Internal Hernias: Diagnosis and Management
Introduction: Internal hernias are rare, with an overall incidence of less than 1%. They account for 0.5 to 5.8 % of cases of intestinal obstructions. If left untreated, their overall mortality exceeds 50 % in cases of strangulation. The aim of this work is to report 04 new cases of different types of internal hernias and to review the literature on the circumstances of occurrence, discovery, and therapeutic modalities for internal hernias. Observations: We report four (04) observations concerning different types of internal hernias: (02 peri-cecal internal hernias, one hernia through the Winslow's hiatus, and one supra-vesical internal hernia), all revealed by clinical presentations of acute intestinal obstructions and confirmed by preoperative CT scan. Our patients (03 men and 01 woman) have an average age of 63 years. All 04 cases were operated on urgently, with 03 undergoing laparotomy and 01 undergoing laparoscopy. The procedure performed is the reduction of the hernia (viable strangulated small bowel loops) with closure of the hernial orifice to prevent recurrences. Postoperative courses were uneventful in all four patients. The average length of hospital stay is 02 days. After a follow-up ranging from 02 years to 08 years, no recurrence was observed. Conclusion: Internal hernias are rare and should be considered in cases of acute intestinal obstruction, especially in patients without abdominal surgical history or trauma. Laparotomy remains the most commonly used surgical approach, but laparoscopy is increasingly reported in recent publications.
Introduction
Internal hernias are rare, with an overall incidence of less than 1% [1]. They account for 0.5 to 5.8% of cases of intestinal obstructions [2]. If left untreated, their overall mortality exceeds 50% in cases of strangulation [1]. The different types of internal hernias are usually presented according to their relative frequency and anatomical location, according to the classification proposed by Welch [3]. According to this classification, para-duodenal hernias account for 50 to 55%, peri-cecal hernias for 10 to 15%, trans-mesenteric hernias for 08 to 10%, omental foramen hernias for 06 to 10%, intersigmoid hernias for 04 to 08%, pelvic hernias for 06%, and finally through the broad ligament 4 to 05% [3]. From a pathophysiological point of view, a distinction is made between hernias through a normal or paranormal peritoneal orifice and internal hernias developed through an abnormal peritoneal orifice [3].
The aim of this work is to report 04 new cases of different types of internal hernias and to review the literature on the circumstances of occurrence, discovery, and therapeutic modalities for internal hernias. In this work, we will not address postoperative internal hernias.
Observations
Observation N° 01
A 72-year-old man, with no pathological history, consulted urgently for epigastric abdominal pain, accompanied by nausea and cessation of bowel movements and gas, evolving for eight (08) hours. Abdominal palpation revealed tenderness and dullness in the epigastric region and left hypochondrium. The rest of the exam was normal. The biological assessment showed no abnormalities.
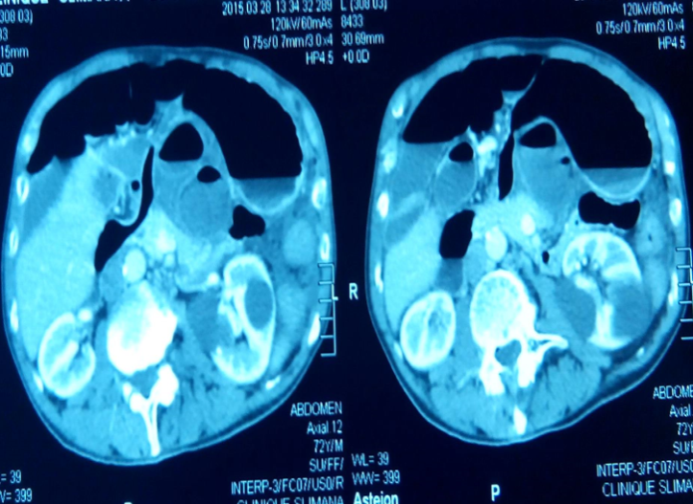
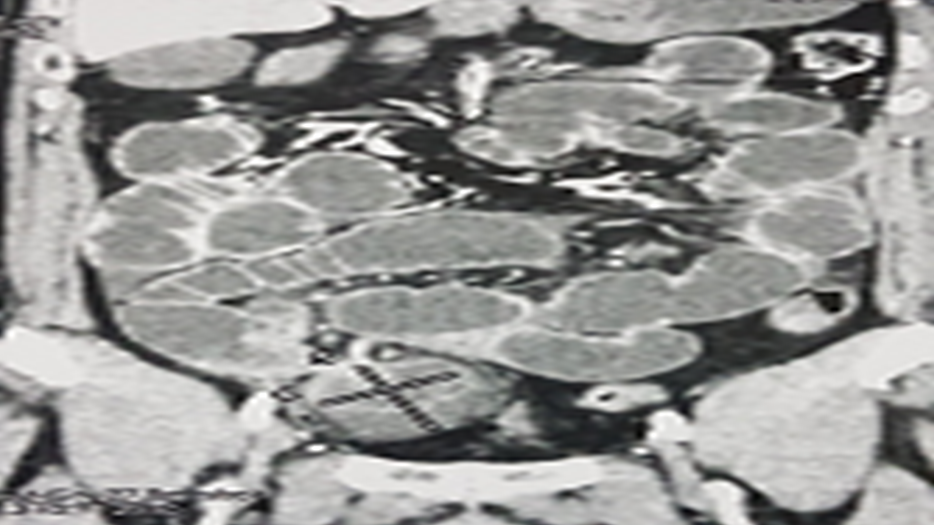
Abdominal X-ray without preparation: central hydro- aerial levels, jejunal, with an epigastric location. The abdominal CT scan revealed an acute intestinal obstruction originating from an internal hernia through the Winslow’s hiatus (Figure 1).
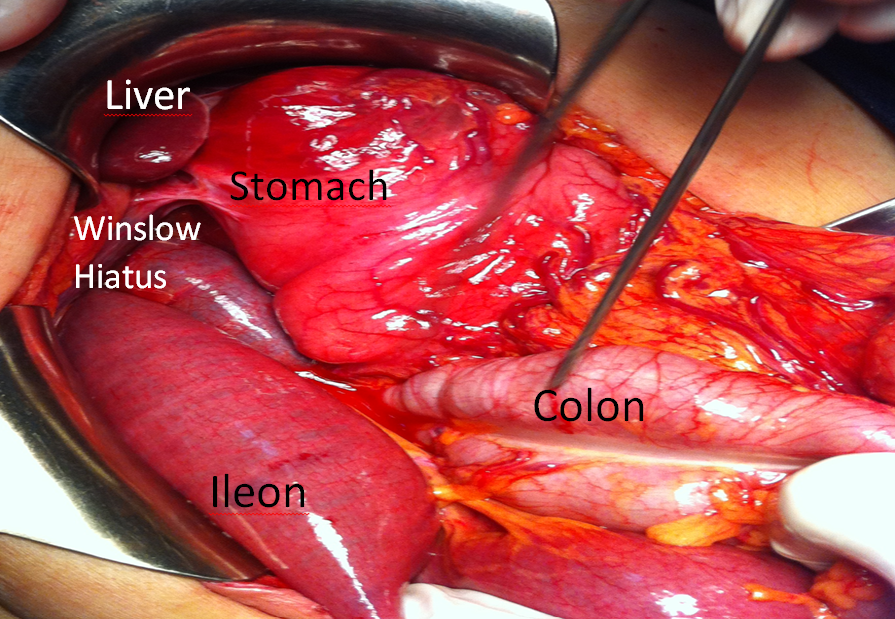
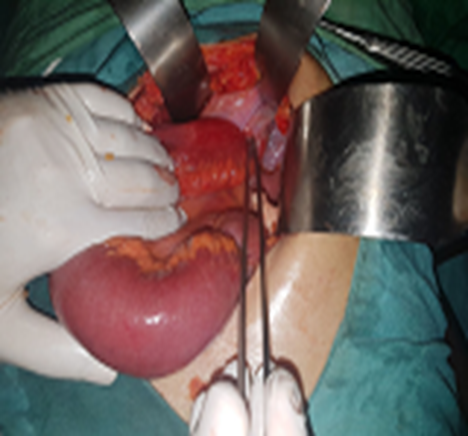
The patient underwent emergency surgery by midline laparotomy, where we found an incarceration of the ileum for approximately 40 centimeters, in the omental bursa through the Winslow’s hiatus. Treatment consisted of opening the omental bursa, releasing the incarcerated loop, which was cyanotic but quickly regained its normal appearance (Figure 2). To prevent recurrences, we closed the Winslow’s hiatus.
The post opérative follow-up was simple, feeding and discharge are done on the first post opérative day.
Observation No. 02
A 57-year-old woman, hypertensive under treatment for 05 years, admitted urgently for right iliac fossa pain, with nausea and cessation of bowel movements and gas, evolving for 48 hours. Clinical examination found a patient in good general condition, non-distended abdomen, tenderness and dullness in the right iliac fossa. The rest of the examination was normal. Blood tests were unremarkable.The abdominal- pelvic CT scan revealed an intestinal obstruction caused by an incarcerated small bowel loop in the retrocecal region.
The patient underwent emergency surgery by midline laparotomy. Intraoperative exploration found an ileal loop incarcerated in the retrocecal region, with upstream small intestine distension. We released the strangulated bowel loops, which were viable, and fixed the right colon to the posterior abdominal wall to prevent recurrences. Postoperative courses were uneventful, and the patient was discharged on postoperative day 02.
Observation N° 03
A 68-year-old man, diabetic under treatment, with no abdominal surgical history, consulted urgently for right iliac fossa pain, with vomiting, evolving for 03 hours in an afebrile context. Clinical examination found tenderness in the right iliac fossa with clear defense, with the rest of the abdomen being soft and painless. The clinical picture strongly suggested a surgical emergency, particularly that of uncomplicated acute appendicitis. Blood tests were normal. Emergency ultrasound and CT scan revealed thickening of the terminal ileum, and the appendix was not visualized.
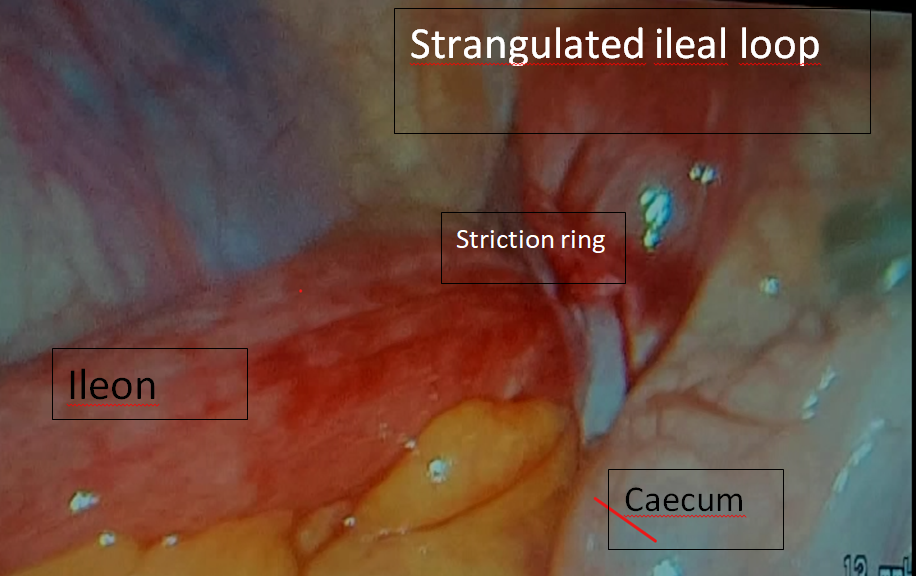
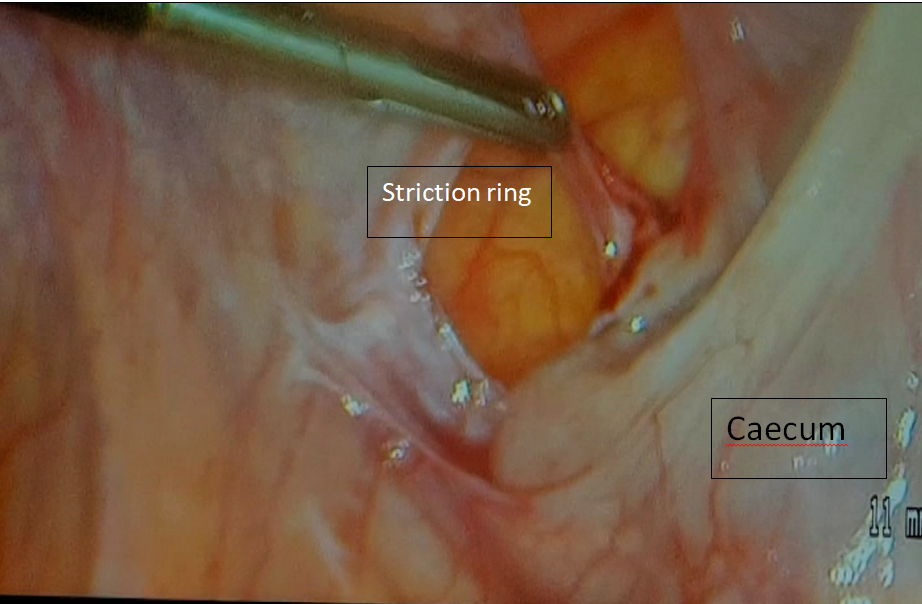
Given this discrepancy between clinical data and radiological findings (non-visualized appendix), and with the patient’s consent, we opted for diagnostic laparoscopy and potentially therapeutic. Intraoperative laparoscopic exploration found an internal hernia of a small bowel loop (ileum), incarcerated in the retrocecal space with a small amount of reactive fluid in the pouch of Douglas (Figures 3 & 4).
We proceeded with the reduction of the incarcerated loop, which was cyanotic but quickly regained normal coloration. The appendix was retrocecal, macroscopically healthy, and intentionally left in place. To prevent recurrences, we closed the hernial orifice. Postoperative courses were uneventful. Resumption of feeding and discharge of the patient were done on the first postoperative day.
Observation N° 04
A male patient, 60 years old, with a history of cardiac arrhythmia due to atrial fibrillation (ACFA) under vitamin K antagonist, consulted urgently for an obstructive syndrome, characterized by diffuse abdominal pain, vomiting, and cessation of bowel movements and gas, evolving for 03 days in a febrile context at 38.8°C. Physical examination found a distended, tympanic abdomen with generalized abdominal defense but no signs of peritonitis. Hernial orifices were free, and rectal examination was normal. The rest of the somatic examination was unremarkable. Laboratory tests found leukocytosis at 22000 with functional renal insufficiency (creatinine at 14.4 mg/L). The abdominal-pelvic CT scan Figures 5 & 6 revealed significant small bowel distension upstream of a hernia sac located in the hypogastric region measuring 63 mm in the major axis with incarceration of an ileal loop suggesting an internal hernia-related obstruction.

The patient underwent emergency surgery by sub- umbilical median laparotomy. Intraoperative exploration found an ileal loop incarcerated in the supra-vesical space with small bowel distension upstream (Figure 7).
After enlarging the neck, we reduced the incarcerated loop, which was painful but viable, and closed the hernial orifice (Figures 8-10). Postoperative courses were uneventful. Feeding was resumed on the first postoperative day, and discharge on the 2nd day.



Discussion
Internal hernias are defined by the protrusion of a viscus (frequently the small intestine) through a normal or abnormal peritoneal orifice located peritoneally or mesenterically [4]. There are different types of internal hernias [3, 5]. Although these hernias are rare, we have reported three different varieties of internal hernias (Blandin hernia, retrocecal hernia, and supra-vesical hernia). The omental foramen hernia (Blandin hernia) corresponds to the protrusion of the intestine through Winslow’s hiatus, first described in 1823, and accounts for 8% of all internal hernias of the abdomen [3]. Peri-cecal internal hernias constitute 10 to 15% of internal hernias; they are mostly congenital and are usually revealed in adulthood [6, 7, 8]. Four types of peri-cecal hernias are classically described corresponding to four peritoneal recesses [2, 4, 6]. Inside the cecum, the upper ileocecal recess is located between the termination of the distal ileum and the peritoneal fold of the anterior cecal artery; the lower ileocecal recess is located between the meso-appendix and the ileocecal fold. Outside the cecum, the paracolic recesses (paracolic sulci) located in the paracolic gutter are inconsistent [2, 4, 6]. Behind the cecum, the retrocecal recess is located between the cecum and the posterior abdominal wall and laterally delimited by two peritoneal folds; it is the widest recess.
The supra-vesical hernia was first described in 1804 by Sir Astley Cooper; it is unusual and rarely reported in the literature [9]. It corresponds to the incarceration of viscera in the supra-vesical fossa, which is an area of the abdominal wall between the remainder of the urachus (median umbilical ligament) and the remainder of the left or right umbilical artery (medial umbilical ligament) [10].
Internal hernias are often revealed by a picture of acute intestinal obstruction, generally nonspecific, always involving abdominal pain and vomiting, with ischemic component by strangulation [5, 9, 11, 12]. Sometimes the diagnosis can be made outside acute episodes [3]. Preoperative discovery, while rare, can exceptionally be considered based on radiological signs [9]. In our observation, the four cases of internal hernias that we reported were revealed by acute intestinal obstructions.
CT has become the imaging technique of choice in these patients due to its availability, speed, and multiplanar reformatting capabilities [1]. In our observation, preoperative CT confirmed the diagnosis of acute intestinal obstruction caused by an internal hernia in three patients. However, in the fourth patient, the CT scan could not determine the origin of the intestinal obstruction.Blood tests are not necessary for diagnosis [13]. In our 04 patients, blood tests did not contribute to the positive diagnosis.
Treatment is surgical, with the classic midline approach recommended for acute occlusive syndrome in the absence of preoperative diagnosis [12]. Laparoscopic approach may, however, be considered, both for diagnostic and therapeutic purposes, as long as the defect is anterior [12]. In our observation, the midline approach was used in three patients. In the fourth patient, the CT scan could not determine the origin of the intestinal obstruction, which led us to perform diagnostic laparoscopy for diagnostic and potentially therapeutic purposes. Technical ease via laparoscopic approach, in addition to the well-known advantages of this approach, should encourage surgeons to use it more commonly in such situations.
Intraoperatively, the diagnosis is easy to establish [6, 12]. The small intestine is often strangulated [3]. The first step of the intervention is to reduce the hernia [13]. Resection may be necessary in case of necrosis of the strangulated viscera [6]. Prevention of recurrence varies depending on the type of internal hernia. In case of internal hernia through Winslow’s hiatus, to prevent recurrence, it is essential to replace the intestine and the greater omentum in the anatomical position. Direct closure of Winslow’s hiatus by suture is not recommended, partly due to the risks of vascular injury, even thrombosis of the portal vein, and partly because it most often closes spontaneously due to local postoperative inflammatory reaction. Finally, some propose to release the right colonic angle to fix it to the anterior abdominal wall to prevent the small intestine from accessing the supra- mesocolic stage [12]. In our case, to prevent recurrence, we closed Winslow’s hiatus. No complications were observed. In the case of peri-cecal hernia, simple point obliteration can be performed in the presence of a small sac; collapse by coloparietal detachment in the plane of the right Toldt fascia will be performed in the presence of a larger sac, to avoid recurrence [6]. Finally, in case of supra-vesical internal hernia, simple suture of the hernial sac is sufficient for some authors and prevents recurrences [14]. This is the case of our patient, where no recurrence was noted after 04 years of evolution.
Conclusion
Internal hernias are rare, often revealed by a picture of acute intestinal obstruction. Abdominal CT, due to its availability and reliability, is the first-line technique for diagnosis. Treatment consists of reducing the hernia associated or not with visceral resection depending on the vitality of the strangulated viscera. Prevention of recurrence will be based on the location of the hernia.
Ethics Approval
The data and files of patiénts presented in this manuscript are available at the Department of General Surgery of the University Hospital of Ain Taya.All patients consent to their inclusion in this work and the publication of the results.
Conflicts of Interest
The author declare that they have no conflicts of interest.
Author Contributions
All authors contributed to this work
Funding
Funding will be provided by the lead author, with no funding from any other source.
Availability of Data and Materials
The data (Patient records, information sheets for each patient) are available and entered in Excel and Word formats
References
-
Martin LC, Merkle EM, Thompson WM (2006) Review of internal hernias: radiographic and clinical findings. AJR Am J Roentgenol 186(3): 703-717.
-
Cazejust J, Lafont C, Raynal M, Azizi L, Menu Y, et al. (2013) Internal hernia through the omental foramen. Answer to the e-quid “Epigastric pain with sudden onset’’. Diagn Interv Imaging 94(6): 663-666.
-
Mathias J, Phi I, Bruot O, Ganne PA, Laurent V, Regent D (2008) Hernies internes. EMC radiologie et imagerie médicale : Abdominale – Digestive Nancy University Hospital, France, pp: 1-8.
-
Bruot O, Laurent V, Tissier S, Meyer-bisch L, Barbary C, et al. (2007) Une hernie interne du caeco-colon ascendant via le hiatus de Winslow explorée en coloscanner à l’eau. J Radiol 88: 393-396.
-
Denost Q (2016) La Lettre de l’Hépato-gastroentérologue. Occlusive syndrome and internal hernia 19.
-
Lê. P, El Braks R, Ramaheriarison Y, Billey C (2008) Une hernie rétro-cæcale, Feuillets de Radiologie 48(1): 35- 38.
-
Pessaux P, Tuech JJ, Derouet N, Du Plessis R, Ronceray J, et al. (1999) Internal hernia: a rare cause of intestinal obstruction. A propos of 14 cases. Ann Chir 53(9): 870- 873.
-
Yen CH, Chen JD, Tui CM, Chou YH, Lee CH, et al. (2005) Internal hernia: computed tomography diagnosis and differentiation from adhesive small bowel obstruction. J Chin Med Assoc 68(1): 21-28.
-
Adamou H, Habou O, Adakal O, Magagi IA (2015) Supra bladder internal hernia, a rare cause of acute intestinal obstruction Pan Afr Med J 21: 14.
-
Saravanan B, Paramu MK, Ranganathan E (2008) Supravesical hernia--a rare cause of intestinal obstruction. Int J Surg 6(6): 471-472.
-
Peru N, Jouvin I, Pocard M (2020) Acute small bowel obstruction due to a right paraduodenal hernia resulting from mesenteric malrotation, Journal de Chirurgie Viscérale 157(3): 218-219.
-
Kotobi H, Echaieb A, Gallot D (2005) Surgical treatment of uncommon intra abdominal hernias. EMC – Chirurgie 2(4): 425-439.
-
Brunschweiler B, Ainseba Daoud M, Serot MC, Mauvais F (2005) Ileocecal herniation through the foramen of Winslow: a case report. Annales de Chirurgie 130(5): 346-349.
-
Harissou Adamou, Habou O, Adakal O, Magagi IA (2015) Hernie interne supravésicale, cause rare d’occlusion intestinale aiguë. Pan African Medical Journal 21: 14.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review