Contextual Interference Effect in Learning of Simulated Laparoscopic Tasks
Laparoscopy, a minimally invasive surgical technique involving fine motor movements of the hands and fingers, has proven to be an invaluable tool in surgical care. Expediting the learning process of surgeons to reach proficiency in this surgical technique directly impacts patient outcomes, recovery times, and time management in hospitals [1]. Within motor learning, blocked and random practice has been identified as having correspondingly low or high levels of contextual interference, with different effects on learning and retention of motor skills. Contextual interference can be described as the level of mental interference created during the practice of motor skills. So far, research has been equivocal in identifying the best practice schedule for optimizing the acquisition and retention of fine and gross motor skills. This study examines the role of contextual interference in the acquisition, short-term retention (10-minute), and long-term retention (10-day) of three variations of a simulated laparoscopic task in 60 adults aged 18-65, 30 males and 30 females. The index of performance was represented by the total time taken to complete each task using curved laparoscopic graspers. Results showed that both blocked and random practice groups significantly improved acquisition performance over 54 acquisition trials. Participants undergoing a blocked practice schedule improved their pattern time-to-completion by 46%, retaining most of their performance in the 10-minute retest while maintaining their skill as well after 10 days. The random practice group improved acquisition performance by 38%, maintaining most of their performance in the short-term retention test, with only a slight decrease in speed in the long-term retention test. No statistically significant differences in the efficiency of blocked versus random practice schedules were found for both acquisition and retention, suggesting that both practice schedules can be viable options for learning and retention of simulated laparoscopic surgical tasks. We suggest tailoring training programs to individual skill levels to provide each learner with the optimal amount of contextual interference to reach their optimal challenge point according to subjective task difficulty experienced.
Introduction
Motor learning and control theory provides the basis for determining the optimal practice schedule for the acquisition, retention, and transfer of motor skills [2]. Laparoscopic surgery, an advanced, minimally invasive, surgical technique using tiny video cameras inserted through small incisions into the bodily cavities, has been gaining attention and popularity among motor learning researchers in recent decades [3]. This surgical technique requires precise motor control, coordination, and fine motor skills achieved through countless hours of practice. The benefits of laparoscopy are immense, as it allows a much less invasive surgical procedure compared to traditional open surgery.
Laparoscopic surgery consists of using two or more small (1 cm) incisions to access the abdomen or pelvis. A trochar (tube), which includes a removable borer with a sharp tip to cut through tissue beyond the skin inside a cannula to serve as a portal, is inserted through the incisions to create small ports into the abdomen to allow access for instruments. Trochars often include a valve mechanism to allow for insufflation with carbon dioxide gas to create a larger working space and to view the area more clearly. A long rod consisting of a high-resolution camera (laparoscope) with a high-intensity light source is inserted through one incision and smaller, long narrow instruments are inserted through the other incisions to allow viewing and manipulating the anatomy and tissues. The camera transmits a video feed to nearby monitors beside the patient’s body to allow the surgeons to see inside the patient’s body while operating [3].
Laparoscopic technology has many benefits. Since the surgical incisions are smaller than in open surgery, laparoscopic surgery offers improved recovery outcomes for patients and reduces the risks associated with surgery. The smaller incisions tend to heal faster and cause less discomfort for the patient, which in turn helps patients return to regular activity sooner after surgery. This effect is emphasized in patients over 50 years of age, who usually take longer to recover from open surgery than younger patients, due to the presence of comorbidities and lower tolerance of surgical stress [4]. Additionally, laparoscopic surgery can have less of an impact on other aspects of patient well-being. Laparoscopic surgery usually results in more aesthetically pleasing scars than the long incisions made in traditional surgery, which can benefit the psychological health of patients. The shorter recovery times associated with laparoscopic surgery also allow patients to return to work quicker, which can reduce financial strain.
Considering the financial burden of surgeries, particularly in the context of the publicly-funded Canadian health system, laparoscopic surgery has been shown to be superior to traditional open surgery. While the laparoscopic procedure itself is more expensive, the minimally invasive nature usually results in less pain and shorter stays in the hospital. As each day of stay in the hospital incurs a cost, the shorter post-operative stay in the hospital decreases the overall cost per surgical patient. The resulting cost of laparoscopy was found to be lower by multiple studies [5, 6]. In England, the increased use of laparoscopic colon cancer surgery between 2006 and 2012 helped save £29.3 million (almost CAD$50 million) for the National Health Service [6].
Overall, laparoscopy is a great advancement in the surgical field, and efficient training practices should be implemented in medical residencies and fellowship programs. Unlike sports performance, where motor learning research has historically focused, a single mistake in the production of a movement in surgery may cause significant injury or fatality in the patient. Identifying the optimal practice schedule for improving laparoscopic skills may assist medical education programs in optimizing the learning and application of laparoscopic surgical skills to improve operating room efficiency and patient outcomes.
This called for an analysis of the literature and obtaining experimental evidence to determine the best practice schedule for the development of laparoscopic surgical skills in the least amount of time.
Review of Literature and Rationale
The two most widely studied practice schedules are blocked and random practice, both characterized as being on the extreme opposite ends of the contextual interference continuum [7]. Blocked practice, practicing similar movement tasks in succession before moving on to the next class of movements, creates the least amount of contextual interference. Contrastingly, random practice, practicing the different variations of movement often of differing levels of difficulty in a random order, creates high levels of contextual interference during the acquisition of a complex set of motor skills. Early literature reported that random practice schedules result in poorer performance during skill acquisition, but improved retention and transfer [8]. Retention, defined as the recreation of similar levels of obtained performance in the skill after a period of inactivity, and transfer, defined as the application of learned skill to new contexts and situations, can be used as more appropriate measures of learning than performance during skill acquisition, particularly in the context of a surgical career.
Guadagnoli MA, et al. [9] as well as Shea J, et al. [2] suggested that learning can be enhanced by introducing additional information processing requirements to a task, which is most effectively done by random practice trials. Guadagnoli MA, et al. [9] introduced the idea of an OCP, the point at which the learner is exposed to an ideal amount of interpretable information, in order to maximize motor learning.
Motor tasks have two types of difficulty: nominal and functional. Nominal difficulty relates to the objective or inherent difficulty of the task. Functional difficulty is defined as the subjective or perceived difficulty of learning the task and the learner’s perceived difficulty has a greater impact on skill acquisition. Therefore, it can be inferred that increased contextual interference through random practice may bring the individual to their OCP more quickly, hence the enhanced learning and retention of skill.
According to Shea J, et al. [2] improvement in retention performance, as well as improved transfer, may be attributed to more than just increased functional difficulty of the learning trials. The authors offer an additional explanation, according to which high contextual interference in random practice forces the participants to use multiple neural processing strategies, increasing flexibility in mechanisms of motor initiation and control, and leading to improved transfer of performance to other contexts and tasks.
In the first seminal work discussing the contextual interference effect in motor movement, the experiment involved the practice of a gross motor skill, maneuvering tennis balls using the shoulder, elbow, and wrist joints to hit targets [2]. However, laparoscopic surgery is a fine motor skill activity, where the surgeons use very small degrees of movement generated solely through their wrist, hand, and finger joints. This begs the question; do practice schedules characterized by different degrees of contextual interference have the same effect on acquisition, retention, and transfer in both fine and gross motor skills? Or is random practice only beneficial for the retention and transfer of gross motor skills? Fitts PM [10] discussed the idea that precise motor movements involving the hand and fingers have a larger information capacity than more gross movements involving the arm, such as in Shea J, et al. [2] experiment, further highlighting the importance of differentiating between gross and fine motor skill experimental evidence with regard to motor learning.
A subsequent study by Hynes-Dusel JM [11] observed the contextual interference effect in motor learning of fine motor skills involving the use of chopsticks. Similarities can be seen between chopsticks and laparoscopic tools. Both of them involve small, delicate movements of the hands and fingers to manipulate long, thin “sticks” used to grasp and control relatively small objects. Hynes-Dusel JM [11] found enhanced retention and transfer of fine motor skills following blocked practice conditions, in contrast to the original view of the impact of contextual interference in learning physical skills.
Although Hynes-Dusel JM [11] found blocked practice to be superior in both short and long-term retention tests, Shea J, et al. [2] study design is more widely accepted because their research included twice as many participants compared to Hynes-Dusel’s JM [11] study (72 and 36, respectively), and a longer rest period between acquisition and long-term retention tests (10 days versus 48 hours, respectively). It is also unknown whether Hynes-Dusel recruited an equal number of male and female participants, unlike Shea J, et al. [2] who recruited equal numbers of both sexes. Shea J, et al. [2] found faster movement times in male participants, attributed to greater muscle development in those subjects.
However, their study involved gross motor skills involving large muscle groups, which are not utilized to the same extent in fine motor movements. Therefore, exploration of sex differences in laparoscopic skill acquisition and retention is warranted.
Shewokis PA, et al. [12] designed a study in which they used functional near-infrared spectroscopy to monitor changes in hemodynamics in the prefrontal cortex while third-year medical students learned and performed simulated laparoscopic tasks. The students were randomized to either a blocked or random practice schedule and their performance and cognitive effort were assessed during acquisition, retention, and transfer tests. The results showed that the random practice schedule led to better performance and less cognitive load during retention and transfer tests, as evidenced by lower total hemoglobin change in the right dorsolateral prefrontal cortex. Overall, the study suggests that random practice schedules may lead to enhanced learning compared to blocked practice schedules.
Rivard JD, et al. [13] examined the effects of blocked and random training schedules on the acquisition and retention of laparoscopic skills in 36 laparoscopic novices. Participants were randomized to either blocked, random, or no additional training, and outcomes were measured using the validated Fundamentals of Laparoscopic Surgery (FLS) and hand- motion efficiency scores. Both blocked and random groups showed significant improvement in FLS and hand-motion efficiency scores on post-tests and higher overall FLS scores on retention tests compared to controls. There was no significant difference in skill acquisition or retention between the blocked and random groups, indicating that both training schedules may be considered valid options for tailoring training to individual needs.
Research Question and Hypothesis
The goal of this study was to identify the optimal practice schedule for learning and retention of simulated laparoscopic skills, considering the contrasting findings of the current state of literature and research. Since the most critical value of simulated laparoscopic surgery tasks is the retention of performance and optimal transfer to real-world hospital environments, maintenance of similar levels of performance achieved during skill acquisition displayed through the short-term and long-term retention tests was the objective of interest. While we expected both blocked and random practice groups to improve in acquisition performance as a result of practicing the skill, we hypothesized that a random practice schedule would result in worse performance during acquisition, but better performance during short and long-term retention tests. In addition, we sought to examine sex differences in both acquisition and retention of the learned skill. We hypothesized that males and females would perform similarly, given the fine motor skill nature of the task, which does not require significant utilization of muscle mass.
Method
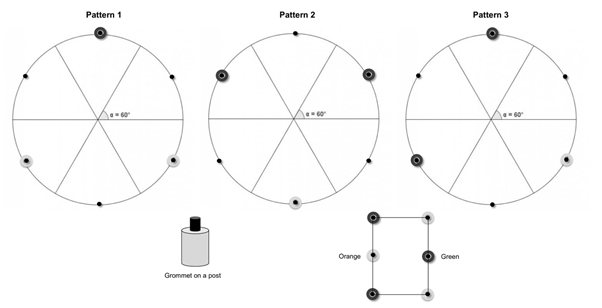
An experiment with a study design modelled on Shea J, et al. [2] was undertaken using a laparoscopic simulator (3DmedTM laparoscopic training device) and fine motor movements. Sixty adults aged 18-65, 30 males and 30 females, were recruited through posters and snowball sampling. Participants were students with no previous experience or training using the device. Participants were verbally screened for handedness, three males and two females self-identified as left-handed. One participant self- identified as colour-blind but no other visual or motor disability was found. All participants provided informed consent. The experimental procedure was approved by the University Human Research Ethics Board (HE18984) and funded by an internal university research grant. Participants were randomly assigned to either blocked practice (low contextual interference) or random practice (high contextual interference) groups. Each participant performed 54 training trials on the 3DmedTM device, consisting of 18 trials for each motor task. The tasks involved grasping and lifting three of six rubber grommets placed on six pegs on the left side of the device, transferring them to the right side of the device, and placing them onto their corresponding pegs. The task was mirrored for left- handed participants as the peg plate could be inverted. The participant could select from 6 coloured grommets either green or orange, there were three of each. These colours were chosen to accommodate colour-blind participants who identified the largest distinction between those two colours. Three different patterns were displayed on the wall directly above the 3DmedTM trainer in front of the participant at eye level (Figure 1).
Participants stood on an adjustable step platform, similar to the ones used in an operating room, so there was roughly a 90-degree angle between their upper arm and forearm. This allowed for maximal mobility.
Participants were instructed to hold two Maryland laparoscopic instruments (graspers), one grasper in each hand and to insert them into the front of the 3DmedTM trainer. They were able to see the ends of the graspers, grommets and pegs inside the trainer via a 32 GB 9.7” Apple iPad Pro that was mounted on the 3DmedTM device and used to view the board indirectly through its high-resolution video camera, which was also used to video-record each trial. As a result, the participants’ view was two-dimensional, and not three-dimensional, reducing their depth perception and simulating a laparoscopic surgeon’s view in the operating room.
At the start of each trial, the experimenter announced the pattern number, and the participant was required to use the Maryland laparoscopic instrument to grasp and lift one grommet from the rectangular starting location with the dominant hand, transfer it to the instrument held by the dominant hand, and drop the grommet onto the designated peg on the right side of the board. Each pattern required placing three grommets on three specific pegs using a specific colour (Figure 1). The blocked practice group performed 18 subsequent trials of the same peg pattern, before continuing to the next pattern.
Participants always started with pattern 1, before proceeding to pattern 2, and then pattern 3. The random practice group performed all 54 trials in the same predetermined random order, generated by a random- number generator, ensuring that each pattern did not repeat itself more than two times in a row.
Following a 10-minute rest period, each participant performed a short-term retention test consisting of three trials, one of each pattern. The participants were invited back to the laboratory after 10 days for a long-term retention test, again performing three trials, one of each pattern. On both retention tests, the experimenter announced the order of the trials in a non-sequential order.
Each participant was assigned a number (indicated on the consent form), and data analysis was performed by viewing the video recordings of the instrument use. Nothing that would identify the participants was visible in the videos. The variable measured was the duration of time (to the nearest second) to complete each trial. The timer was manually started by the experimenter upon the participant grasping and lifting of the first rubber grommet and was stopped with the release of the third grommet onto its corresponding peg. The time taken to perform this task was the overall index of skill performance. Analyzed data was entered into a Microsoft ExcelTM (2021, Office 365 v16.0) spreadsheet containing participant numbers, practice schedule assigned, handedness, sex, and time taken to complete each trial.
Statistical data analysis included the calculation of the mean times for six clusters of nine acquisition trials (total of 54 trials), three short-term (10-minute) retention trials, and three long-term (10-day) retention trials across blocked and random practice groups (60 participants). Statistical analyses were performed using JamoviTM version 1.6 (2021). To examine the difference between groups during the acquisition trials, a two-way repeated measures analysis of variance (ANOVA) was performed on acquisition trials (6 acquisition clusters) x group (blocked vs. random), with repeated measures on the acquisition cluster. To examine the difference between groups in retention performance, a two- way repeated measures ANOVA was performed on retention (last cluster of acquisition vs. short-term retention vs. long- term retention) x group (blocked vs. random), with repeated measures on retention. An additional two-way repeated measures ANOVA was performed to compare acquisition and retention performance between sexes. To examine the difference between sexes during the acquisition trials, a two- way repeated measures analysis of variance (ANOVA) was performed on acquisition trials (6 acquisition clusters) x sex (male vs. female), with repeated measures on the acquisition cluster. To examine the difference between sexes in retention performance, a two-way repeated measures ANOVA was performed on retention (last cluster of acquisition vs. short- term retention vs. long-term retention) x sex (male vs. female), with repeated measures on retention. Tukey’s post- hoc tests were used to determine the location of within- and between-participant effects of significant main or interaction effects. Statistical significance was set at α = 0.05.
Results
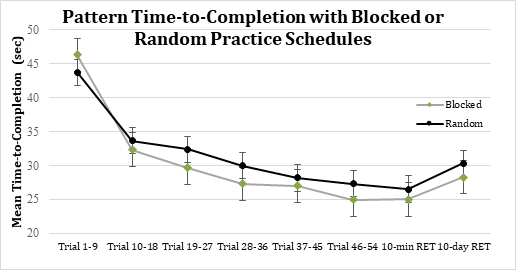
The index of performance was represented by the total time taken to complete each trial during acquisition and retention. Fifty-four acquisition trials were grouped into six blocks of nine trials, and retention tests were the average of all three trials for data analysis. Mean time-to-completion was plotted against trials to compare blocked and random practice groups in the acquisition, 10-minute, and 10-day retention tests (Figure 2).
Acquisition Differences between Blocked and Random Practice Schedules
The mean pattern-completion time in the blocked practice group was 31.24 ± 15.79 seconds, while the random practice schedule group completed acquisition patterns in a mean time of 32.14 ± 14.82 seconds.
There was a main effect of acquisition trials, F(5,290) = 119.43, p < .001. Post-hoc tests revealed that acquisition performance improved through practice, with all clusters significantly different from each other (p < .05) except for the fourth and fifth clusters, as well as the fifth and sixth clusters, which were not significantly different from each other (p > .05). There was no main effect of group, F(1,58) = 0.120, p = 0.731, and no significant interaction between acquisition clusters and group, F(5,290) = 1.89, p = 0.096.
The blocked practice group reduced its time-to- completion score from 46.3 to 24.9 seconds (46% improvement), while the random practice group averaged a 43.7 second time in the first cluster of trials and ended the acquisition trials with an average time-to-completion of 27.3 seconds (38% improvement).
Retention Differences between Blocked and Random Practice Schedules
There was a significant main effect of retention, F(2,116) = 9.342, p < .001. Post-hoc tests revealed that performance was not significantly reduced after a 10-minute break (p = 0.783). Long-term retention declined significantly compared to the last cluster of acquisition (p = 0.005) and short-term retention (p = 0.002). There was no significant main effect of group, F(1,58) = 0.862, p = 0.357, and no significant interaction between retention and group, F(2,116) = 0.480, p = 0.620. Hence, The rate of reduction in performance following a 10-day break was not significantly different between the groups.
Acquisition and Retention Sex Differences
There was a main effect of acquisition trials, F(5,290) = 121.83, p < .001. There was no main effect of sex, F(1,58) = 0.482, p = 0.490. There was a significant interaction between acquisition clusters and sex, F(5,290) = 3.09, p = 0.01.
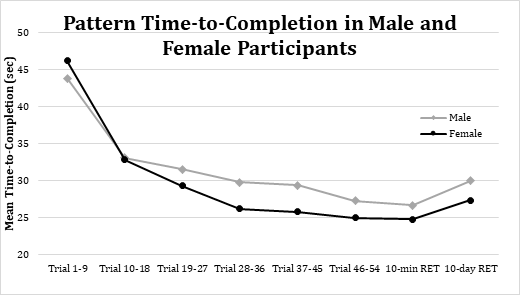
While female participants (time = 46.17 seconds) started with worse performance than males (time = 43.86 seconds) in the first cluster of acquisition trials, they improved faster than their male counterparts.
There was a 21.19 second (46%) versus 16.58 second (38%) improvement in pattern completion times, comparing the first (1-9) to last (46-54) clusters of acquisition trials, showcased by a steeper performance curve for the female participants (Figure 3). However, this difference in performance was not statistically significant, F(1,58) = 2.67, p = .108.
There were no statistically significant differences between the sexes in 10-minute retention, F(1,58) = 0.198, p = 0.658, and 10-day retention of performance, F(1,58) = 0.055, p = 0.815, when compared to the final cluster of acquisition trials (Figure 3). Hence, retention of the learned skill was similar between the sexes.
Discussion
The results obtained did not match our hypothesized effect of a random practice schedule resulting in impaired acquisition performance but improved short and long-term retention of simulated laparoscopic skills. The study did not find a difference between the acquisition and retention of simulated laparoscopic tasks across blocked and random practice schedules, in contrast to the findings by Shea J, et al. [2] who found impaired acquisition during learning of the skill with high levels of contextual interference (random practice schedule), but better short and long-term retention of the acquired performance, compared to low contextual interference condition (blocked practice schedule). While Shea J, et al. [2] experiment involved gross motor skills, Hynes-Dusel JM [11] and Shewokis PA, et al. [12] assessed fine motor skill acquisition and retention, with contradictory results. Hynes-Dusel JM [11] found enhanced retention following a blocked practice schedule, while Shewokis PA, et al. [12] detected improved performance and reduced cognitive load in retention tests following random acquisition trials.
Our findings are consistent with Rivard JA, et al. [13] study, which found that both practice schedules produced similar and significant improvements in both acquisition and retention of simulated laparoscopic tasks involving fine motor movements of the hands, fingers, and wrists. These results suggest that both blocked and random practice schedules can be deemed suitable choices for developing training programs in medical education settings aimed at improving laparoscopic surgery skills.
Interestingly, we found an effect of sex differences (Figure 3) on improvement in acquisition performance, where female learners improved more throughout the acquisition trials than male learners, however, this effect did not meet the established significance threshold (p of 0.108). Past literature discussing the acquisition and retention of either fine or gross motor skills did not report sex differences in the performance of such tasks (although Shea J, et al. [2] reported faster reaction times but longer movement times in female subjects, the total time to complete the task was not significantly different between the sexes). Although females improved to a greater extent over the 54 acquisition trials, their short and long-term retention was similar to that of males. Further experimental evidence is warranted to establish whether providing enhanced contextual interference to female laparoscopic trainees can better put them at the OCP of maximizing the potential learning benefit of simulated laparoscopic tasks and fine motor skill acquisition.
Guadagnoli MA, et al. [9] suggested that in order to reap the benefits of a random practice schedule, an OCP must be reached whereby the difficulty of the task is optimized to expose the learner to an ideal amount of interpretable information which is not too high or too low for their individual information-processing capabilities. Throughout the duration of the experiment, we observed great individual differences in the performance of the simulated laparoscopic tasks, whereby some individuals manipulated the laparoscopic tools and grommets with relative ease, while others experienced great difficulty, although all participants were naïve to simulated laparoscopic tasks. Therefore, it may be suggested that exposing all laparoscopic trainees to the same level of nominal task difficulty (objective difficulty of the activity) is counterintuitive since their individual functional task difficulty level (subjective difficulty of the task to the performer) towards the task may differ greatly. If the performers are exposed to a functional difficulty that is too low through blocked practice training, they may not reach their OCP to optimize learning. Similarly, if the performers are exposed to a subjective functional difficulty that is too high through a random practice schedule, they will experience information overload that exceeds their OCP, impairing learning and performance.
Therefore, laparoscopic skills training programs should be tailored to an individual’s initial skill level, as less-skilled performers will benefit from lower levels of contextual interference, and as they improve, additional contextual interference can be introduced to bring them to their optimal level of functional difficulty where they are exposed to an ideal amount of interpretable information that maximizes motor learning. Guadagnoli MA, et al. [9] predicted that the largest advantage of random practice for learning is for tasks of lower nominal difficulty, such as the tasks tested by Shea J, et al. [2] in which the participants used tennis balls to hit targets. Since fine motor skills involve a higher informational capacity than gross motor skills, random practice schedules may result in information overload and impair performers’ ability to process task requirements in the most beneficial way for learning and skill improvement [10].
Rivard JD, et al. [13] provided a possible explanation for their results based on Albaret JM, et al. [14] research concerning the effects of task complexity on contextual interference. Their study found that contextual interference’s benefits were only present in simple tasks, explaining that in complex tasks, participants have difficulty keeping all movement-related information in working memory as they progress through the different trials. Albaret JM, et al. [14] defines movement complexity as “the number of components (segments) of the patterns that the subjects have to reproduce” (p. 11). They found that simpler tasks were composed of two and three segments, while the complex task required the participants to learn four-segment movements. Rivard JD, et al. [13] used a laparoscopy simulator involving four tasks: peg transfer, pattern cutting, ligating loop, and intracorporeal suturing. Therefore, laparoscopic simulator training can be seen as a complex task, explaining the lack of performance benefit following high contextual interference learning conditions. However, our study only incorporated a peg transfer task, which poses the question of whether this task could be classified as a complex motor skill compared to other studies incorporating multiple tasks.
The target population of simulated laparoscopic skill training is medical students, residents, and surgical trainees, who often have previous exposure to complex fine motor skill training, whereas our study population consisted of individuals naïve to such targeted training. Thus providing high contextual interference in the form of a random practice schedule may have resulted in excessive movement complexity for the study population. Previous experience with fine motor skill training should be a consideration when designing training programs involving contextual interference to optimize the challenge point of the specific tasks for the target population.
Limitations
Several limitations should be considered when drawing conclusions from our study. Firstly, our participants were naïve to targeted fine motor skill training and were sampled from the general population. This differs from other laparoscopic training studies that typically assess medical trainees or practicing physicians [12, 13, 15, 16]. Therefore, our results may not be generalizable to those with prior experience in laparoscopic techniques or those in medical training programs. Further research is needed to understand how our findings apply to these populations.
Another limitation was our inability to recruit a sample size of 72 participants, as seen in Shea J, et al. [2]. We experienced issues with participants performing acquisition trials but not returning for retention tests after 10 days. This may be attributed to the lack of incentives offered to participants, as they did not receive any reward or benefit for their involvement in the study. Future research should consider the implementation of incentives to encourage participant motivation to participate and return for retest sessions.
Our study also employed a relatively short long-term retention interval of 10 days, compared to the 6-week interval utilized by Rivard JD, et al. [13]. It is possible that retention effects could differ over longer periods of time. Future research should explore the effects of varying retention intervals on the consolidation and retention of laparoscopic skills to better understand the long-term impacts of training.
Lastly, our sample consisted of participants within a wide range of ages, which may not be representative of medical students and residents. Although the majority of our participants were undergraduate students, the age variation could have influenced the results. Further studies should focus on samples that more accurately represent the target population of those undergoing laparoscopy surgical training to ensure greater external validity.
While our study provides valuable insights into simulated laparoscopic skills training, these limitations should be considered when interpreting the findings. Future research should address these limitations and explore the long-term effects of training on targeted fine motor skills within medical trainees and other relevant populations.
Future Directions
Moving forward, one important aspect to consider is the tailoring of contextual interference to match each learner’s skill level. Drawing from the existing literature, instructors should consider getting poor performers to begin with blocked practice, while more skilled performers could benefit from random practice [7, 8, 9]. By individualizing training regimens as much as possible, we can better accommodate the unique needs and abilities of each learner, leading to more efficient skill acquisition and improved overall performance.
Another crucial factor in optimizing learning, retention, and transfer of laparoscopic skills is identifying each learner’s OCP. By detecting this point, educators can tailor task difficulty during skill acquisition, ensuring that the learner remains engaged and motivated while also promoting the development of effective strategies for overcoming challenges. Future research should focus on developing methods for accurately identifying OCP’s and adapting training accordingly.
Additionally, educators must be able to distinguish between nominal and functional task difficulty when designing training programs. Nominal difficulty refers to the inherent complexity of a task, while functional difficulty accounts for the interaction between the learner’s skill level and the task’s complexity. Recognizing these differences allows educators to create training regimens that are more closely aligned with the needs of individual learners, promoting greater skill development, retention, and transfer to other tasks.
Our study demonstrated that the 3DmedTM laparoscopic training device can be used as a viable tool for improving simulated laparoscopic task skills, as performance significantly improved in both groups of participants during a short, approximately one-hour long study. Learners also retained their performance well in both 10-minute and 10- day retests and performed significantly better than at the beginning of the experiment. Future research should further explore the potential of this and other training devices, examining their effectiveness in various training contexts and their ability to support the long-term retention and transfer of laparoscopic skills.
The future of laparoscopic skills training research should focus on individualizing training experiences, identifying OCP’s, distinguishing between types of task difficulty, and exploring the efficacy of various training tools. There is also the difficulty in standardizing and measuring the acquired motor skills when working on a human patient to consider. By addressing these areas, we can continue to enhance the quality of laparoscopic training programs and ultimately improve surgical training efficiency and patient outcomes.
Conclusion
Our study did not support the hypothesized effect of a random practice schedule resulting in impaired acquisition performance but improved short and long-term retention of simulated laparoscopic skills.
Instead, we found that both blocked and random practice schedules produced similar improvements in acquisition and retention of these skills, aligning with the findings of Rivard JD, et al. [13]. Interestingly, we observed a trend towards greater improvement in acquisition performance for female learners, although this effect did not reach statistical significance. These results emphasize the importance of tailoring laparoscopic skills training programs to an individual’s initial skill level and considering their previous experience with fine motor skill training. By optimizing the challenge point of specific tasks for each learner, we can maximize their potential learning benefits in acquiring and retaining simulated laparoscopic task performance and fine motor skills. Further research is needed to explore the role of task complexity, individual differences, and the OCP in laparoscopic training programs, with the ultimate goal of improving surgical outcomes in clinical practice.
References
-
Aliseda D, Sapisochin G, Cruchaga PM, Zozaya G, Blanco N, et al. (2023) Association of laparoscopic surgery with improved perioperative and survival outcomes in patients with resectable intrahepatic cholangiocarcinoma: A systematic review and meta‑analysis from propensity‑score matched studies. Annals of Surgical Oncology 30(8): 4888-4901.
-
Shea J, Morgan RL (1979) Contextual interference effects on the acquisition, retention and transfer of a motor skill. Journal of Experimental Psychology: Human Learning and Memory 5(2): 179-187.
-
Alkatout I, Mechler U, Mettler L, Pape J, Maass N, et al. (2021) The development of laparoscopy: A historical overview. Frontiers of Surgery 8(799442): 1-12.
-
Lagares-Garcia J, Bansidhar B, Moore RA (2003) Benefits of laparoscopy in middle-aged patients. Surgical Endoscopy 17(1): 68-72.
-
Chiu CC, Hsu WT, Choi JJ, Galm B, Lee MG, et al. (2019) Comparison of outcome and cost between the open, laparoscopic, and robotic surgical treatments for colon cancer: A propensity score-matched analysis using nationwide hospital record database. Surgical Endoscopy 33(11): 3757-3765.
-
Laudicella M, Walsh B, Munasinghe A, Faiz O (2016) Impact of laparoscopic versus open surgery on hospital costs for colon cancer: A population-based retrospective cohort study. BMJ Open 6(11): e012977.
-
Lee TD, Wishart LR (2005) Motor learning conundrums (and possible solutions). Quest 57(1): 67-78.
-
Magill RA, Hall KG (1990) A review of the contextual interference effect in motor skill acquisition. Human Movement Science 9(3-5): 241-289.
-
Guadagnoli MA, Lee TD (2004) Challenge point: A framework for conceptualizing the effects of various practice conditions in motor learning. Journal of Motor Behavior 36(2): 212-224.
-
Fitts PM (1954) The information capacity of the human motor system in controlling the amplitude of movement. Journal of Experimental Psychology 47(6): 381-391.
-
Hynes-Dusel JM (2002) Practice and motor learning. The Physical Educator 59(2): 58-66.
-
Shewokis PA, Shariff FU, Liu Y, Ayaz H, Castellanos A, et al. (2016) Acquisition, retention and transfer of simulated laparoscopic tasks using fNIR and a contextual interference paradigm. The American Journal of Surgery 213(2): 336-345.
-
Rivard JD, Vergis AS, Unger BJ, Gillman LM, Hardy KM, et al. (2015) The effect of blocked versus random task practice schedules on the acquisition and retention of surgical skills. The American Journal of Surgery 209(1): 93-100.
-
Albaret JM, Thon B (1998) Differential effects of task complexity on contextual interference in a drawing task. Acta Psychologica 100(1-2): 9-24.
-
Hasson HM, Kumari NV, Eekhout J (2001) Training simulator for developing laparoscopic skills. Journal of the Society of Laparoendoscopic Surgeons 5(3): 255- 265.
-
Johnson GGRJ, Park J, Vergis A, Gillman LM, Rivard JD (2022) Contextual interference for skills development and transfer in laparoscopic surgery: A randomized controlled trial. Surgical Endoscopy 36(9): 6377-6386.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review