Liver Surgery Outcomes: Early Experience of a Highly Trained Group in a Low-Income Country
Background: The aim of this study is to analyze the morbidity and mortaslity rates among patients undergoing hepatic resections at a tertiary healthcare center in the city of Cuenca, Ecuador. A surgical team with formal training in hepatopancreatobiliary (HPB) surgery performs these surgeries. Study Design: A retrospective descriptive cross-sectional study was performed over time between 2017 and 2022 at the Hospital Jose Carrasco Arteaga, in which all patients who underwent liver resection during a 5-year period were included. The variables used were: I. Demographic data variables (age, sex, BMI, cirrhotic, ASA), II. pre-surgical diagnosis variables, III. Intraoperative and postoperative outcome variables (complications, blood loss, time in the operating room, etc.). Outcomes: A total of 38 liver resections were identified, of which 26.3% were male and 73.7% were female. Mean age: 60.5 years. Of the patients, 31.6% were reoperated, 23.7% were readmitted to the hospital, and 18.4% required a trans-operative blood transfusion. The surgical time averaged 290 minutes. The most common reason for surgery was hepatocarcinoma (23.68%), followed by intrahepatic cholangiocarcinoma (ICC) (13.15%). Morbidity was 23,68%, corresponding to Clavien Dindo 3B or higher. The 90-day mortality rate was 5.25%. Conclusions: According to the results obtained during the period from 2017 to 2022 at Hospital Jose Carrasco Arteaga, the implementation of hepatic resections has been demonstrated to be a safe and effective procedure, characterized by low rates of mortality and morbidity.
Introduction
Liver cancer is considered one of the most common malignant neoplasms worldwide, with an incidence of 841,080 cases in 2018 [1] and 905,700 new cases in 2020 [2]. The standardized incidence and mortality rates per 100,000 people per year were 9.5 for incidence and 8.7 for mortality [2]. It is one of the leading causes of death, with more than 800,000 deaths annually globally [3]. In Ecuador, according to the World Health Organization (WHO) data published in 2020, liver cancer is the tenth most common, with 5.8% annual mortality and a prevalence of 5.07 per 100,000 inhabitants. Worldwide, the incidence of males is 4.7 per 100,000 inhabitants, and that of females is 4.6 per 100,000 [4]. On a global scale, hepatocellular carcinoma (HCC) accounts for approximately 75% of liver neoplasms, while intrahepatic cholangiocarcinoma (ICC) is responsible for 10–15% of primary liver cancers [5, 6]. However, there is a significant variation in the incidence patterns of liver cancer due to various etiologies worldwide [5].
Recent research has identified a significant increase in the incidence of primary liver cancer, which has a significant impact on both patient health and health systems at the national and international levels, with surgery, hepatectomy, or transplantation being the pillar of treatment for most patients diagnosed with this liver neoplasm [5, 6]. Over the past 20 years, liver surgery has undergone significant changes due to medical innovations and surgical procedures. Due to the significant technological advancements made by the pioneers in the previous century, hepatectomies have become widely used all over the world and have proven to be safe [1, 7]. This is why mortality and morbidity in the perioperative period have been reduced and the likelihood of long-term survival increased [1, 3].
At the Hospital Jose Carrasco Arteaga, demographic information is available to examine both short-term outcomes and long-term survival after all surgical procedures, using the MIS AS 400 system of the Ecuadorian Institute of Social Security. The aim of the present study was to analyze the morbidity and mortality of patients who underwent liver surgeries at the Hospital Jose Carrasco Arteaga during the period from 2017 to 2022, the same information that is put into their hands in the following paper.
BMI Normal 31.6% Overweight 44.70% Obese GI 18.40% Obese GII 53.40% cirrhotic 5 (13.2%) Child A 100% Steatosis 23.70% ASA I 13.15% II 57.89% III 26.31% IV 2.63% Approach Conventional 31 -81.30% Operation time mean 290 min ± 109.7 min Postoperative bleeding mean 225 ml ± 529 ml _
Material and Methods
The study looked back over a period of time (2017– 2022) and used a database to store information about each patient’s medical history. This information came from the MIS AS 400 system at the Hospital Jose Carrasco Arteaga, which is part of the Ecuadorian Institute of Social Security. A total of 48 patient records were found, and after applying the inclusion and exclusion criteria, the sample for analysis was made up of 38 cases.
Inclusion Criteria: • Patients who had any liver resection, with benign or malignant pathology within resectability criteria.
Exclusion criteria:
- Unresectable patients determined at laparoscopy or initial laparotomy.
- Patients who did not complete their hospitalisation at the hospital centre due to lack of data.
- Resections for adenocarcinoma of the gallbladder.
Results
A total of 38 patients met the inclusion criteria (Table 1); the average age at the time of resection was 60.5 ± 13.37 years, with 10 (26.3%) males and 28 (73.7%) females. The BMI of the submitted patients was classified as normal (31.6%), overweight (44.7%), obese grade 1 (18.4%), and obese grade 2 (53.4%). Of the 38 patients interviewed, 5 (13.2%) had cirrhosis, and all were on scale A in Child Pugh (100%). As for comorbidities, hepatic steatosis occurred in 23.7% of patients: first-degree ASA (13.15%), second- degree (57.89%), third-degree (26.31%), and fourth-degree (2.63%). The type of surgical approach was conventional in 31 (81.3%) patients and laparoscopic in 7 (18.7%) patients. As for the peri-operative results, the average surgical time was 290 minutes, ±109.7.
Total Patients n. 38 Mean age (years) 60.5 ± 13.37 Male 10 (26.3%) Female 28 (73.7%)
| Postoperative transfusion | 7 (18.4%) | _ | _ |
|---|---|---|---|
| Bleeding greater than 1000ml | 4 (10.5%) | _ | _ |
| Re Interventions | 12 (31.6%) | _ | _ |
| Hospital readmissions | 9 (23.7%) | _ | _ |
| Mortality at 90 days | 2 (5.26%) | _ | _ |
Table 1: Demographic data.
The average transoperative bleeding is 225 ml ± 529 ml. Of the 38 patients treated, 7 (18.4%) needed post-surgical blood transfusions, 4 (10.5%) had bleeding greater than 1000 ml, 12 (23.7%) needed reintervention, 9 (23.7%) needed re- hospitalization, and 2 (5.26%) had 90-day mortality. The distribution was made by age groups (Table 2), including 2 (5.26%) patients under the age of 30, 41 to 50 years old, 11 (28.94%) patients, 51 to 60 years old, 6 (15.78%) patients, 61 to 70 years old, 11 (28.94%) patients, and over 70 years of age, for a total of 8 (21.05%) patients.
| Age Group | n | % |
|---|---|---|
| Under 30 Years Old | 2 | 5.26 |
| 41 A 50 Years Old | 11 | 28.94 |
| 51 A 60 Years Old | 6 | 15.78 |
| 61 A 70 Years Old | 11 | 28.94 |
| More than 70 Years Old | 8 | 21.05 |
| Total | 38 | 100 |
Table 3: Distribution of patients by age groups.
According to the Brisbane classification, the resections performed were ordered and obtained: hepatectomies bisegmentectomy 8 (21.05%), right hepatectomy 10 (26.31%), right hepatectomy plus segmentectomy 1 (2.63%), right extended hepatectomy 1 (2.63%), left hepatectomy 5 (13.15%), left hepatectectomy plus segmentectomy 3 (7.89%), extended left hepatectomy 1 (2.63%), left side sideectomy 2 (5.26%), and segmentectomy 7 (18.42%). The Clavien-Dindo classification was used which is a system used to classify complications in a standardized manner [8] that may arise after surgery (Table 3), 24 (63.15%) were classified as II, 5 (13.15%) III A, 7 (18.42%) as III B, 1 (2.63%) as IV A and 1 (2.63%) as V.
| Clavien Dindo | n | % |
|---|---|---|
| II | 24 | 63,15 |
| III A | 5 | 13,15 |
| III B | 7 | 18,42 |
| IV A | 1 | 2,63 |
| V | 1 | 2,63 |
| Causes of Hospital Readmission | n | % |
| Ascites | 1 | 12,5 |
| Colon Cancer | 1 | 12,5 |
| Wound Dehiscence | 1 | 12,5 |
| Wound Infection | 2 | 25 |
| Lung Tumor | 1 | 12,5 |
| Pneumonia | 1 | 12,5 |
| Liver Failure | 1 | 12,5 |
Table 4: Complications according to classification Clavien Dindo
As for the postoperative complications (Table 4), a total of 2 (11.76%) were obtained of stress ascites, 1 abdominal stretch (5.88%), 3 liver abscesses (17.64%), 1 wound dehiscence (5. 88%), 1 intra-abdominal collection (5,88%), 1 surgical site infection (5. 1988%), 1 anemia (5. 188%), 1 pleural stroke (5.-88%), 1 hemorrhage (5.89%), 1 pneumonia (5.86%), 1 atelectasia (5.188%), 1 IVU (5.85%), 1 sepsis (5.888%), and 1 neumotorax (5.87%).
| Complications | n | % |
|---|---|---|
| Tension Ascites | 2 | 11,76 |
| Abdominal Distension | 1 | 5,88 |
| Liver Abscess | 3 | 17,64 |
| Wound Dehiscence | 1 | 5,88 |
| Intra-Abdominal Collection | 1 | 5,88 |
| Surgical Site Infection | 1 | 5,88 |
| Anemia | 1 | 5,88 |
| Pleural Effusion | 1 | 5,88 |
| Bleeding | 1 | 5,88 |
| Pneumonia | 1 | 5,88 |
| Atelectasis | 1 | 5,88 |
| UTI | 1 | 5,88 |
| Sepsis | 1 | 5,88 |
| Pneumothorax | 1 | 5,88 |
Table 2: Description of complications.
Causes of re-intervention in patients undergoing treatment (Figure 2) were biliary stenosis 1 (8.33%), intra-abdominal collection 5 (41.66%), wall dehiscence 2 (16.66%), wound infection (8.33%), oblitoma 1 (8.33%), and hemoperitoneum 2 (16.66%). As for the re-entry of patients after they were discharged (Table 5), a total of 1 ascites (12.5%), 1 colon cancer (12.5%), 1 wound dehiscence (12.5%), 2 wound infections (25%), 1 lung tumor (12.5%), 1 pneumonia (12.5%), and 1 liver failure (12.5%) were collected.
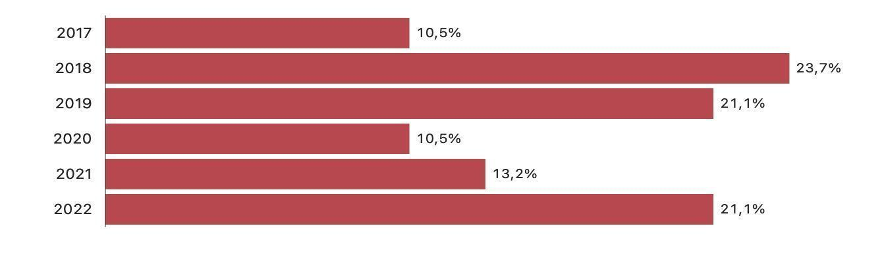
In 2017, a total of 10.5% of surgeries were hepatectomies, followed by a notable increase to 23.7% in 2018. Subsequent years witnessed fluctuations, with percentages ranging from 10.5% in 2020 to 21.1% in both 2019 and 2022. Variations in the total number of hepatectomies across years may reflect changes in healthcare priorities, funding allocations, or the prevalence of conditions necessitating liver resection surgeries in low-income regions.
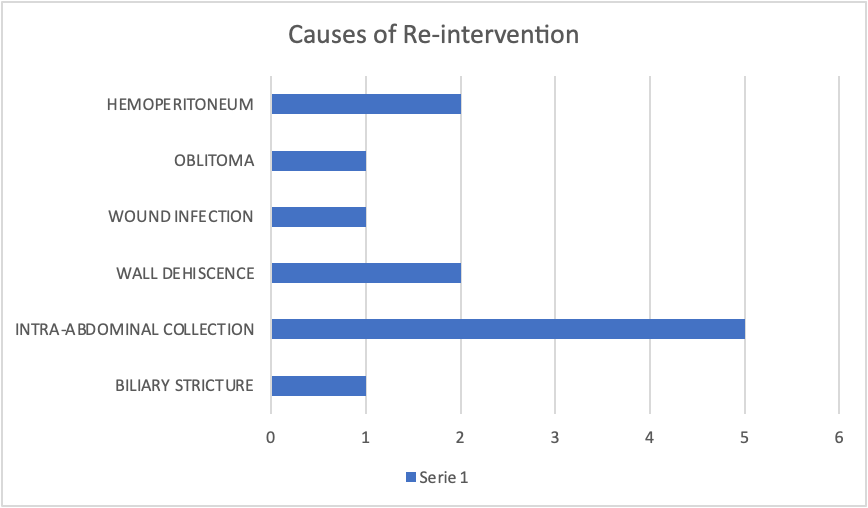
Figure 2: Complications Requiring Surgery Following Hepatectomy. The data are based on a study involving 38 patients, with 12 individuals requiring surgery for postoperative complications. Complications and Incidence: Hemoperitoneum: 2 cases (16.7%), Oblitoma: 1 case (8.3%), Wound infection: 1 case (8.3%), Wall dehiscence: 2 cases (16.7%), intra-abdominal collection: 5 cases (41.7%) and billiard stricture: 1 case (8.3%). Intra-abdominal collection emerged as the most common complication, accounting for 41.7% of cases requiring surgical intervention among the study cohort.
Understanding the incidence and nature of these complications is crucial for optimizing patient care and improving outcomes in post-hepatectomy management.
The distribution of hepatectomies performed annually from 2017 to 2022 fluctuated significantly (Figure 1). In 2018, there was a notable surge, with hepatectomies comprising 23.7% of all surgeries, while in 2020 and 2021, the percentages dropped to 10.5% and 13.2%, respectively. However, by 2022, the proportion rose again to 21.1%, mirroring the figures observed in 2019. These fluctuations highlight dynamic trends in surgical practices over the six- year period, reflecting changes in medical protocols and patient demographics.
Discussion
In our study, we had a final sample of 38 patients, and the data obtained in the 5 years of the hepatectomies performed were analyzed. It was fundamental to know the morbidity and mortality of the patients undergoing hepatectomies and the influence of the different perioperative and demographic factors. In the study of Sucandy et al., they divided 831 patients by age into three groups: A, B, and C. In which, group A included persons under the age of 70; in group B, persons between the ages of 70 and 79; and in group C, persons over or equal to 80 years of age. Groups B and C were associated with higher comorbidities and high ASA, along with more postoperative complications. However, despite higher preoperative comorbidities and ASA scores, there was no significant increase in postoperative morbidity after minimally invasive liver resection in patients ≥ 70 years of age [9].
According to our study, the majority of the patients interviewed were between the ages of 61 and 70 (28.94%), 41 to 50 (2.8.94%), and 70 (21.05%), indicating a higher prevalence in adult patients under the age of 70. However, in our study, the morbidity in these patients was also relatively low. In Germany, a total of 110.332 liver resections were performed between 2010 and 2015, with an intra-hospital mortality rate of 5.8%. Mortality varied depending on age: 2.2 percent in patients under the age of 50 years, 4.3 percent for patients between the ages of 50 and 69 years, and 8.8 percent among patients older than 69 years was the highest risk and mortality group [10].
However, the combination of population aging and advances in perioperative care has made surgery more frequently performed in older patients and even in elderly patients with various complications. If adequate perioperative care is provided, safe and radical surgery can be performed in patients with HCC 80 years of age or older [11]. Age itself is not considered a risk factor, but what should be taken into account in old age are comorbidities, the Child Pugh scale in patients with cirrhosis, the extent of liver injury, and the quality of both surgery and perioperative care.
Schiergens TS, et al. [12] suggest that age does not affect the long-term survival of patients undergoing primary or secondary liver resections; however, the results of broader observational studies indicate a substantially higher perioperative risk for patients who are of advanced age. This can be explained because they do not tolerate well the stress of a major surgery due to a decrease in physiological reserves and the concomitance of underlying medical diseases [12]. Regarding gender, Nagata et al. mentioned that females are predisposed to more comorbidities, noting that more caution should be given to this sex in perioperative care [12].
In our study, 73.7% of patients were female, while 26.3% were male. The loss of intraoperative blood is crucial to its prognosis; according to Suh SW [13] intraoperative blood loss is greater in obese patients than in non-obese patients. Keep in mind that this could be because people with a higher body mass index have higher ventilation pressure, which changes the flow of veins in the liver and makes it easier for bleeding to happen when the liver parenchyma is cut [13]. Obese patients are at greater risk of bleeding because they have hepatic steatosis, with or without steatohepatitis, which makes the liver tissue more fragile, which promotes blood loss during resection and puts the patient’s life at risk, thus giving poor early postoperative results [13].
Throughout our examination, we obtained a higher prevalence of obesity (53.4%), along with steatosis (23.7% of all patients undergoing treatment) and 13.2% of patients with cirrhosis. Hepatectomies in cirrhosis patients were considered to be a high-risk procedure; however, the rates of morbidity and per-operative mortality have decreased over the last 20 years, and a reduction in blood loss during hepatic resection has been achieved. At present, morbidity rates remain a problem in patients, demonstrating ascites as a frequent postoperative complication among these patients. Our study affirms this, with ascites being the second most common complication (11.76%), and 13.2% of patients are cirrhotic [14].
The Child-Pugh score system was proposed to predict mortality in patients with cirrhosis, originally conceived in 1964 by Child and Turcotte, and was carried out to guide the selection of patients who would benefit from optional portal decompression surgery. This category divides patients into three categories: A, who has good liver function; B, who has moderately impaired hepatic function; and C, who has advanced liver dysfunction. It is recommended to operate only on Child-Pugh A in cirrhotic patients, as 100% of our patients have cirrhosis with Child [15].
According to the guidelines of the European Liver Study Association (EASL), the American Association for the Study of Liver Diseases (AASLD), and the National Comprehensive Cancer Network (NCCN), following the liver cancer system of the Barcelona Clinic [BCLC], only patients in stage A on the Child Pugh scale are resectable [16]. That’s why, in our study, all our cirrhosis patients were within the Child Pugh A scale. The value obtained from the American Society of Anesthesiologists (ASA) scale is critical for prognosis.
According to Longchamp G, et al. [17] the ASA value should be considered an independent predictor of postoperative comorbidities. The fact that these patients frequently experience significant blood loss and require blood transfusions explains why ASA values greater than or equal to 3 are significantly more likely to result in higher morbidity rates [17].
In our study, the prevalence of patients undergoing ASA II was the highest, being favorable for their prognosis; however, ASA III was 26.31%, with a greater tendency to perioperative comorbidities.
Currently, surgery has made significant advances in addressing hepatectomies, with options such as robotic, laparoscopic, or open. According to Wang et al., the laparoscopic approach has many advantages compared to the conventional approach. Less hospitalization and fewer postoperative complications can be highlighted. In turn, it mentions that for patients over the age of 65, a laparoscopic approach is indicated, especially for HCC [18]. In this study, the conventional or open approach was greater with 81.3% compared to the laparoscopic approach, which was 18.7%, and HCC was the most diagnosed with 23.68%. Surgery time is linked to the morbidity of patients undergoing hepatectomies because prolonged surgical time negatively affects the results and is independently associated with postoperative infectious complications and a longer hospital stay [18].
Operating time was an average of 290 minutes, with a standard deviation of ±109.7 minutes. Which is a long time; however, the laparoscopic approach compared to the conventional is longer. Many ways have been thought of to keep blood loss as low as possible during hepatectomies, since large amounts of blood loss are linked to higher rates of illness, death, and tumor recurrence in people with primary liver cancer who are having hepatectomies. Risk factors for major bleeding are tumor size, serum creatinine, clinically significant portal hypertension, and major hepatectomy [18]. The smallest bleeding in our study was 89.5%, while the larger bleeding was 10.5%, thus showing low ranges in bleeding. Red
blood cell transfusion increases the risk of major complications in patients undergoing hepatectomies [19, 20].
According to Postlewait, et al. [21] the patients who underwent a major hepatectomy and needed blood transfusions had greater complications and a higher risk of re-entering in 90 days [21]. In our study, 18.4% needed transoperative blood transfusions; this is another parameter of morbidity. In Montalti, et al. [22] most recent study comparing robotic surgery with laparoscopic surgery, they mention that there are different variables that define the perioperative prognosis, including the surgical approach, sex, comorbidities, previous surgeries, ASA, and tumor size, among others. In our study, we were able to observe that the morbidity was 23.68%, a slightly high figure. This could be explained by the variables already analyzed, such as the greater open approach and sex, among others.
The main etiologies of liver cancer are the hepatitis B virus (HBV), the hepatitis C virus (HCV), alcohol consumption, and non-alcoholic steatohepatitis. Chronic infection with the hepatitis C virus and the hepatitis B virus has been the leading cause of liver cancer, with HCC predominating [23]. However, increased vaccination coverage against the hepatitis B virus with antiviral therapy has reduced the incidence of HBV-associated liver cancer in some countries. Since 2014, safe and effective oral antivirals have been available for HCV, which reduces the risk of HCC [23, 24]. In our study, we observed that the etiology was equitable, as was HCV, alcoholic, medicinal, autoimmune, and idiopathic.
Advances in surgical technique, patient selection, and perioperative care have significantly reduced surgical mortality to 1-3% in experienced centers [25]. In our study, we were able to observe a low mortality rate of only 5.26%, thanks to perioperative care and the experience and knowledge of the group of highly specialized surgeons. Hepatectomy is the most important part of both primary and secondary liver tumor treatments. It has better long-term oncological outcomes than other medical or interventional treatments in a number of hepatobiliary and oncologic conditions [26, 27].
The nature of the lesion and its location in the liver, along with the anatomy of the patient and the volume and quality of liver tissue remaining after resection, should be taken into account to ensure adequate future liver residue [28]. Most of the time, major liver resections are needed to get the best treatment for both cancerous conditions like HCC, cholangiocarcinoma, and other rare types of cancer, as well as benign primary liver tumors like giant hemangiomas and adenomas [26]. These are associated with increased morbidity and post-operative mortality due to postoperative liver failure [27].
Liver resection and liver transplantation are the main curative options for HCC and various malignant neoplasms of the liver, which offer a 70% higher survival rate than 5 years. [28]. Hepatectomy, unlike liver transplantation, can get rid of the main tumor, but there are still risks of chronic liver disease and micrometastases that can’t be seen [14, 15]. Hepatectomy is currently a very well-liked curative procedure because the availability of donors limits the use of liver transplants [28]. Most of the time, problems that happen after liver resection are infections from venous catheters, pleural strokes, incisional infections, atelectasia, pneumonia, ascites, urinary infections, intraperitoneal hemorrhage, gastrointestinal bleeding, biliary tract hemorrhoids, coagulation disorders, bile leakage, and liver failure. Liver failure is the most serious complication after liver resection and can be life-threatening [26].
The Clavien-Dindo classification can be used to measure postoperative morbidity. A major complication is defined as one that is greater than IIIA [29]. The incidence of postoperative complications in obese patients is higher than in non-obese patients. Infection of the wound and hernia of the abdominal wall are frequent complications. In turn, this leads to a longer hospital stay in the group of obese patients [20].
Perioperative blood transfusion has been associated with increased morbidity post-hepatectomy. This is due to the combination of surgical stress and blood transfusion, which can lead to synergism by activating the immune system through the release of inflammatory cytokines. The most common serious morbidities in blood transfusions were posthepatectomy liver failure and bile leakage [18].
The utilization of the Clavien-Dindo classification played a crucial role in the assessment of the morbidity associated with hepatectomies, obtaining a 63.15% in II showing that hepatectomies are safe and effective, followed by an 18.42% IIIB and 13.15% IIIA. The mortality rate for benign liver tumors is low, at 4.5%. Compared to cancerous tumors, these happen more often: 9.3% of people who get cancer of the liver or intrahepatic biliary tract die from it, and 14.6% of people who get perihilar cholangiocarcinoma die from it. Extrahepatic cholangiocarcinoma is the type of cancer that causes the most deaths across all major resection types, with rates of 13.5% for a left hepatectomy, 28.8% for a right hepatectomy, 23.1% for major resections, and 26% for enlarged resections [10].
As for the difference between minor and major hepatectomies, according to Fillman et al., anatomical resections produced a hospital mortality rate of 3.8% compared to these minor, segmentary, and bisegmentary resections. Compared to the larger resections, which have a hospital mortality rate of 10.4%, there is a significant difference in mortality between left and right hepatectomy, with 6.2% for left and 10.7% for right. However, in our study, the highest mortality rate was for enlarged resection with biliodigestive anastomosis, at 25.5% [10].
Of a total of 38 cases, 23 were major resections, with 95.65% being open and 4.35% laparoscopic. While 17 resections were minor, a total of 64.71% were open, and 35.39% were laparoscopic, which clearly indicates that the minimum invasion in liver surgery at the moment is preferred by the group for minor resections (segmentectomies, preferably on the left side of the liver). Mortality at 90 days is considered a key indicator for short-term perioperative results in liver resections [11]. It has been seen that hepatectomies have a low short-term mortality rate of 5.3%. It has been determined that blood transfusions can increase mortality up to seven times more than in patients who did not receive them [27]. In the field of liver surgery, huge advances have been made in the last 50 years.
In many liver disease treatment centers, liver resection is a common practice due to its notable improvement in effectiveness and safety. Indications for hepatectomies have increased, and perioperative care has improved. Advances and improvements in preoperative evaluations, imaging, patient selection, operational techniques, and intensive care management have reduced morbidity and mortality. The results of the treatment of patients with hepatic resections have improved with a multidisciplinary approach. In our study, we verified that hepatectomies are an effective and safe treatment for the Ecuadorian population, showing good results.
Acknowledgements
We are very grateful to the people at the centers who gave us the permissions and patient information to be able to carry out this research.
Conflict of Interest Statement
None of the authors have any conflicts of interest.
Authors Contributions
All the authors participated in equally parts in the study design, data collection, outcomes and discussion.
References
-
Gilg S, Sparrelid E, Isaksson B, Lundell L, Nowak G, et al. (2017) Mortality-related risk factors and long- term survival after 4460 liver resections in Sweden—a population-based study. Langenbecks Arch Surg 402(1): 105-113.
-
Thornblade LW, Shi X, Ruiz A, Flum DR, Park JO (2017) Comparative effectiveness of minimally invasive surgery and conventional approaches for major or challenging hepatectomy. J Am Coll Surg 224(5): 851-861.
-
Vonlanthen R, Lodge P, Barkun JS, Farges O, Rogiers X, et al. (2018) Toward a consensus on centralization in surgery. Ann Surg 268(5): 712-724.
-
WHO (2020) International Agency for Research on Cancer, Ecuador, Globocan.
-
Liu Z, Jiang Y, Yuan H, Fang Q, Cai N, et al. (2019) The trends in incidence of primary liver cancer caused by specific etiologies: Results from the Global Burden of Disease Study 2016 and implications for liver cancer prevention. J Hepatol 70(4): 674-683.
-
Tsilimigras DI, Sahara K, Moris D, Mehta R, Paredes AZ, et al. (2020) Assessing textbook outcomes following liver surgery for primary liver cancer over a 12-year time period at major hepatobiliary centers. Ann Surg Oncol 27(9): 3318-3327.
-
Kokudo N, Takemura N, Ito K, Mihara F (2020) The history of liver surgery: Achievements over the past 50 years. Ann Gastroenterol Surg 4(2): 109-117.
-
Clavien PA, Sanabria JR, Strasberg SM (1992) Proposed classification of complications of surgery with examples of utility in cholecystectomy. Surgery 111(5): 518-526.
-
Sucandy I, Cheek S, Tsung A, Marsh JW, Geller DA (2018) Minimally invasive liver resection for primary and metastatic liver tumors: influence of age on perioperative complications and mortality. Surg Endosc 32(4): 1885- 1891.
-
Filmann N, Walter D, Schadde E, Bruns C, Keck T, et al. (2019) Mortality after liver surgery in Germany. Br J Surg 106(11): 1523-1529.
-
Lei GY, Shen L, Junnarkar SP, Huey CT, Low J, et al. (2021) Predictors of 90-day mortality following hepatic resection for hepatocellular carcinoma. Visc Med 37(2): 102-109.
-
Schiergens TS, Lindenthaler A, Thomas MN, Rentsch M, Mittermeier L, et al. (2016) Time-dependent impact of age and comorbidities on long-term overall survival after liver resection. Liver Int 36(9): 1340-1350.
-
Suh SW (2022) Influence of obesity and fluid balance on operative outcomes in hepatic resection. J Pers Med 12(11): 1897.
-
Harimoto N, Araki K, Ishii N, Muranushi R, Hoshino K, et al. (2020) Predictors of postoperative ascites after hepatic resection in patients with hepatocellular carcinoma. Anticancer Res 40(8): 4343-4349.
-
Tsoris A, Marlar CA (2023) Use of the Child Pugh score in liver disease. StatPearls Publishing.
-
Chen X, Lai L, Ye J, Li L (2021) Downstaging therapies for unresectable hepatocellular carcinoma prior to hepatic resection: A systematic review and meta-analysis. Front Oncol 11: 740762.
-
Longchamp G, Labgaa I, Demartines N, Joliat GR (2021) Predictors of complications after liver surgery: a systematic review of the literature. HPB (Oxford) 23(5): 645-655.
-
Wang Q, Li HJ, Dai XM, Xiang ZQ, Zhu Z (2022) Laparoscopic versus open liver resection for hepatocellular carcinoma in elderly patients: Systematic review and meta-analysis of propensity-score matched studies. Int J Surg 105: 106821.
-
Cannon RM, Brown RE, St Hill CR, Dunki-Jacobs E, Martin RCG, et al. (2013) Negative effects of transfused blood components after hepatectomy for metastatic colorectal cancer. Am Surg 79(1): 35-39.
-
Hallet J, Mahar AL, Nathens AB, Tsang ME, Beyfuss KA, et al. (2018) The impact of perioperative blood transfusions on short-term outcomes following hepatectomy. Hepatobiliary Surg Nutr 7(1): 1-10.
-
Postlewait LM, Squires MH, Kooby DA, Weber SM, Scoggins CR, et al. (2016) The relationship of blood transfusion with peri-operative and long-term outcomes after major hepatectomy for metastatic colorectal cancer: a multi-institutional study of 456 patients. HPB (Oxford) 18(2): 192-199.
-
Montalti R, Giglio MC, Wu AGR, Cipriani F, D’Silva M, et al. (2023) Risk factors and outcomes of open conversion during minimally invasive major hepatectomies: An international multicenter study on 3880 procedures comparing the laparoscopic and robotic approaches. Ann Surg Oncol 30(8): 4783-4796.
-
Huang DQ, Singal AG, Kono Y, Tan DJH, El-Serag HB, et al. (2022) Changing global epidemiology of liver cancer from 2010 to 2019: NASH is the fastest growing cause of liver cancer. Cell Metab 34(7): 969-977.
-
Dang H, Yeo YH, Yasuda S, Huang CF, Iio E, et al. (2020) Cure with interferon-free direct-acting antiviral is associated with increased survival in patients with hepatitis C virus-related hepatocellular carcinoma from both east and west. Hepatology 71(6): 1910-1922.
-
Kulik L, El-Serag HB (2019) Epidemiology and management of hepatocellular carcinoma. Gastroenterology 156(2): 477-491.e1.
-
Ju M, Yopp AC (2019) The utility of anatomical liver resection in hepatocellular carcinoma: Associated with improved outcomes or lack of supportive evidence. Cancers (Basel) 11(10): 1441.
-
Fagenson AM, Pitt HA, Lau KN (2022) Perioperative blood transfusions or operative time: Which drives post- hepatectomy outcomes. Am Surg 88(7): 1644-1652.
-
Nagata M, Hara Y, Hayakawa S, Komura H, Shibata J, et al. (2020) Retrospective study of predictive factors for postoperative complications of hepatectomies lasting 12 or more hours. Fujita Med J 6(3): 59-66.
-
Imai D, Maeda T, Wang H, Shimazaki T, Sanefuji K, et al. (2021) Risk factors for and outcomes of intraoperative blood loss in liver resection for hepatocellular tumors. Am Surg 87(3): 376-383.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review