Surgical Treatment Tumors Giant Size of the Submandibular Area
Lipomas of the submandibular space are relatively rare. The prevalence is 1% of all lipomas in the body. A lipoma may contain elements other than blood vessels of adipose tissue, muscle fibers, fibroconnective tissue, and bone tissue. Fibrolipomas of the submandibular zone are rare and account for approximately 3-4% of all head and neck tumors. With large tumors of the submandibular region, facial deformation appears. The larger the tumor, the greater the deformation of the face and neck. This report describes a case of a giant fibrolipoma in the submandibular space. We present a case of a 50-year-old man with a tumor of the right submandibular zone. The tumor appeared 8 years ago and the patient was not treated. The tumor had a locally widespread form and spread to the paropharyngeal area. Due to the difficulty of administering incubation anesthesia and taking into account possible postoperative complications, the patient underwent a tracheotomy under local anesthesia at the first stage and a radical removal of a giant tumor was performed at the second stage. Postoperative histology - Fibrolipoma. In this case, due to the large size of the tumor, in addition to deformation of the face and neck, the patient had impaired functions of swallowing food, difficulty breathing and speaking. In the postoperative period, a satisfactory aesthetic and functional result was achieved. Postoperative wound healing was primary; there were no complications.
Introduction
Lipoma is a benign soft-tissue tumor of mature adipose tissue with no cellular atypia present. It can occur anywhere in the human body where adipose tissue is present. They can be encapsulated or diffuse [1]. These are most common soft tissue tumor, and about 13-20% of cases occur in the head and neck region [2, 3].
Lipomas of the submandibular space are relatively uncommon. Prevalence is 1%. Conventionally, lipomas are divided into three types. Superficial lipomas (arise within subcutaneous tissue), deep lipoma (arise within deep soft tissue) and parosteal lipoma (arise within surfaces of the bone) [4, 5].
Patients with a giant tumor of the submandibular region with an 8-year history are rare, so it is intended to show a clinical case of a patient with a tumor of the submandibular region who underwent successful surgery.
A 50-year-old patient turned to RSSPMCO&R in March 2015 with complaints of a large tumor of the right submandibular zone, deformation of the face and neck, difficulty swallowing and difficulty moving the tongue due to compression by the tumor, as well as the appearance of pain in the tumor area (Figure 1).

Figure 1: General view of a 50-year-old patient before treatment From the anamnesis, the tumor appeared 8 years ago. At his place of residence he contacted doctors and they discovered a tumor in the submandibular region and offered surgery to remove the tumor, but the patient refused the proposed operation. After this, the patient did not go to the doctors. In March 2015, due to the appearance of pain and an increase in tumor in the submandibular area on the right, the patient contacted our clinic.
After a preliminary examination, the patient was hospitalized in the department of head and neck tumor surgery for surgical treatment.
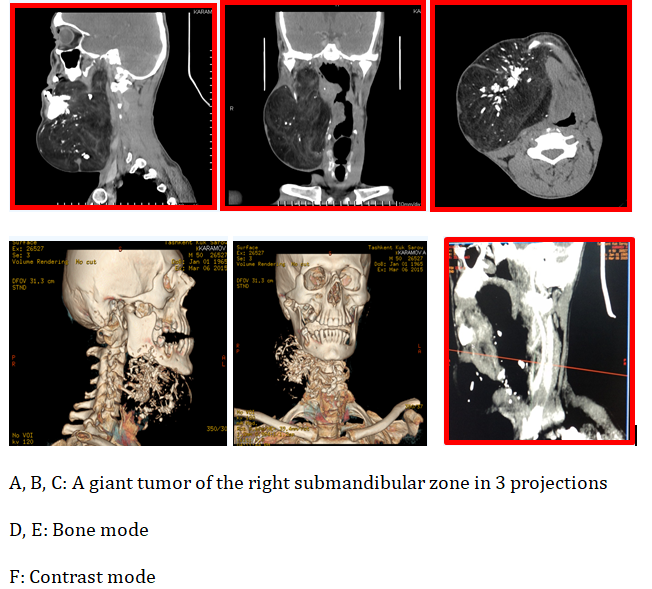
During CT examination: Computed Tomography March 2015. Figure 2 in the right lateral anterior surface of the neck there is a space-occupying formation that has spread to the right floor of the oral cavity, the right parapharyngeal region, and the pterygopalatine zone, and is also infiltrated into the tissue of the upper pole of the palate. The main part of the formation is formed by adipose tissue, on the surface of which multiple scars of indeterminate shape are found. The size of the formation is 14.9x20.5x17.0 cm. Signs of minor destruction of the porous part of the bone in the area of the body and angle of the right lower jaw were revealed. The condition of the vascular cavity after the introduction of a contrast agent in the veins of the neck trunk is satisfactory, all vessels are located lateral and dorsal to the formation, no signs of germination into the vessels were found.
Ultrasound + Doppler March 2015 - on the right submandibular region there is a formation with compression of the submandibular salivary gland, the common carotid artery and the vein jugularis interna, as well as spreading into the floor of the oral cavity. The formation has an irregular shape measuring 196x143x170 mm, a heteroexogenous structure, with mixed vascularization, without deformation of the common carotid artery, the blood flow in the jugularis interna vein has slowed down, and it has expanded to 23x24 mm. The boundary between the formation and the vessel wall is clear, no signs of proliferation were found. Conclusion: soft tissue tumor of the right submandibular zone.
Neurofibrolipoma? Fine needle aspiration cytology revealed fat droplets.
Status Localis
There is asymmetry in the neck area. In the submandibular region on the right and in front there is a large tumor with a soft elastic consistency of 25x20x18 cm, clear boundaries, spreading to the floor of the mouth and moving the tongue to the left. Due to the large size of the tumor in the sublingual region, the tongue stands perpendicular. There is difficulty swallowing and difficulty moving the tongue due to compression by the tumor, as well as the appearance of pain in the tumor area. Regional lymph nodes are not enlarged (Figure 1).
A patient diagnosed with a soft tissue tumor of the legal submandibular region underwent surgery on March 11, 2015. The first stage, due to the difficulty of administering incubation anesthesia and taking into account possible postoperative complications, a tracheotomy was performed under local anesthesia and the second stage was the removal of a giant tumor from the submandibular region on the right.
During the operation: a skin incision was made from the earlobe on the right, slightly bordering it, parallel to the edge of the lower jaw, to the angle of the lower jaw on the left. A thinned m. was revealed directly subcutaneously. Platisma, in the place of greatest protrusion in the form of sparse muscle fibers. Dissected m. platisma, a voluminous formation of adipose tissue is determined, consisting of three vaguely defined lobes covered with a thin membrane. At the base, the membrane is thinned and grows into the intermuscular spaces. The submandibular salivary gland is located medial to the tumor. In (Figure 3) the stage-by-stage removal of the tumor in the submandibular region is visible.
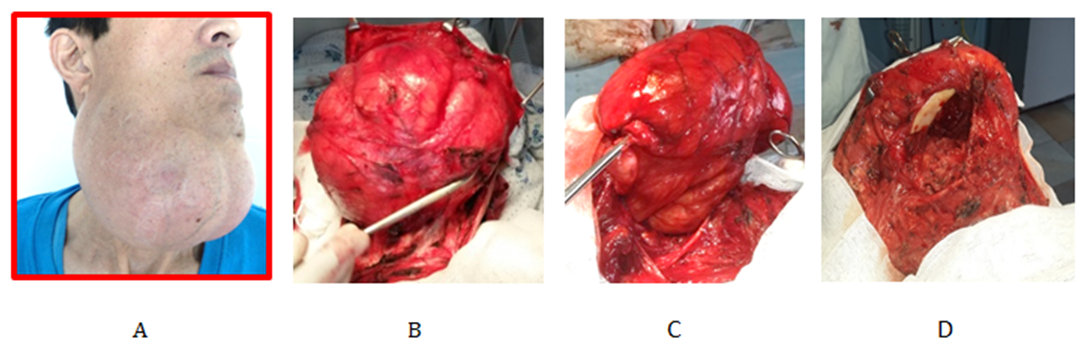
The tumor was isolated bluntly, and at the base it was isolated sharply and radically removed. The upper edge of the tumor was fused to the body and lower edge of the lower jaw. Calcified bone areas were found in this place and, with technical difficulties, they were removed separately from the main mass of the tumor. After removal of the tumor, during the audit, bone destruction in the area of the body and angle of the right lower jaw was not detected, and after removal of the tumor, the integrity of the oral mucosa was preserved. Due to the peculiarity of the location of the submandibular salivary gland, it was removed in a single block. In addition, a part of the tumor that spread to the right parapharyngeal region and from the remaining anatomical parts of the head and neck where the tumor spread was radically removed.
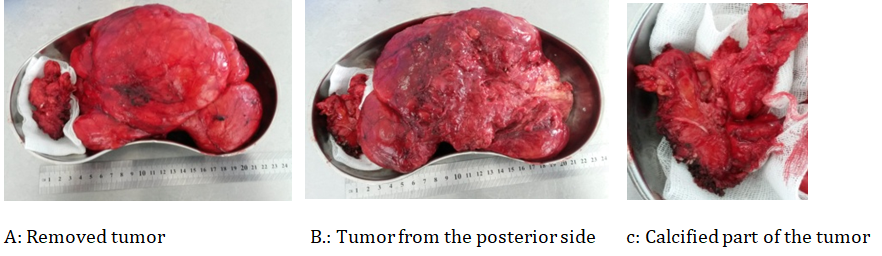
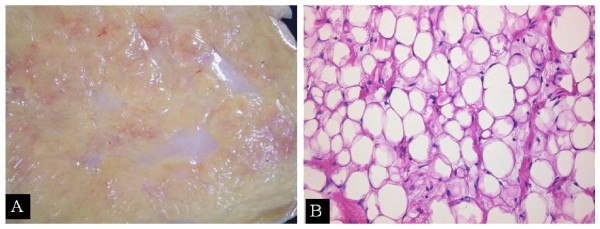
When examining a gross specimen, the tumor is pink, oval in shape, consisting of adipose tissue measuring 24x18x16 cm, weighing ~ 1300 grams. When cut, the tumor had fatty tissue. In the part fused to the lower jaw, bone calcifications were found in the tumor, which indicates how long ago the tumor appeared (Figure 4). Postoperative Histology No. 3043-44 o/15 - fibrolipoma.
In the postoperative period, a satisfactory aesthetic and functional result was achieved. Postoperative wound healing is primary. There were no postoperative complications. The patient was discharged home. (Figure 6).
The patient came for a follow-up examination 8 years later in August 2023; there were no signs of tumor recurrence.
Discussion
Head and neck lipomas are fairly common but their presentations in sites suchas the submandibular, sublingual and submental regions are rarely seen. The rarity of their presentation in these sites can often lead to difficulties in making clinical diagnosis [6].
Lipomas are generally asymptomatic and gradually progressive in size, causing aesthetic and functional deficits such as difficulty in chewing and speech (as exemplified in our patient).
One way of classifying lipomas is on the basis of their weight or size. A tumour is classified as a giant lipoma if the size is greater than 100 mm in one dimension or the weight is greater than 1000g [7, 8]. The specimen in our patient weighed 1300 g and measured 240x180x160 mm. Obesity and local growth of adipose tissues (hypertrophy theory) may both be responsible for formation of a lipoma [9].
Fibrolipoma is a histological variant of lipoma characterized by a significant fibrous component intermixed with lobules of adipose tissue [10].
Lipomatous lesions of the parotid gland are rare occurrences, and are even rarer in the submandibular gland [11, 12, 13, 14]. Agaimy, et al. [13] conducted the most recent large- scale study of lipomatous neoplasms of the salivary glands, which included 29 lipomatous tumors of the parotid gland and 2 lipomatous tumors of the submandibular gland. Both the submandibular gland tumors were ordinary lipomas [13].
A study that examined the incidence of salivary gland tumors for 20 years in a defined population revealed that only 2 submandibular lipomatous tumors (lipoblastomas) developed during the investigation. Moreover, other studies that focused on soft tissue lesions of the salivary glands did not distinguish between the sites of occurrence or included lesions of the parotid gland only [11, 15].
In the case of submandibular gland, ordinary lipoma occurs in the submandibular space or variant lipomas occurred within the submandibular gland [16, 17]. However, there are few reports or studies on ordinary lipomas within the salivary glands. Based on previous studies, we cannot assume that ordinary lipomas occurring inside the submandibular gland are more common than other variants [18].
The prognosis of lipoma is generally favorable, and recurrence is unlikely when surgery is performed appropriately. However, a case in which a lipoma of the buccal mucosa, which was diagnosed by biopsy, underwent transformation to liposarcoma has been reported [19].
Conclusion
In conclusion, we report a rare case of a giant fibrolipoma of the right submandibular zone that extended to the right floor of the mouth, right parapharyngeal region and pterygopalatine zone. The complications that arose with the gigantic size of the tumor: deformation of the face and neck, difficulty swallowing and difficulty moving the tongue, as well as the appearance of pain in the tumor area in the postoperative period were eliminated, i.e., a satisfactory aesthetic and functional result was achieved. Careful diagnostic measures made it possible to carry out a radical operation. The main treatment method for giant lipomas is surgical removal of the tumor.
References
-
Buric N, Krasic D, Visnjic M, Katic V (2001) Intraosseous mandibular lipoma: A case report and review of the literature. J Oral Maxillofac Surg 59(11): 1367-1371.
-
Bandéca MC, de Pádua JM, Nadalin MR, Ozório JE, Silva- Sousa YT, et al. (2007) Oral soft tissue lipomas: A case series. J Can Dent Assoc 73(5): 431-434.
-
Hemavathy S, Roy S, Kiresur A (2012) Intraosseous angiolipoma of the mandible. J Oral Maxillofac Pathol 16(2): 283-287.
-
Pusiol T, Franceschetti I, Scialpi M, Piscioli I (2009) Oncocytic sialolipoma of the submandibular gland with sebaceous differentiation: A new pathological entity. Indian J Pathol Microbiol 52(3): 379- 382.
-
Sathyaki DC, Jyothi Swarup R, Mohan M, Rekha Varghese (2014) Lipoma of the submandibular space. J of Oral and Maxillofacial Pathology 18(1): 149.
-
Rikhotso RE, Mhlanga G, Bobat M (2017) Giant Lipoma of the Head and Neck Region: Case Report and Review of the Literature. Open Journal of Stomatology 7(11): 469- 474.
-
Sanchez MR, Golomb FM, Moy JA, Ptozkin JR (1993) Giant Lipoma: Case Report and Review of the Literature J Am Acad Dermatol 28(2): 266-268.
-
Kalia V, kaushal N, Pahwa D (2011) Giant Subcutaneous Solitary Lipoma Arising in the Neck: Case Report and Review of Literature. Web med Central Maxillofacial Surgery 2(4): WMC001838.
-
Rikhotso RE, Mhlanga G, Bobat M (2017) Giant Lipoma of the Head and Neck Region: Case Report and Review of the Literature. Open Journal of Stomatology 7(11): 469- 474.
-
Manjunatha B S, Pateel GS, Shah V (2010) Oral fibrolipomaa rare histological entity: Report of 3 cases and review of literature. Journal of Dentistry 7(4): 226- 231.
-
Cho KJ, Ro JY, Choi J, Choi SH, Nam SY, et al. (2008) Mesenchymal neoplasms of the major salivary glands: clinicopathological features of 18 cases. Eur Arch Otorhinolaryngol 265(S1): 47-56.
-
Starkman SJ, Olsen SM, Lewis JE, Olsen KD, Sabri A (2013) Lipomatous lesions of the parotid gland: Analysis of 70 cases. Laryngoscope 123(3): 651-656.
-
Agaimy A, Ihrler S, Markl B, Lell M, Zenk J, et al. (2013) Lipomatous salivary gland tumors: a series of 31 cases spanning their morphologic spectrum with emphasis on sialolipoma and oncocytic lipoadenoma. Am J Surg Pathol 37(1): 128-137.
-
Bradley PJ, McGurk M (2013) Incidence of salivary gland neoplasms in a defined UK population. Br J Oral Maxillofac Surg 51(5): 399-403.
-
Ito FA, Ito K, Vargas PA, de Almeida OP, Lopes MA (2005) Salivary gland tumors in a Brazilian population: a retrospective study of 496 cases. Int J Oral Maxillofac Surg 34(5): 533-536.
-
Ahn D, Park TI, Park J, Heo SJ (2014) Oncocytic sialolipoma of the submandibular gland. Clin Exp Otorhinolaryngol 7(2): 149-152.
-
Weiss A, Shnayder G, Tagliareni J, Wun E, Clarkson E, et al. (2012) Large unilateral neck mass in submandibular region. J Oral Maxillofac Surg 70(4): 842-850.
-
Lee YW, Chung J (2021) Intraglandular Ordinary Lipoma of the Submandibular Gland. Ear Nose Throat Journal 100(5): 587S-589S.
-
Yamada K, Dohara Y, Nagata M, Kawashima K, Yamashita S (1979) A case of liposarcoma of the cheek. Japanese Journal of Clinical Oncology 9(1): 123-129.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review