Prognostic Significance of the Lymph Node Ratio for Overall Survival after Curative Surgery for Rectal Cancer: A Retrospective Cohort Study
Background: Accurate rectal cancer N staging requires the histopathological evaluation of at least 12 lymph nodes. Retrieval of that count is not always possible. The purpose of the study is to evaluate the lymph node ratio (LNR) prognostic significance on overall survival. Methods: The current study is a retrospective cohort study of 229 patients who underwent curative surgery for resectable rectal cancer. Receiver Operating Characteristic (ROC) curve analysis was used to determine the optimal cut-off value for Lymph Node Count (LNC), Positive Lymph Nodes count (PLN), and LNR for overall survival (OS). The Kaplan-Meier product limit method was used for univariate analysis of factors affecting OS. Log Rank (Mantel-Cox) test was used to test significance. A Cox-Regression Hazard model was used to detect the most significant factor affecting OS. Results: ROC curve analysis of the PLNs revealed a poor prognostic value of the test, with a sensitivity of 51.9% at PLNs 4 cutoff value, with a shorter mean OS above it (21.71±11.597 vs. 31.20 ± 16.634 for ≥4 vs. <4). ROC curve analysis of LNC revealed the poor value of the test, with a sensitivity of 56% at LNC 12 cutoff value, with longer mean Overall Survival (OS) above it (28.21±15.432 vs. 22.22±12.97 for LNC ≥12 vs. <12). ROC curve analysis of the LNR revealed good value of the test for predicting survival, with a sensitivity of 95% at LNR 18.82% cutoff value, with longer mean OS above it (21.44±11.607 vs. 39.82±15.085 for LNR ≥18.8% vs. <18.8%). According to our univariate analysis, the factors significantly affecting OS were histopathological examination (p =.000), Lympho-Vascular Invasion (LVI) (p =.014), and the LNC cutoff value (p=.002), the PLN cutoff value (p =.008), and the LNR cutoff value (p =.000. According to our multivariate analysis, the LNR cutoff value of 18.8% was the most significant factor affecting OS (p =.000). Conclusions: A high LNR with an 18.82% cutoff value is an independent adverse prognostic factor affecting OS after curative surgery for cancer rectum. The LNR could be considered a good alternative to the absolute number of PLNs, particularly in patients with a low LNC. A higher LNC ≥12 was associated with a longer OS; maximum possible lymphadenectomy should be performed for each patient.
Abbreviations
CRC: Colorectal Cancer; ERUS: Endorectal Ultrasound; LVI: Lymphovascular Invasion; LNC: Lymph Nodes Removed; PLNs: Positive Lymph Nodes; CAP: College of American Pathologists; AJCC: American Joint Committee on Cancer; ROC: Receiver Operating Characteristic.
Introduction
Colorectal cancer (CRC) is the 3rd most common cancer and the 2nd most common cause of cancer death worldwide [1]. In Egypt, colorectal cancer is the 7th most common cancer, accounting for 3.47% and 3% of all male and female cancers, respectively [2]. Lymph node metastasis is considered the most significant prognostic factor affecting the five-year survival rate, where it decreases from 80% to 30%-60% [3].
Accurate staging of colorectal cancer is critical for adjuvant therapies planning. The College of American Pathologists (CAP) and the American Joint Committee on Cancer (AJCC) staging system recommended the removal of a minimum of 10–14 lymph nodes to decrease the incidence of pathological downstaging; however, this is not always possible [4, 5, 6, 7].
LNC harvested en bloc with the surgical specimen affects staging accuracy and oncological outcomes. It is affected by many factors, including surgeon experience and specialization, extent of surgical resection, patient volume, emergency status, use of laparoscopy, advanced age, female sex, obesity, preoperative radiotherapy, tumor site, and tumor stage [8].
The 8th edition of the AJCC staging system for colorectal tumors is based on the number of metastatic lymph nodes, and the retrieval of 12 or more lymph nodes is required for accurate staging. A lower LN count is associated with false- negative N staging followed by under treatment.
The 8th edition of the AJCC staging system Recommends new imaging studies such as MRI and Endorectal Ultrasound (ERUS) to improve N staging accuracy [7].
According to Destri GL, et al. [8] the LNR is an independent prognostic factor in patients with colorectal cancer when compared to the PLN count, mainly in patients with an inadequate number of retrieved lymph nodes [8].
This study was conducted to compare the significance of the LNR and the absolute PLN count on OS in patients with resectable rectal cancer who underwent surgical resection with curative intent.
Patients and Methods
A retrospective cohort study included 229 patients with rectal cancer, 69 of them received neoadjuvant therapy.
Patients who underwent radical resection with curative intent between 2012 and 2022 in 2 tertiary hospitals were included. This work is in line with the STROCSS criteria [9].
The exclusion criteria included patients with familial adenomatous polyposis, multiple synchronous or metachronous rectal cancers, and death within 3 months.
All patients were subjected to medical history, physical examination, preoperative full laboratory investigations, metastatic workup, CEA, CA 19-9, and colonoscopic biopsy for tissue diagnosis. Cancer stages were scored according to the American Joint Committee on Cancer (AJCC) Staging System, 8th edition.
Demographic, histopathological, follow-up and outcome data were collected retrospectively from completed hospital files for patients operated on since 2012. The demographic information included age, sex, family history, and chief complaint at presentation. Histopathological data included tumor site, grade, Lymphovascular invasion (LVI), total number of lymph nodes removed (LNC), and number of positive lymph nodes (PLNs).
The LNR was defined as the ratio of PLN to LNC in the histopathology specimen. OS was defined as the duration between the date of surgical resection and the date of death in months.
Surgical method of lymph node dissection: Total mesorectal excision with high or middle level ligation of the inferior mesenteric artery was used. Lateral lymph node dissection was performed selectively in patients with suspicious enlarged lymph nodes.
Handling method for the specimen: The surgeon did not open the bowel segment. The specimen was oriented with sutures and then sent to the pathologist. The pathologist fixed the specimens in 10% formalin for at least 96 hours. Sampling from the tumor and radial, proximal and distal margins was performed. All LNs were identified by palpation and removed sharply by scissors and scalpel. Every single lymph node was bisected or trisected and submitted to paraffin sectioning, followed by microscopic examination. Immunohistochemistry and genetic testing were only performed for selected patients.
Follow-up: All patients were followed up postoperatively every 3 months for the first 2 years, every 6 months for 3
years, and then whenever necessary. The follow-up period included clinical assessments for possible complications, tumor markers, and investigations (endoscopic/radiological) as needed.
Statistical Analysis
Demographic, histopathological, and postoperative follow-up data were collected, tabulated, and analysed by SPSS version 26 (Statistical Package for Social Sciences, PSS, Inc., Chicago, Illinois, USA). Qualitative data are presented as frequencies and percentages. Numerical data are expressed as the arithmetic mean ± standard deviation (M±SD). The Kolmogorov‒Smirnov test was used to test the normality of the data distribution.
Receiver Operating Characteristic (ROC) curve analysis was used to determine the optimal cut-off value affecting OS for LNC, PLN, and the LNR. The Kaplan‒Meier product limit method was used in univariate analysis for factors affecting OS. The log rank (Mantel–Cox) test was used for significance. All the significant factors identified in the univariate analysis were entered into the Cox regression hazard model test, and the Wald test was used to determine the most significant factors affecting OS. A p value < 0.05 was considered to indicate statistical significance.
Results
This study included 229 patients with operable rectal cancer who underwent radical surgery with curative intent. Of the 229 patients, 121 (52.8%) were males. The age range and M±SD were 18-85 (48.02±15.98) years. The most common site of the tumor was the lower rectum in 88 (38.4%) patients. Low anterior resection was the most common procedure performed on 127 (55.5%) patients. Open surgery was performed for 219 patients, and laparoscopic- assisted surgery was performed for 10 patients. A diverting stoma was used for 46 patients (20.1%). Complications were encountered in 60 patients. The most frequent complication was wound infection (24 patients), followed by low-output fistulas (18 patients). The patients’ follow-up period ranged between 1 and 7 years.
Moderately differentiated adenocarcinoma was the most common histopathology present in 96 (41.9%) patients. Lympho-Vascular Invasion (LVI) was present in 90 (39.3%) patients. Stage 3 rectal cancer was the most common stage in our cohort 135 (59%) patients. LNC was more than 12 in 148 (64.6%) patients. The LNC range and M±SD were 2-37 (13.22±6.464). The PLN range and M±SD were 0-11(3.94±2.658). In 39 (17%) patients, recurrence was recorded at 4-42(13.67±9.742) months. The mortality rate was 35.4% (81 patients). The mean overall survival was 5-75 (25.93±14.806) months. Demographic and pathological data of the studied group are summarized in Table 1.
| Variable | Results | |
|---|---|---|
| Age | Range | 18-85 |
| Mean±SD | 48.02±15.978 | |
| Sex (Number and percentage) | Female | 108 (47.2%) |
| Male | 121 (52.8%) | |
| Neoadjuvant Therapy (Number and percentage) | No | 160 (69.9%) |
| Chemotherapy | 4 (1.7%) | |
| Radiotherapy | 4 (1.7%) | |
| Chemoradiation | 61 (26.6%) | |
| Lymphovascular Invasion (Number and percentage) | No | 139 (60.7%) |
| Yes | 90 (39.3%) | |
| T Stage (Number and percentage) | T1 | 2 (9%) |
| T2 | 40 (17.5%) | |
| T3 | 165 (72.1%) | |
| T4 | 22 (9.6%) | |
| N Stage (Number and percentage) | N0 | 94 (41%) |
| N1 | 67 (29.3%) | |
| N2 | 68 (29.7%) | |
| Tumor Stage (Number and percentage) | Stage 1 | 10 (4.4%) |
| Stage 2 | 84 (36.7%) | |
| Stage 3 | 135 (59%) | |
| Positive Lymph Node Count | Range | 0-11 |
| Mean±SD | 3.94±2.658 | |
| Lymph Node Count | Range | 2-37 |
| Mean±SD | 13.22±6.464 | |
| Distal Resection Margin in Cms | Range | 0.5-8 |
| Mean±SD | 2.616± 1.5562 | |
| Recurrence (Number and percentage) | No | 190 (83%) |
| Yes Locoregional recurrences/ Distant Recurrence | 26 (11.3%3) | |
| Disease Free Survival in months | Range | 4-42 |
| Mean±SD | 13.67± 9.742 | |
| Survival in Months | Range | 5-75 |
| Mean±SD | 25.93± 14.806 |
Table 1: Demographic and pathological data of the studied group.
ROC Curve Analysis
ROC curve analysis of PLNs revealed the poor value of the test (area under the curve: 0.643; with a sensitivity 51.9%, specificity 35.1%; at PLNs 4 cut-off value with shorter mean OS above it (21.71±11.597 vs. 31.20 ± 16.634 for PLNs ≥ 4 vs. PLNs < 4).
ROC curve analysis of LNC revealed poor predictive value (area under the curve=0.62; sensitivity=56%;
specificity=33%; LNC12 cut-off value, with longer mean OS above this cut-off (28.21±15.432 vs. 22.22±12.97 for LNC ≥ 12 vs. LNC < 12).
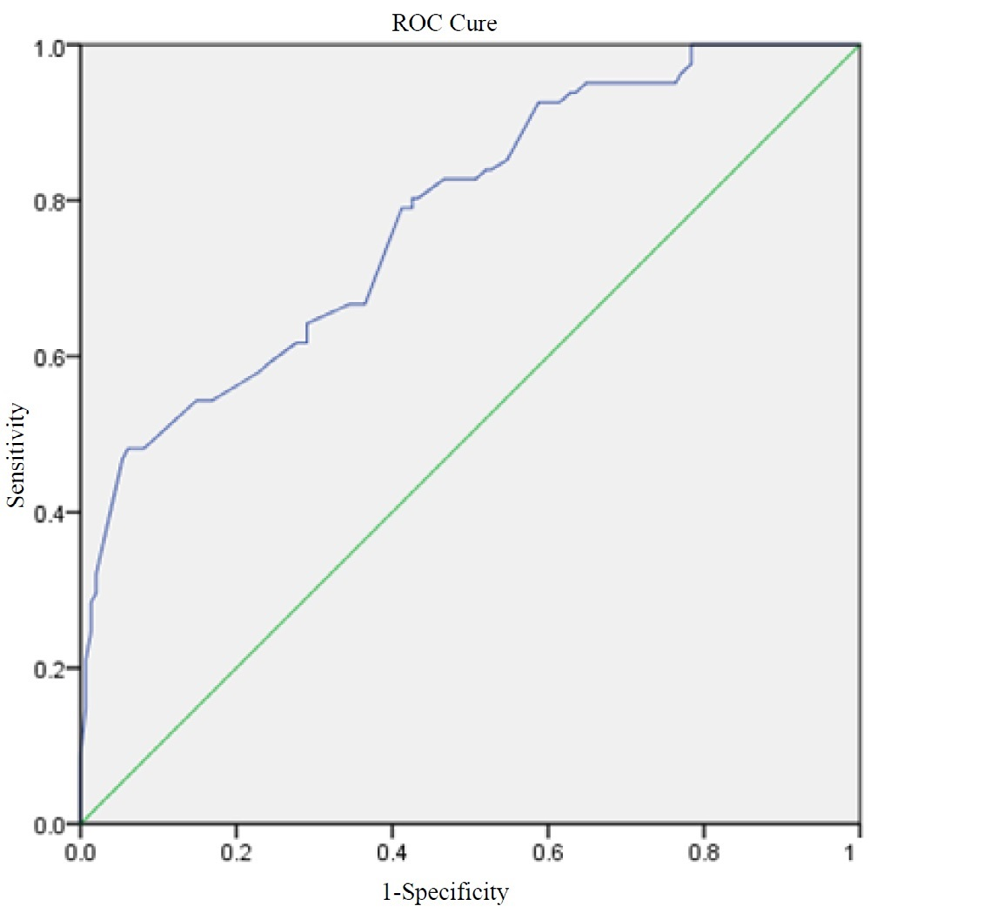
ROC curve analysis of the LNR revealed a good value of the test for predicting OS (area under the curve=0.78; with a sensitivity 95% and specificity 65% at LNR 18.82% cut-off value), with longer mean OS below this cut-off (21.44±11.607 vs. 39.82±15.085 for LNR ≥18.8% vs. LNR<18.8%) (Figure 1).
Univariate Analysis
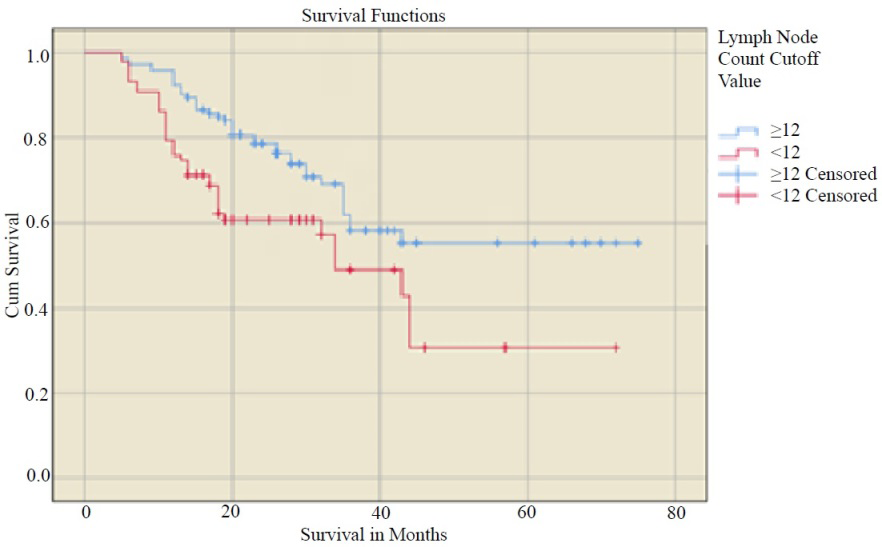
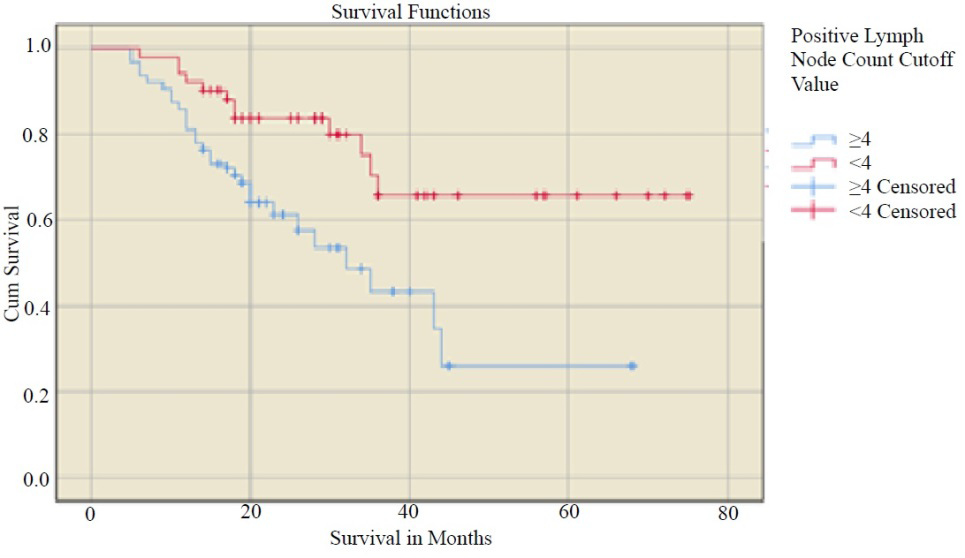
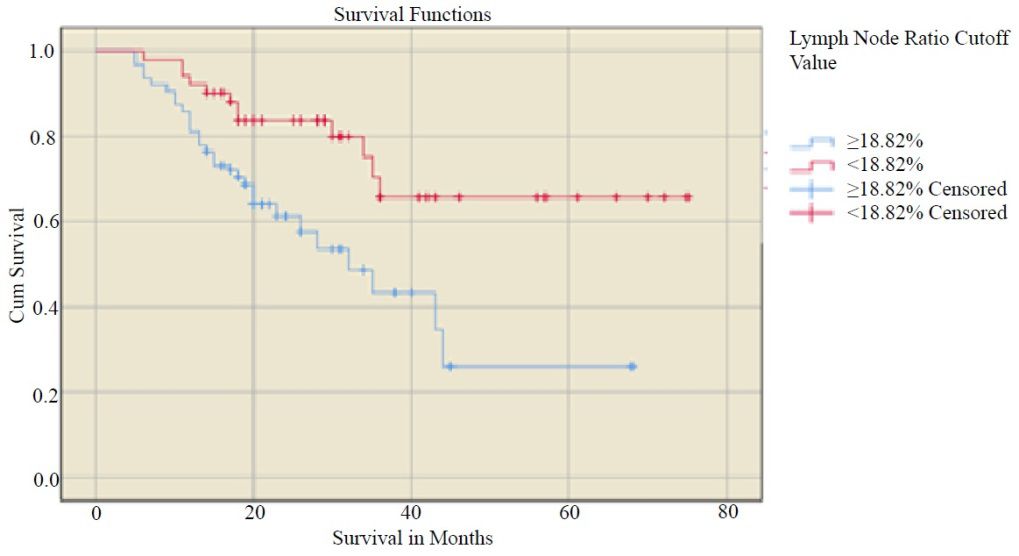
The factors significantly affecting OS were histopathological examination (p =.000), LVI (p =.014), the LNR cut-off value (p =.000), and the LNC cut-off value (p =.002.). Histopathology, LVI, an LNR cut-off value of 18.82%, and PLN cut-off value ≥ 4 had significant negative effect on OS, while LNC had a significant positive effect on OS (Tables 2,3 & Figures 2-4).
| Variable | Number of Patents (n= 229) | Percentage | p value | |
|---|---|---|---|---|
| Gender | Female | 108 | 47.20% | 0.675 |
| Male | 121 | 52.80% | ||
| Site of the tumor | Upper Rectum | 85 | 37.10% | 0.675 |
| Mid Rectum | 56 | 24.50% | ||
| Low Rectum | 88 | 38.40% | ||
| Histopathological Examination | Well differentiated adenocarcinoma | 64 | 27.90% | .000 |
| Moderately differentiated adenocarcinoma | 96 | 41.90% | ||
| Poorly differentiated adenocarcinoma | 6 | 2.60% | ||
| Undifferentiated adenocarcinoma | 2 | 0.90% | ||
| Mucinous Carcinoma | 54 | 23.60% | ||
| Signet Ring Carcinoma | 7 | 3.10% | ||
| LVI | No | 139 | 60.70% | 0.014 |
| Yes | 90 | 39.30% | ||
| N Stage | N0 | 94 | 41.00% | 0.063 |
| N1 | 67 | 29.30% | ||
| N2 | 68 | 29.70% | ||
| PLNC Cut-off Value | ≥ 4 | 127 | 55.50% | 0.008 |
| < 4 | 102 | 44.50% | ||
| LNR Cut-off Value | <18.8% | 56 | 24.50% | .000 |
| ≥ 18.8% | 173 | 75.50% |
Table 2: Univariate analysis of factors affecting overall survival.
| Variable | Mean±SD | p value | ||
|---|---|---|---|---|
| Age in years (Mean±SD) | 48.02±15.978 | 0.053 | ||
| Absolute LNC (Mean±SD) | 13.22±6.464 | 0.224 | ||
| Survival In months (Mean±SD) | Overall Survival in Months | 25.93±14.806 (5-75) | - | |
| LNC cut-off value | ≥ 12 | 28.21±15.432 | 0.002 | |
| <12 | 22.22± 12.970 | |||
| PLNC cut-off value | ≥ 4 | 21.71±11.597 | 0.008 | |
| < 4 | 31.20± 16.634 | |||
| LNR cut-off value | Overall | 32.067±20.34 | .000 | |
| <18.8% | 21.44±11.597 | |||
| ≥ 18.8% | 39.82± 16.634 | |||
| LVI | Present | 24.80±13.337 | 0.014 | |
| Absent | 26.67± 15.687 | |||
| Distal Resection Margin in cms | 2.616±1.5562 | 0.714 |
Table 3: Univariate analysis of factors affecting overall survival.
The hazard of death increased by 263.1% with each unit increase in the LNR above the cut-off value. A total of ≥ 12 LNCs had a statistically significant positive effect on OS. The hazard of death decreased by 63.3% with each unit increase above the LNC cut-off value (Table 4).
| Variable | B | SE | Wald | df | Sig. | Exp(B) |
|---|---|---|---|---|---|---|
| Histopathological Examination | -.620 | .642 | 0.932 | 1 | .334 | .538 |
| Lympho-Vascular Invasion | .440 | 0.242 | 3.307 | 1 | .069 | 1.552 |
| LNC cut-off value | -.633 | 0.23 | 7.73 | 1 | .005 | .531 |
| PLNC Cut-off | .391 | 0.28 | 1.946 | 1 | .163 | 1.479 |
| LNR cut-off value | 2.631 | 0.52 | 25.6 | 1 | .000 | 13.889 |
Table 4: Multivariate analysis of factors affecting overall survival.
In addition, according to the multivariate analysis of factors affecting tumor recurrence and disease-free survival, the LNR affects recurrence but not disease-free survival (Tables 5 & 6).
| Covariates | Univariate analysis | Multivariate analysis | |||||||
|---|---|---|---|---|---|---|---|---|---|
| p value | B | SE | Wald | df | p value | Exp(B) | 95.0% CI for Exp(B) | ||
| Lower | Upper | ||||||||
| Age | 0 | -0.1 | 0.02 | 20.45 | 1 | 0 | 0.908 | 0.87 | 0.947 |
| Sex | 0.036 | -1.69 | 0.52 | 10.64 | 1 | 0.001 | 0.185 | 0.067 | 0.51 |
| Lymphovascular Invasion | 0.014 | 0.579 | 0.52 | 1.258 | 1 | 0.262 | 1.784 | 0.649 | 4.907 |
| Tumer Stage | 0.003 | -0.93 | 0.49 | 3.649 | 1 | 0.056 | 0.393 | 0.151 | 1.025 |
| Distal Resection Margin in Cms | 0.03 | -0.08 | 0.16 | 0.239 | 1 | 0.625 | 0.923 | 0.671 | 1.271 |
| Neoadjuvant Therapy | 0 | -0.56 | 0.6 | 0.857 | 1 | 0.355 | 0.573 | 0.177 | 1.861 |
| Adjuvant Therapy | 0.008 | 0.595 | 0.47 | 1.63 | 1 | 0.202 | 1.813 | 0.727 | 4.517 |
| Lymph Node Ratio | 0 | 0.048 | 0.01 | 11.89 | 1 | 0.001 | 1.049 | 1.021 | 1.078 |
| Positive Lymph Node Count | 0.009 | 0.029 | 0.11 | 0.073 | 1 | 0.787 | 1.03 | 0.833 | 1.272 |
Table 5: Factors predicting tumor recurrence after curative surgery for cancer rectum.
| Covariates | Univariate analysis | Multivariate analysis | |||||||
|---|---|---|---|---|---|---|---|---|---|
| p value | B | SE | Wald | df | p value | Exp(B) | 95.0% CI for Exp(B) | ||
| Lower | Upper | ||||||||
| Age | .000 | .049 | .025 | 3.726 | 1 | .054 | 1.050 | .999 | 1.104 |
| Histopathological Examination | .000 | .094 | .179 | .278 | 1 | .598 | 1.099 | .774 | 1.562 |
| Distal Resection Margin in Cms | .013 | .214 | .168 | 1.628 | 1 | .202 | 1.238 | 0.892 | 1.720 |
| Positive Lymph Node Count | .006 | .241 | .113 | 4.513 | 1 | .034 | 1.272 | 1.019 | 1.589 |
| Lymph Node Ratio | 0.004 | -.009 | .013 | .431 | 1 | .511 | .991 | .966 | 1.018 |
| Neoadjuvant Therapy | .003 | -.187 | .538 | .120 | 1 | .729 | .83 | .289 | 2.383 |
| Adjuvant Therapy | .004 | -1.525 | .675 | 5.107 | 1 | .024 | .218 | .058 | .817 |
Table 6: Factors Predicting Disease-free Survival After curative surgery for cancer rectum.
Discussion
The main route of spread of colorectal cancer is through lymphatic spread. In rectal cancer, the lymph node burden, and the absolute number of PLNs have been established as adverse predictors of OS [10]. Therefore, according to the current (AJCC) staging system, the PLN count was categorized as the N category based on the absolute number of metastatic lymph nodes, in which N1 had 1-3 PLNs and N2 had >4 PLNs [11]. This staging system does not consider the number of negative lymph nodes that are independently correlated with improved OS [12].
In 1990, the World Congress of Gastroenterology in Sydney established a minimum of 12 LNs to achieve the correct diagnosis of N0 in 90% of patients [13]. This number was referred to as the magic number by Kukreja SS, et al. [14]. Additionally, Fielding, et al. reported that the histopathological evaluation of LNC less than 12 is associated with a high false-negative rate and understaging, which is considered a limitation in the American Joint Committee on Cancer (AJCC) staging system [14]. The LNR can be used to overcome this limitation, particularly in patients with a low LNC.
This magic number cannot be reached in all cases because it is affected by many modifiable and unmodifiable factors. Destri GL, et al. [8] reported in their systematic review that a surgeon with more than 15 years of experience (p < 0.05), colorectal subspecialisation of the surgeon (p = 0.001), surgeon’s annual case volume of 5 or more patients (p = 0.001) and laparoscopic lymphadenectomy for rectal cancer (p = 0.026) were associated with an increased number of LNCs. Advanced age and more difficult surgical resections due to low rectal tumors, neoadjuvant radiotherapy, and obesity were associated with a lower LNC [8, 15].
In our study, the cut-off value for the LNC was 12. Patients with a retrieved LNC ≥ 12 had a longer OS. In a systematic review carried out by Chang et al. on 16 of 17 studies, increased OS was reported in patients with higher LNC [16]. Additionally, Norwood et al. reported a decreased OS in patients with LNC less than 12 [17].
In a systematic analysis of 10 studies carried out on 4300 patients by McDonald et al., the LNC cut-off value was between 6 and 21 [13]. It was 6-17 in the Valsecchi ME, et al. [18] study and 6-40 in the Noura S, et al. [19] study. These results might draw attention to the so-called magic number, which seems to be real.
Retrieval of ≥ 12 lymph nodes seems to not only have a positive impact on OS but also to have therapeutic value regardless of the number of positive nodes in the specimen. This difference might be attributed to the clearance of microdeposits in the mesentery and lymphatic vessels along with en bloc excision in the presence of negative lymph nodes. The obsession with this number was discussed in detail by Kukreja SS, et al. [14] in their article.
If the LNR provides an alternative predictor of the N stage, surgeon effort and enthusiasm should not decrease to perform maximum lymphadenectomy as much as the situation permits. This approach avoids compromising accurate N staging and subsequent treatments and, moreover, provides the patient with the best possible chance for maximum possible LNC retrieval and OS.
In our study, a higher LNR was associated with poor OS. Comparable results were reported in a meta-analysis of 33 studies performed on 75,839 patients by Zhang et al. These authors reported that a high LNR was significantly associated with shorter OS (hazard ratio (HR): 1.91; 95% CI: 1.71-2.14; p<.001) regardless of LNC [20].
In summary, LNC ≤12, PLC ≥ 4, and LNR ≥ 18.82% had negative effects on OS according to univariate analysis.
The LNR was the most significant factor according to multivariate analysis, with a cut-off value of 18.82%, a sensitivity of 95%, and a specificity of 65%. The LNR not only reflects the lymph node status but also prevents understaging and subsequent undertreatment, particularly in patients with a low LNC.
Conclusion
A high LNR with an 18.82% cutoff value is an independent adverse prognostic factor affecting OS after curative surgery for cancer rectum. The LNR could be considered a good alternative to the absolute number of PLNs, particularly in patients with a low LNC. A higher LNC ≥12 was associated with a longer OS; maximum possible lymphadenectomy should be performed for each patient.
Statements & Declarations
Ethical Approval and Study Registration
Ethical approval for this study was provided by the Ethical Committee of Faculty of Medicine, South Valley University, Qena, Egypt , in October 2022 IRB number SVU- MED-SUR011-4-22-10-464. The study has been registered at ClinicalTrials.gov with a Unique Identifying number or registration ID: NCT05667259 which found at: ClinicalTrials. gov PRS: Record Summary NCT05667259.
Funding
No source of funding
Availability of Data And Materials
The dataset is available upon reasonable request.
Competing Interests
The authors have no relevant financial or non-financial interests to disclose.
Authors Contributions
All authors participated in the study concept and study design, reviewing patients’ files and collection of data. Abdallah Taha performed the statistical analysis and wrote the primary draft of the manuscript. All authors reviewed the manuscript. Taha, refined, edited the manuscript to its final form, and he is the corresponding author.
References
-
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, et al. (2018) Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 68(6): 394- 424.
-
Ibrahim AS, Khaled HM, Mikhail NN, Baraka H, Kamel H (2014) Cancer incidence in Egypt: results of the national population-based cancer registry program. J Cancer Epidemiol 2014: 437971.
-
Siegel R, Ward E, Brawley O, Jemal A (2011) Cancer statistics, 2011: the impact of eliminating socioeconomic and racial disparities on premature cancer deaths. CA Cancer J Clin 61(4): 212-36.
-
Le Voyer TE, Sigurdson ER, Hanlon AL, Mayer RJ, Macdonald JS, et al. (2003) Colon cancer survival is associated with increasing number of lymph nodes analyzed: a secondary survey of intergroup trial INT- 0089. J Clin Oncol 21(15): 2912-2919.
-
Tepper JE, O Connell MJ, Niedzwiecki D, Hollis D, Compton C, et al. (2001) Impact of number of nodes retrieved on outcome in patients with rectal cancer. J Clin Oncol 19(1): 157-163.
-
Washington MK, Berlin J, Branton P, Burgart LJ, Carter DK, et al. (2009) Protocol for the examination of specimens from patients with primary carcinoma of the colon and rectum. Arch Pathol Lab Med 133(10): 1539-1551.
-
Amin MB, Greene FL, Edge SB, Compton CC, Gershenwald JE, et al. (2017) The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population- based to a more “personalized” approach to cancer staging. CA Cancer J Clin 67(2): 93-99.
-
Li Destri G, Di Carlo I, Scilletta R, Scilletta B, Puleo S (2014) Colorectal cancer, and lymph nodes: the obsession with the number 12. World J Gastroenterol 20(8): 1951-1960.
-
Mathew G, Agha R, Albrecht J, Goel P, Mukherjee I, et al. (2021) STROCSS 2021: Strengthening the Reporting of cohort, cross-sectional and case-control studies in Surgery. International Journal of Surgery 96: 106165.
-
Vather R, Sammour T, Kahokehr A, Connolly A, Hill A (2011) Quantitative lymph node evaluation as an independent marker of long-term prognosis in stage III rectal cancer. ANZ J Surg 81(12): 883-888.
-
Amin MB, Greene FL, Edge SB, Compton CC, Gershenwald JE, et al. (2017) The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population- based to a more “personalized” approach to cancer staging. CA Cancer J Clin 67(2): 93-99.
-
He WZ, Xie QK, Hu WM, Kong PF, Yang L, et al. (2018) An increased number of negative lymph nodes is associated with a higher immune response and longer survival in colon cancer patients. Cancer Manag Res 10: 1597-1604.
-
McDonald JR, Renehan AG, O’Dwyer ST, Haboubi NY (2012) Lymph node harvest in colon and rectal cancer: Current considerations. World J Gastrointest Surg 4(1): 9-19.
-
Kukreja SS, Esteban-Agusti E, Velasco JM, Hieken TJ (2009) Increased lymph node evaluation with colorectal cancer resection: does it improve detection of stage III disease. Arch Surg 144(7): 612-617.
-
Fielding LP, Arsenault PA, Chapuis PH, Dent O, Gathright B, et al. (1991) Clinicopathological staging for colorectal cancer: an International Documentation System (IDS) and an International Comprehensive Anatomical Terminology (ICAT). J Gastroenterol Hepatol 6(4): 325- 344.
-
Chang GJ, Rodriguez-Bigas MA, Skibber JM, Moyer VA (2007) Lymph node evaluation and survival after curative resection of colon cancer: systematic review. J Natl Cancer Inst 99(6): 433-441.
-
Norwood MG, Sutton AJ, West K, Sharpe DP, Hemingway D, et al. (2010) Lymph node retrieval in colorectal cancer resection specimens: national standards are achievable, and low numbers are associated with reduced survival. Colorectal Dis 12(4): 304-309.
-
Valsecchi ME, Leighton J, Tester W (2010) Modifiable factors that influence colon cancer lymph node sampling and examination. Clin Colorectal Cancer 9(3): 162-167.
-
Noura S, Ohue M, Kano S, Shingai T, Yamada T, et al. (2010) Impact of metastatic lymph node ratio in node- positive colorectal cancer. World J Gastrointest Surg 2(3): 70-77.
-
Zhang MR, Xie TH, Chi JL, Li Y, Yang L, et al. (2016) Prognostic role of the lymph node ratio in node positive colorectal cancer: a meta-analysis. Oncotarget 7(45): 72898-72907.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review