Role of Preoperative MRCP in the Management of Biliary Pancreatitis: A Retrospective Study from Saudi Arabia
Background: Gallstones are the leading cause of acute pancreatitis worldwide. Acute biliary pancreatitis occurs when distal common bile duct stones obstruct the ampulla. This can result in severe consequences for some patients, including significant fluid loss, metabolic imbalances, hypotension, and sepsis. Definitive management strategies for choledocholithiasis include laparoscopic cholecystectomy and/or endoscopic retrograde pancreatography. Magnetic resonance cholangiopancreatography (MRCP) has been increasingly used to evaluate bile duct pathology, leading to more frequent pre-operative biliary duct evaluations for patients with acute gallstone pancreatitis. Despite its widespread use, there have been conflicting reports in the literature regarding its effectiveness and impact on hospital stay duration and healthcare-associated costs. Aim: The aim of this study was to compare the impact of performing MRCP in biliary pancreatitis and its utility, measure its cost-effectiveness, and assess the sensitivity and specificity of different laboratory and radiological investigations in diagnosing impacted biliary stones. Methods: This study followed a retrospective design and analyzed, the records of all patients diagnosed with acute biliary pancreatitis during the study period (2015-2019). Data regarding the following variables were obtained and analyzed from patients’ records: age, comorbidities, and previous medications of the patients; BISAP pancreatitis severity score; serum amylase, at the time of admission; serial recordings for biomarkers and liver function test results (for Day, 1, 3, and 6); ultrasonography results; computed tomography results; MRCP and ERCP results; postoperative complications; length of hospital stay in days; and the time waiting for surgery in days. Results: 133 participants were found in the hospital admission registry and included in this analysis, with an average age of 51.73 years. At the time of admission, the average serum amylase level was 1310 units/liter. Regarding the length of hospital stay, 8.9 days was the average among the patients, with a maximum length of stay of 48 days. Our analysis revealed that MRCP has a sensitivity of 77% and a specificity of 64% for detecting CBD stones. Patients who had MRCP stayed longer at the hospital with an average of 9.21 days, although the difference was not statistically significant (p-value: 0.570), compared withan average of 6.15 among patients who did not have MRCP. As for the days to surgery, the average time until surgery was 3.79 (standard deviation 3.73), with a maximum of 16 days until surgery. Patients who had MRCP had to wait for a longer period of time until surgery than their counterparts who waited for less than a day for their surgery (p-value: < 0.001). Conclusion: Our results revealed that patients who underwent MRCP preoperatively had a longer hospital stay and significantly waited longer for surgery than their counterparts. However, more multi-centered, large studies are needed to further support our findings.
Background
Gallstones are the leading cause of acute pancreatitis worldwide [1]. Acute biliary pancreatitis occurs when distal common bile duct stones obstruct the ampulla. Although most of these stones pass through the ampulla spontaneously, approximately 20% of cases do not [2]. This can result in severe consequences for some patients, including significant fluid loss, metabolic imbalances, hypotension, and sepsis [3]. Several mechanisms contribute to the development of acute biliary pancreatitis. One such mechanism is biliary duct stones (BDS), which cause trauma as they pass through the ampulla of Vater or obstruct the ampulla, leading to increased pressure in the duct of Wirsung [4]. Obstruction of the ampulla results in elevated levels of cholestatic enzymes and serum direct bilirubin in ABP [5].
Endoscopic retrograde cholangiopancreatography (ERCP) has traditionally been considered the “gold standard” for evaluating pancreaticobiliary conditions in the presence of choledocholithiasis [6]. However, ERCP is an invasive procedure with a mortality rate of up to 1% and a morbidity rate of 3-10%. Magnetic resonance cholangiopancreatography (MRCP), which has been available for over two decades, has emerged as a valuable non-invasive imaging tool for assessing the hepatobiliary tree and surrounding anatomy [7].
Over the past decade, MRCP has been increasingly used to evaluate bile duct pathology, leading to more frequent pre-operative biliary duct evaluations in patients with acute gallstone pancreatitis [8]. However, the use of MRCP in biliary pancreatitis has raised concerns about whether pancreatic inflammation reduces the ability of MRCP to visualize the distal common bile duct (CBD) and detect ampullary stones. In addition, biliary pancreatitis is often associated with relatively small stones that may not be detectable by MRCP [9]. Despite its widespread use, there have been conflicting reports in the literature regarding its effectiveness and impact on hospital stay duration and healthcare-associated costs [10, 11, 12, 13].
Definitive management strategies for choledocholithiasis include laparoscopic cholecystectomy and/or endoscopic retrograde pancreatography (ERCP) [14]. Since its introduction in the 1980s, laparoscopic cholecystectomy has become the preferred treatment for cholelithiasis. It is one of the most common laparoscopic procedures performed, with over one million procedures performed annually in the United States [15, 16].
Recent changes in lifestyle among Saudis suggest that gallstone disease is may be of increasing importance to public health. Although little research has been conducted on the prevalence of gallstone disease in Saudi Arabia on a community basis, a regional teaching hospital with 550 beds reported performing 320 Cholecystectomycholecystectomies in a single year [17]. In Saudi Arabia, the average cost of performing MRCP in a private hospital ranges from USD 1333 to 16001333 to 1600 USD. Therefore, it isIt is therefore crucial to manage acute biliary pancreatitis cost-effectively. The aim of this study was to compare the impact of performing MRCP preoperatively before laparoscopic cholecystectomy versus proceeding directly to laparoscopic cholecystectomy based only on ultrasonography (USS) results on the length of hospital stay and waiting time until surgery, and to assess the ability of MRCP for detecting CBD stones in patients with biliary pancreatitis.
Methods
This study followed a retrospective design and analyzed, the records of all patients diagnosed with acute biliary pancreatitis during the study period (2015-2019). The study was conducted in a large tertiary hospital (Armed
Forces hospitals – Southern Region) in the southern region of Saudi Arabia. Ethical approval was obtained from the institutional review board of the hospital. Data regarding the following variables were obtained from the records:; age, comorbidities and previous medications of the patients, BISAP pancreatitis severity score, serum amylase at the time of admission, serial recordings for biomarkers and liver function test results (for Day, 1, 3, and 6), ultrasonography (USS) results, computed tomography (CT) results, MRCP and ERCP results, postoperative complications, length of hospital stay in days, and the time waiting for surgery in days. In addition, the following inclusion and exclusion criteria were applied when selecting patients: Inclusion criteria;
- Patients admitted to the hospital and diagnosed with acute biliary pancreatitis during the study period.
- First attack of acute biliary pancreatitis.
- Underwent laparoscopic cholecystectomy. Exclusion criteria;
- Pregnant patients.
- Recurrent acute biliary pancreatitis.
- Nonbiliary pancreatitis.
- Post-cholecystectomy and chronic pancreatitis.
- Patients referred from other hospitals.
Data were collected from the electronic records using EXCEL sheets. Patients, identifiers remained concealed during the whole process of this analysis, and no patient was contacted to obtain any information. Data were managed and analyzed using the statistical package for social sciences (SPSS) version 25 software. Categorical data are presented as percentages and frequencies, while continuous data are presented as means and standard deviations (SD). Moreover, Spearman correlation, t-test, and ANOVA were used to test for the association between different study variables. A, P-value of 0.05 was considered statistically significant for the association, and a confidence level of 95% was used during the analysis.
Results
133 participants were eligible and included in this analysis, with an average age of 51.73 years. Most 70 patients (52.6%) were medically free from morbidities at the time of admission, and the average serum amylase level was 1310 units/liter (SD 1206) with a maximum of 7263 units/ liter. Their average BISAP score was one and the maximum reported score was three. On ultrasonography, the average CBD diameter among the participants was 5.78 mm, and the maximum reported diameter was 14.3 mm; stones were identified in 10 (7.5%) patients. CT was performed for 43 patients; most them 40 (93%) showed signs of significant pancreatic and peripancreatic inflammation. Twenty-five patients underwent ERCP, stone extraction was performed for 13 (52%) of them, and 18 (72%) of them underwent stenting. 126 patients had MRCP before their surgery, and stones were identified in 23 (17.7%) of them. Furthermore, severe postoperative complications were reported among 23 (17.3%) of the patients, (Table 1). Serial biomarkers were also reported, showing a decline in the reported values of liver enzymes after 48h when comparing the values on days one and three, especially for AST and ALT, (Table 2).
| Frequency (%) | Mean (SD) | ||
|---|---|---|---|
| Age | 51.73 (21) years | ||
| BISAP score | 1 (0.65) | ||
| Medications: | |||
| No medications | 132 (99.2) | ||
| On medications | 1 (0.8) | ||
| Comorbidities: | |||
| Medically Free | 70 (52.6) | ||
| Single Comorbidity | 25 (18.8) | ||
| Multiple Comorbidities | 38 (28.6) | ||
| Postoperative complications: | |||
| no complications | 109 (82.0) | ||
| minor postoperative complications | 1 (0.8) | ||
| severe complications | 23 (17.3) | ||
| CBD stones on USS: | |||
| CBD stone(s) present | 10 (7.5) | ||
| No CBD stone(s) | 123 (92.5) | ||
| CBD diameter on the USS | 5.78 (2.23) mm | ||
| CT scan: | |||
| CT was not done | 81 (65.3) | ||
| Normal Pancreas | 3 (2.4) | ||
| significant pancreatic and peripancreatic inflammation | 40 (32.3) | ||
| ERCP: | |||
| ERCP was not done | 108 (81.8) | ||
| Stone(s) extracted | 13 (9.8) | ||
| No stone(s) detected in the ERCP | 11 (8.3) | ||
| MRCP: | |||
| MRCP was not done | 4 (3.1) | ||
| CBD stone(s) detected | 23 (17.7) | ||
| No stone(s) detected | 103 (79.2) | ||
| Serum amylase on admission | 1310 (1206) units/liter |
Table 1: Characteristics of the study participants.
| Day 1 Mean (SD) | Day 3 Mean (SD) | Day 6 Mean (SD) | |
|---|---|---|---|
| AST | 232.30 (259.44) | 69.40 (65.43) | 48.01 (32.20) |
| ALT | 215.60 (183.70) | 125.80 (115.50) | 64.40 (38.70) |
| GGT | 235.43 (183.15) | 176.10 (137.40) | 170.70 (115.12) |
| ALP | 191.30 (144.70) | 167.80 (118.10) | 161.60 (104.20) |
| Total Bilirubin | 49.60 (74.50) | 37.83 (75.43) | 38.00 (77.12) |
| Direct Bilirubin | 28.20 (53.16) | 18.44 (46.70) | 23.20 (53.20) |
| HCT | 41.00 (6.50) | 39.00 (5.62) | 40.00 (4.90) |
| WBC | 10.21 (4.90) | 10.24 (7.40) | 9.80 (3.44) |
Table 2: Average serial serum biomarkers recorded on days 1, 3, and 6 of admission.
Regarding the length of hospital stay, 8.9 days was the average among the patients, with a maximum length of stay of 48 days. Havening comorbidities was not significantly associated with longer hospital stay (p-value: 0.151, average days: 10.47); however, the average length of hospital stay was longer among patients with multiple comorbidities compared with other groups. The length of hospital stay was also not associated with the medications that the patients were taking, or with the presence or absence of CBD stones on ultrasonography.
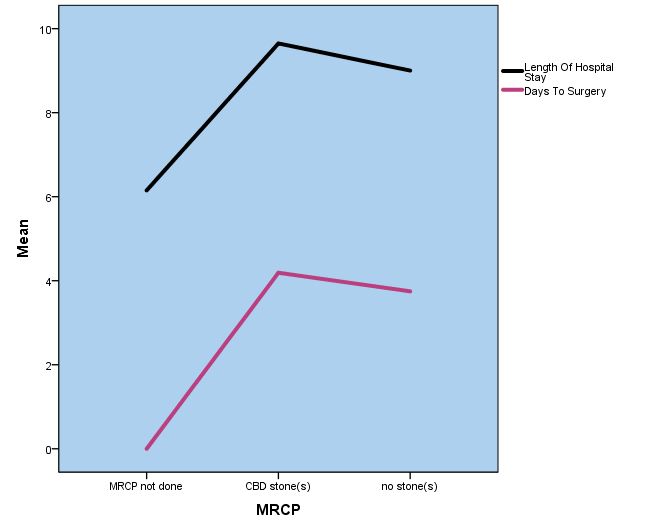
CT scan results were also not significantly associated with the length of hospital stay; however, the average length of hospital stay was slightly increased in the group of patients who showed signs of pancreatic and peripancreatic inflammation (p value; 0.689, average days: 9.6). Performing ERCP was significantly associated with longer hospital stay (p-value: 0.032). Patients who had MRCP stayed longer at the hospital with an average of 9.21 days, compared with an average of 6.15 days among patients who didnot have MRCP, although this difference was not statistically significant. As for the days to surgery, the average time until surgery was 3.79 (SD: 3.73), with a maximum of 16 days until surgery. Age was significantly associated with the number of days waiting for surgery, with younger patients having less waiting time (p-value: <0.001). In addition, a lower BISAP score was significantly associated with less time until surgery (p-value: 0.005). However, patients who underwent MRCP had to wait for a longer period of time until surgery than their counterparts who waited on average less than a day for their surgery (p-value: < 0.001), (Figure 1).
Using ERCP as a gold standard, 13 patients had CBD stones, and MRCP was able to detect CBD stones in 10 out of these 13 patients with a sensitivity of 77%. On the other hand, MRCP falsely detected CBD stones in four of the 11 patients with a specificity of 64%. Other parameters were also evaluated for predicting CBD stones, using USS. Any, CBD diameter >= 8 was considered dilated, based on which USS was able to detect stones in five out of 12 patients, with a sensitivity of 42%. Additionally, USS could directly detect two of 13 patients, with a sensitivity of 15%. The mean BISAP score was 0.6 among patients who were found to have CBD stones on ERCP compared to 0.7; this difference was not statistically significant when using the BISAP score to predict the presence of CBD stones, (P-value: 0.14). Out of the 13 patients who had CBD stones on ERCP, nine had high ALP (>= 180 IU/dl) values on the first day, and thus the sensitivity of high ALP levels in accurately predicting CBD stones was 69%. Furthermore, the sensitivity of high total bilirubin (>= 2 mg/dl) was 46%, while the sensitivity of high GGT (> 40 IU/L) was 92%. Table 3 shows the sensitivity and specificity of different parameters in predicting CBD stones.
| Sensitivity | Specificity | |
|---|---|---|
| MRCP | 77% (10/13) | 64% (7/11) |
| CBD dilation on the USS | 42% (5/12) | 78% (7/9) |
| CBD stones on the USS | 15% (2/13) | 91% (10/11) |
| High total bilirubin levels | 46% (6/13) | 40% (4/10) |
| High ALP | 69% (9/13) | 66% (6/9) |
| High GGT | 92% (12/13) | 20% (2/10) |
Table 3: Sensitivity and specificity of different parameters in predicting CBD stones.
Discussion
The prevalence of gallstone disease in Saudi Arabia, particularly at the community level, remains unclear.
However, recent studies highlight the increasing importance of addressing this topic in Saudi Arabia. For instance, at a regional teaching hospital, with 550 beds, approximately 320 Cholecystectomy are performed annually [17]. Although
our results did not demonstrate statistical significance, we observed that the use of MRCP as a preoperative procedure was associated with an extended hospital stay. Our analysis further identified that patients experienced a longer waiting period for their surgery when subjected to preoperative MRCP. MRCP is widely used in the management of acute biliary pancreatitis; however limited data exist regarding its necessity in acute gallstone pancreatitis and its associated cost implications for our health care system. Therefore, there is a need for further evaluation to determine the extent of MRCP’s utility and its impact on the cost-effectiveness of the healthcare system.
Several studies have highlighted the importance of the diagnostic capabilities of MRCP in acute gallstone pancreatitis. The results of the study by Barlow, et al. [12] clearly demonstrate that abnormal liver function tests (LFTs) and biliary dilatation observed on ultrasonography do not possess sufficient sensitivity or specificity to accurately predict the presence of choledocholithiasis on MRCP. As a result, the authors strongly advocate the inclusion of MRCP in the diagnostic protocol for all patients presenting with acute gallstone pancreatitis, irrespective of LFTs and ultrasonography findings [12]. These findings align with those of previous studies, such as the one conducted by Makary, et al. [18], which reported a sensitivity of 65% for raised bilirubin levels and a sensitivity of 55% for biliary dilatation on ultrasonography in predicting choledocholithiasis on MRCP and ERCP [18]. Similarly, our findings showed that the sensitivity of high total bilirubin was 46%. However, ultrasonography showed lower sensitivity than that reported in the literature. As for LFT results, the sensitivity of high alkaline phosphatase was similar to that reported in the literature; however, high levels of GGT were highly predictive of CBD stones with a sensitivity of 92%; despite this, both of these parameters showed low specificity. Furthermore, Lee, et al. [3] demonstrated that MRCP is an effective and noninvasive modality for detecting CBD stones in acute biliary pancreatitis, with a sensitivity of 93.3% and a specificity of 81.3% [3]. Conversely, our analysis revealed that MRCP has a sensitivity of 77% and a specificity of 64%, although the theoretical dynamic state of any biliary stone might affect these numbers as the stone might pass spontaneously between the two MRCP and ERCP as it is not usually done on the same day.
MRCP has demonstrated high accuracy in detecting CBD stones, as supported by a meta-analysis that reported a summary sensitivity of 93% and specificity of 96% [19]. Notably, as shown in a previous study, relying solely on USS and LFTs would result in the missed diagnosis of approximately 10% of choledocholithiasis cases, highlighting the need for more detailed imaging techniques such as endoscopic ultrasound [12]. Moreover, Moon, et al. [20] reported that the sensitivity of MRCP was 80.8%, compared with 20.0% for ultrasound (US) and 40.0% for computed tomography (CT) [20]. These findings highlight the effectiveness of MRCP as a noninvasive diagnostic tool for accurately detecting CBD stones in patients with ABP. Barlow, et al. [12] reported that undergoing MRCP typically incurs a cost of approximately £200 [12]. A study that delaying the performance of MRCP can result in higher accuracy, as it allows smaller stones to pass naturally. However, research indicates that waiting for MRCP can lead to treatment delays, resulting in a daily inpatient stay cost of £277 [11, 21]. MRCP is a costly procedure, amounting to over $2,000 in some reports, and could also lengthen hospital stays [8, 10]. Similar to our findings, in a secondary economic evaluation of the Gallstone PANC Trial, it has been discovered that despite a higher rate of minor complications associated with early cholecystectomy over control, the early approach reduced the 90-day length of stay by 0.96 days and had a Bayesian probability of 81% of reducing 90-day health system costs [22].
Similar findings to our study that MRCP is associated with higher costs and delays in patient stay because of its limited availability [23]. If MRCP is performed when it is not clinically indicated, it could result in longer hospital stays, patient anxiety, and ultimately, increased hospital expenses [24]. On the other hand, according to a study by Ward, et al. [6], MRCP does not increase the length of hospital stay, and the authors even endorsed the use of MRCP in biliary pancreatitis [6]. Still, MRCP remains essential to detect choledocholithiasis not seen on USS or CT despite cost and length of hospital stay according to Chen, et al. [21].
In patients undergoing laparoscopic cholecystectomy for acute gallstone pancreatitis, intraoperative cholangiography (IOC) may eliminate the need for pre-operative MRCP. According to Chen, et al. [21], there is no need for pre-operative MRCP in patients with suspected choledocholithiasis, and direct laparoscopic cholecystectomy is preferred [21]. Because MRCP is a relatively expensive study, it should be reserved for patients who will more likely benefit from it. Sevensma, et al. [10] found that patients with elevated transaminases and/ or bilirubin LFT within 48 h of admission were more likely to benefit from MRCP than those without elevated lab values [10]. Early ERCP and stone extraction decrease morbidity in patients with severe biliary pancreatitis, as noted by Lee, et al. [3]. Moreover, initial laparoscopic study found that Initial Laparoscopic cholecystectomy is associated with a shorter length of hospital stay than preoperative MRCP or ERCP, with few adverse complications noted among all groups. Therefore, laparoscopic cholecystectomy is recommended as the initial treatment method in patients with suspected choledocholithiasis [23].
Our study’s primary limitation is that it is retrospective. There are few prospective studies in this medical literature that have investigated the role of MRCP in managing acute biliary pancreatitis. Thus, there remains a need for future prospective research in this field. The number of participants in our study and the fact that it is a single-centered study are additional limitations. More multi-centered, large studies are needed to further support our findings. Furthermore, the lack of long-term follow-up data in our study prevented us from fully understanding the potential impact of MRCP on the long-term outcomes of patients with acute biliary pancreatitis. Therefore, future studies should aim to include a larger sample size and incorporate long-term follow-up to provide more comprehensive evidence regarding the role of MRCP in managing this condition.
Conclusion
The main aim of this study was to investigate the impact of preoperative MRCP on the length of hospital stay and waiting time for surgery among patients with acute biliary pancreatitis. Our results revealed that patients who underwent MRCP preoperatively had a longer hospital stay and waited longer for surgery than their counterparts. However, more multi-centered, large studies are needed to further support our findings.
Ethical Approval
This study protocol was reviewed and approved by the Research and Ethics Committee and granted the approval number [AFHSRMREC/2021/GENERAL SURGERY/505].” The study is a file review, retrospective study, and all patient information remains anonymous.
Conflict of Interest Statement
The authors have no conflicts of interest to declare.
Funding Sources
No funding was provided for this study.
Author Contributions
Dr. Shaher was the lead author of the study idea, design manuscript writing, and final editing, for Dr. Feras, Dr. Alqahtani and Dr. Almahdi helped with the analysis and literature review. Drs. Awadh, Hadi Almtheeb, and Dr. Assiri helped in data collection and analysis.
Data Availability Statement
All data generated or analyzed during this study are included in this article. Further inquiries should be directed to the corresponding authors.
References
-
Working Group IAP/APA Acute Pancreatitis Guidelines (2013) IAP/APA evidence-based guidelines for the management of acute pancreatitis. Pancreatology 13(4): e1-e15.
-
Thacoor A, Pike T, Pathak S, Dixon J, Macutkiewicz C, et al. (2019) The role of intraoperative cholangiography in patients undergoing laparoscopic cholecystectomy for acute gallstone pancreatitis: is magnetic resonance cholangiopancreatography needed. Ann R Coll Surg Engl 101(6): 428-431.
-
Lee SL, Kim HK, Choi HH, Jeon BS, Kim TH, et al. (2018) Diagnostic value of magnetic resonance cholangiopancreatography to detect bile duct stones in acute biliary pancreatitis. Pancreatology 18(1): 22-28.
-
Acosta JM, Ledesma CL (1974) Gallstone migration as a cause of acute pancreatitis. N Engl J Med 290(9): 484- 487.
-
Cohen ME, Slezak L, Wells CK, Andersen DK, Topazian M (2001) Prediction of bile duct stones and complications in gallstone pancreatitis using early laboratory trends. Am J Gastroenterol 96(12): 3305-3311.
-
Ward WH, Fluke LM, Hoagland BD, Zarow GJ, Held JM, et al. (2015) The role of magnetic resonance cholangiopancreatography in the diagnosis of choledocholithiasis: Do benefits outweigh the costs. Am Surg 81(7): 720-725.
-
Hekimoglu K, Ustundag Y, Dusak A, Erdem Z, Karademir B, et al. (2008) MRCP vs. ERCP in the evaluation of biliary pathologies: review of current literature. J Dig Dis 9(3): 162-169.
-
Sirinek KR, Schwesinger WH (2015) Has intraoperative cholangiography during laparoscopic cholecystectomy become obsolete in the era of preoperative endoscopic retrograde and magnetic resonance cholangiopancreatography. J Am Coll Surg 220(4): 522- 528.
-
Diehl AK, Holleman DR, Chapman JB, Schwesinger WH, Kurtin WE (1997) Gallstone size and risk of pancreatitis. Arch Intern Med 157(15): 1674-1678.
-
Sevensma K, Allen M, Harden R, Corser W (2017) The Use of Magnetic Resonance Cholangiopancreatography (MRCP) in the Setting of Acute Pancreatitis: When is it Most Useful. Spartan Med Res J 2(1): 5963.
-
Cavdar F, Yildar M, Tellioglu G, Kara M, Tilki M, et al. (2014) Controversial issues in biliary pancreatitis: when should we perform MRCP and ERCP. Pancreatology 14(5): 411-414.
-
Barlow A, Haqq J, McCormack D, Metcalfe M, Dennison A, et al. (2013) The role of magnetic resonance cholangiopancreatography in the management of acute gallstone pancreatitis. Ann R Coll Surg Engl 95(7): 503- 506.
-
Okan I, Bas G, Sahin M, Alimoglu O, Eryilmaz R, et al. (2012) Diagnostic value of MRCP in biliary pancreatitis: result of long-term follow-up. Acta Chir Belg 112(5): 359-364.
-
NICE (2014) Gallstone disease: diagnosis and management. Cholelithiasis and cholecystitis pp: 1-13.
-
Dubois F, Berthelot G, Levard H (1989) Cholecystectomy by coelioscopy. Presse Medicale 18(19): 980-982.
-
Freitas ML, Bell RL, Duffy AJ (2006) Choledocholithiasis: evolving standards for diagnosis and management. World J Gastroenterol WJG 12(20): 3162-3167.
-
Abu Eshy SA, Mahfouz AA, Badr A, El Gamal MN, Al Shehri MY, et al. (2007) Prevalence and risk factors of gallstone disease in a high altitude Saudi population. EMHJ-East Mediterr Health J 13(4): 794-802.
-
Makary MA, Duncan MD, Harmon JW, Freeswick PD, Bender JS, et al. (2005) The role of magnetic resonance cholangiography in the management of patients with gallstone pancreatitis. Ann Surg 241(1): 119-124.
-
Giljaca V, Gurusamy KS, Takwoingi Y, Higgie D, Poropat G, et al. (2015) Endoscopic ultrasound versus magnetic resonance cholangiopancreatography for common bile duct stones. Cochrane Database Syst Rev 2015(2): CD011549.
-
Moon JH, Cho YD, Cha SW, Cheon YK, Ahn HC, et al. (2005) The detection of bile duct stones in suspected biliary pancreatitis: comparison of MRCP, ERCP, and intraductal US. Off J Am Coll Gastroenterol ACG 100(5): 1051-1057.
-
Chen SE, Iqbal Q, Mallappa S (2023) Acute Gallstone Pancreatitis: If a Picture Is Worth a Thousand Words, How Many Images Do We Need. Cureus 15(1): e33666.
-
Isbell KD, Wei S, Dodwad SJM, Avritscher EB, Mueck KM, et al. (2021) Impact of early cholecystectomy on the cost of treating mild gallstone pancreatitis: Gallstone PANC Trial. J Am Coll Surg 233(4): 517-525.
-
Lin C, Collins JN, Britt RC, Britt LD (2015) Initial cholecystectomy with cholangiography decreases length of stay compared to preoperative MRCP or ERCP in the management of choledocholithiasis. Am Surg 81(7): 726-731.
-
Vergel YB, Chilcott J, Kaltenthaler E, Walters S, Blakeborough A, et al. (2006) Economic evaluation of MR cholangiopancreatography compared to diagnostic ERCP for the investigation of biliary tree obstruction. Int J Surg 4(1): 12-19.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review