, reducing ATP production and cellular hypoxia.
Conclusions
According to the conclusions from forensic medical examinations, the most common PRIS signs and symptoms after surgical interventions with the use of propofol are: progressive heart failure, hyperkalemia, and metabolic acidosis (ketoacidosis). The particularity of forensic cases of PRIS are quickly occurring death, when pronounced disturbances of oxidative cellular respiration, and their consequences in the form of multiple organ disorders do not have enough time to develop.
Propofol administration further increases the risk of sudden death during the surgical intervention, in the presence of chronic inflammatory, and destructive changes in the liver and kidneys. Immediate discontinuation of further propofol administration, reduces the risk of adverse outcome.
When forensic chemical testing of biological objects for propofol content is carried out, the analytical technologies used, must have sensitivity for the discovery of propofol in the blood, at level of 0.01 μg/ml or lower, and the method of solid-phase extraction on cartridges with mixed hydrophobic- anion exchange properties with sorbent such as Oasis MAX Cartridge 3cc,/ 60 mg/60μm from the company Waters (USA) is 17% more effective, than the routine liquid-liquid extraction method of propofol from blood. The preparation of TMS derivatives of propofol increases, the efficiency of chromatographic separation and provides the possibilities for the analytical study of extracts from blood over longer period of time (up to 24 hours).
Authors’ contributions
Study concept/design: M.J. Ng, S.B. Lisovskaya, S.Y. Morozov. Literature search and data collection: M.J. Ng, A.A. Bashilov, C.C. Ng. Data analysis and interpretation: M.J. Ng, Y.E. Morozov, S.Y. Morozov. Drafting the manuscript: Ng M.J., Ng C.C., Y.E. Morozov and Lisovskaya S.B. All of the authors reviewed the drafts of the manuscript and approved the final version.
Conflict of Interest: There is no conflict of interest. Conflict of Interest: The authors declare there are no apparent or potential conflicts of interest.
Financing: The study had no sponsorship.
References
-
Krajchova A, Waldauf P, Andel M, Duska F (2015) Propofol infusion syndrome: a structured review of experimental studies and 153 published case reports. Critical Care 19: 398.
-
Fodale V, La Monaca E (2008) Propofol infusion syndrome: an overview of a perplexing disease. Drug Safety 31(4): 293-303.
-
Wahab EA, Hamed EF, Almad HS, Monem SMA, Fathy T (2018) Conscious sedation using propofol versus midazolam in cirrhotic patients during upper GL endoscopy: A comparative study. JGH Open 3(1): 25-31.
-
Li WK, Chen XJC, Altshuler D, Islam S, Spiegler P, et al. (2022) The incidence of propofol infusion syndrome in critically ill patients. J Crit Care 71: 154098.
-
Bergmann SI, Rosner P, Kuhnau HC, Junge M, Schmoldt A (2001) Death after excessive propofol abuse. International Journal of Legal Medicine 114: 248-251.
-
Trampitsch E, Oher M, Pointner I, Likar R, Jost R, et al. (2006) Propofol infusion syndrome. Anaesthesist 55(11): 1166-1168.
-
Chidambaran V, Sadhasivam S, Diepstraten J, Esslinger H, Cox S, et al. (2013) Evaluation of propofol anesthesia in morbidly obese children and adolescents. BMC Anesthesiol 13(1): 8.
-
Cortinez LI, Anderson BJ, Penna A, Olivares L, Munoz HR, et al. (2010) Influence of obesity on propofol pharmacokinetics: derivation of a pharmacokinetic model. British Journal of Anaesthesia 105(4): 448-456.
-
Nishizawa T, Suzuki H (2018) Propofol for gastrointestinal endoscopy. United European Gastroenterology Journal 6(6): 801-805.
-
Li X, Zhao Z, Liu X, Ma G, Zhu MJ (2018) Encephalopathy associated with propofol infusion Syndrome: A case report. Medicine (Baltimore) 97(1): e9521.
-
Farag E, Deboer G, Cohen BH, Niezgoda J (2005) Metabolic acidosis due to propofol infusion. Anesthesiology 102(3): 697-698.
-
Guntani A, Yoshiga R, Mii S (2020) A case of suspected propofol infusion syndrome after abdominal aortic aneurysm surgery. Surgical Case Reports 6(1): 188.
-
Mirrakhimov AE, Voore P, Halytskyy O, Khan M, Ali AM (2015) Propofol Infusion Syndrome in Adults: A Clinical Update. Crit Care 2015: 260385.
-
Savard M, Dupre N, Turgeon AF, Desbiens R, Langevin S, et al. (2013) Propofol-related infusion syndrome heralding a mitochondrial disease: case report. Neurology 81(8): 770-771.
-
Kim JY, Jeong K, Han KS, Park JE, Kim MG, et al. (2021) Anesthetic considerations of Joubert syndrome in patients with mitochondrial disease - A case report. Anesth Pain Med (Seoul) 16(2): 158-162.
-
Diedrich DA, Brown DR (2011) Analytic reviews: propofol infusion syndrome in the ICU. Journal of Intensive Care Medicine 26(2): 59-72.
- Narcotics and Digital Forensics: Bridging Crimes in the Digital Age
- Ethics in Forensic Psychiatry: Principles, Dilemmas, and Human Rights
- Impact of Acute Stress on Attentional Orienting to Social Cues
- Head Injury and Intracranial Hemorrhage in Western Region of Libya
- A Forensic Study on Handedness: Examination of Handwriting Features in Right and Left Handed Writers
- Techniques for Latent Fingerprint Development Using Natural and Synthetic Powders: A Review