35-year Follow-Up Case Report of a Rheumatic Heart Disease Patient with all Valve Replacement
Rheumatic heart disease (RHD) is a preventable cardiovascular disease highly prevalent in developing and underdeveloped countries, especially among women and children. According to the World Heart Federation (WHF), RHD claims 2% of cardiovascular deaths globally. It is caused by rheumatic fever, an inflammation caused by group A streptococcus bacteria leading to valvular dysfunctions eventually leading to death or life-long disability. Surgical valve replacements are being administered to treat valvular disorders in RHD patients. A 22-year-old South Asian female was presented with dyspnoea on exertion. Echocardiography confirms severe rheumatic heart disease with Aortic stenosis (AS), Mitral stenosis (MS), and Tricuspid stenosis (TS). Due to the recurrence of this problem along with other associated complications, the patient had triple valve replacement surgeries at different time points since 1988. These surgeries were uneventful and many secondary complications were regressed post-procedure. This article documents a cardiac auto transplant performed for a triple valve replacement with a 35-year follow-up suggesting that auto transplantation with triple valve replacement improved the condition of the patient.
Abbreviations
RHD: Rheumatic Heart Disease; AS: Aortic Stenosis, MS: Mitral Stenosis; TS: Tricuspid Stenosis; WHF: World Heart Federation.
Introduction
Rheumatic heart disease (RHD) is caused by an autoimmune response triggered by recurring infection by Group A streptococcus bacteria. The reoccurrence results in inflamed valves and heart muscles weakening which eventually leads to chronic valvular disorders and heart failure. Due to poor diagnosis and inadequate primary care accessibility in low-income to middle-income countries, children and women below the age of 25 years old are more susceptible to RHD. According to the World Heart Federation (WHF), RHD claims 2% of cardiovascular deaths globally [1, 2].
It is an acquired cardiovascular disease that can be prevented with early detection and accessibility to primary care. Currently, echocardiography is the preliminary method of diagnosis for RHD globally and other techniques may include cardiovascular magnetic resonance which also provides detailed information on the underlying traits of RHD [3]. In 2023, the World Heart Foundation (WHF) has published a two-step echocardiography diagnosis for RHD. This outlines guidelines and risk management for early detection of RHD-endemic regions [4].
Depending on the complexity of patients suffering from rheumatic heart disease, they are administered through either antibiotic therapy in early stages or valve repairs and replacement in severe conditions [5, 6, 7]. The mitral and atrial valves are the most common valves affected in patients with RHD. RHD affecting the tricuspid and pulmonary valve are less common [8]. Since the disease affects the younger population in lower economic countries, addressing valvular complications of RHD through surgical management is on the rise. A better understanding of intervention timing has been reported to increase the survival rate of RHD patients [9].
In this case report, we present a 35-year follow-up report of a patient diagnosed with rheumatic heart disease who underwent multiple valve replacement surgeries between 1988 and 2023 along with autotransplantation.
Case Report
In the year 1988, a 22-year-old female presented with dyspnea on exertion. Detailed clinical evaluation and echocardiography, revealed severe rheumatic mitral valve stenosis. Since she was unmarried at that time, it was decided to perform a Closed Mitral Valvotomy through a left thoracotomy. Her post-operative recovery was uneventful and she was discharged on the 7th day and was on digoxin and diuretics along with prophylactic penicillin therapy for rheumatic fever.
She went on to get married and in the year 1994, delivered a normal healthy boy. In 1998 (10 years post her closed mitral valvotomy) she was re-admitted for complaints of dyspnea on exertion.
Echocardiography revealed a recurrence of mitral stenosis along with mild tricuspid regurgitation. This time, she underwent an Open Mitral Valvotomy through a median sternotomy. She was continued on regular anti-failure medicines and antibiotic prophylaxis.
In the year 2005 (7 years post her Open Mitral Valvotomy) she again presented with dyspnea on exertion, echocardiography demonstrated severe mitral valve restenosis with moderate to severe tricuspid regurgitation, for which she underwent mitral valve replacement with a 27mm mechanical valve (TTK Chitra) using a KC 4239 prolene by continuous suturing technique, along with bicuspidisation of the Tricuspid valve. Her post-operative recovery was smooth and she was on regular follow-up.
In the year 2010 (5 years post her MVR), she presented with fever and on detailed evaluation with blood cultures confirmed bacterial endocarditis of the mitral valve secondary to urinary tract infection. She also had hypothyroidism, bronchial asthma, and congestive hepatomegaly. Her weight had reduced from 45kgs to 37.9kgs, her heart rate was 104 bpm and blood pressure was 120/56 mm Hg and her prosthetic heart valve click was audible. Detailed echocardiography revealed severe aortic stenosis with moderate aortic regurgitation, bacterial endocarditis of the prosthetic mitral valve, and severe tricuspid regurgitation. Given her cardiomegaly, bacterial endocarditis, and cardiac failure, it was decided to take her up for a triple valve replacement. Following median sternotomy, due to severe adhesions as a result of her previous surgeries and the additional finding of giant left and right atria, to reduce the surgical time and for better exposure of the intra-cardiac anatomy, it was decided to perform an autotransplant. Her core body temperature was cooled to 28oCelsius. The heart was arrested using one dose of cold blood cardioplegia given antegrade through the ascending aorta. The aorta, SVC, IVC, and MPA were clamped and divided, following which, the heart was removed from the thoracic cavity leaving a cuff of left atrial tissue around the 4 pulmonary veins. Since the heart was in a basin fully immersed in crushed ice, cardioplegia was not repeated. All the 3 valves (aortic, tricuspid, and mitral prosthesis) were excised and replaced using a 27mm mitral valve, 29mm tricuspid valve, and 21mm aortic valve (TTK Chitra) using a KC 4239 prolene, continuous suturing technique, along with aortic root enlargement using a bovine pericardial patch. The heart was re-implanted into the thoracic cavity by suturing the floor of the LA, Aorta, SVC, IVC, and MPA using appropriate prolene sutures. The total bypass time was 2hrs and 13mins and the total cross-clamp time was 50 mins. Her post-operative recovery was uneventful and she was electively ventilated for 24 hours. Since the hemostasis was achieved well with an empty thoracic cavity, post-operative bleeding was minimal. She had a remarkable recovery with improvement in her cardiac function, and regression of her hepatomegaly and dilated veins in the neck, chest, and abdominal wall that had almost completely disappeared by the time of her discharge on the 13th postoperative day.
She came for her review in 2023, after a total of 35 years following her initial surgery and she is doing well (Figure 1).
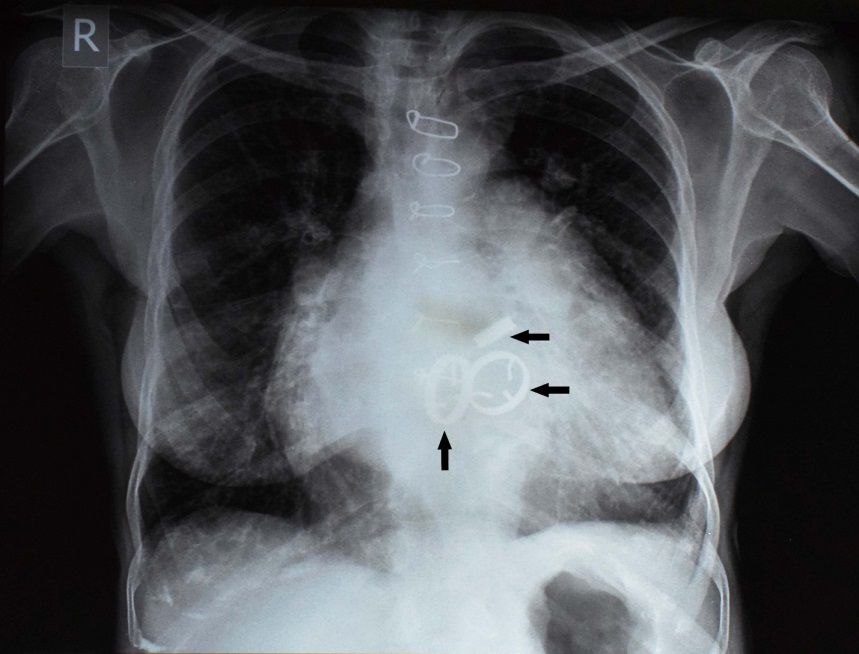
Chest PA – 58yrs/F. Figure 1: Arrows indicating 3 metal prosthetic valves (aortic, mitral, tricuspid) in-situ.
Discussion
The novelty of this case report is that it documents the history of all types of mitral valve surgery starting from Closed Mitral Valvotomy to an Open Mitral Valvotomy to a valve replacement to a re-replacement of her mitral valve all in the same patient done by a single surgeon. Another uniqueness of this case report is that our literature search suggests that she may be the only patient who is a long-term survivor of mitral valve surgery with a follow-up of 35 years after the initial surgery [10].
Furthermore, this article may represent the only case of a triple valve replacement using an auto transplant technique. It also highlights the advantages of performing an auto transplant in a patient who requires multiple valve replacements in one single sitting. The main advantages of the autotransplant in this particular case were that only one cardioplegia was required for the entire procedure and the surgical exposure of all three valves was excellent since the heart was explanted from the thoracic cavity and the heart could be manipulated in any direction hence, facilitated the valve replacements to be completed quickly. Although auto transplants are usually performed in cases of large cardiac tumors that require extensive dissection, this case report provides yet another indication for performing an auto transplant, in patients requiring multiple simultaneous valve replacements in a single surgical procedure [11, 12, 13].
Conclusion
This case emphasizes the benefits of auto- transplantation in the patient with all valve replacements. It also points out that this could be the first and longest case report where the patient is healthy after undergoing triple valve replacements as well as auto-transplantation. Since the patient was initially diagnosed with RHD which can be detected by echocardiography and prevented by modern innovations through vaccines, better disease management and customized surgical approaches are suggested that can improve the lifetime expectancy of patients with RHD and multiple valve failures.
Conflict of Interest
The authors have nothing to disclose about commercial support. No funding was received from any grant/company. Fully informed written consent was obtained from the patient to publish the data, without disclosing the identity/ any personal information.
References
-
What We Do (2024) Rheumatic Heart Disease. World Heart Federation.
-
Watkins DA, Johnson CO, Colquhoun SM, Karthikeyan G, Beaton A, et al. (2017) Global, Regional, and National Burden of Rheumatic Heart Disease, 1990-2015. N Engl J Med 377(8): 713-722.
-
Aremu OO, Samuels P, Jermy S, Lumngwena EN, Mutithu D, et al. (2021) Cardiovascular imaging modalities in the diagnosis and management of rheumatic heart disease. Int J Cardiol 325: 176-185.
-
Rwebembera J, Marangou J, Mwita JC, Mocumbi AO, Mota C, et al. (2023) World Heart Federation guidelines for the echocardiographic diagnosis of rheumatic heart disease. Nature Reviews Cardiology 21(4): 250-263.
-
Ralph AP, Currie BJ (2022) Therapeutics for rheumatic fever and rheumatic heart disease. Aust Prescr 45(4): 104-112.
-
Fu G, Zhou Z, Huang S, Chen G, Liang M, et al. (2021) Mitral Valve Surgery in Patients With Rheumatic Heart Disease: Repair vs. Replacement. Front Cardiovasc Med 8.
-
Jia S, Han J, Jiang W, Zhang H (2023) Triple valve repair for a patient with complex rheumatic-heart valvular disease: A case report. Asian J Surg 46(11): 5043-5045.
-
Russell EA, Tran L, Baker RA, Bennetts JS, Brown A, et al. (2014) A review of valve surgery for rheumatic heart disease in Australia. BMC Cardiovasc Disord 14(1): 134.
-
Bhandari S, Subramanyam K, Trehan N (2007) Valvular heart disease: diagnosis and management. J Assoc Physicians India 55: 575-584.
-
McDonald C, Dallimore D, Oates M, Shekar K, Thomson B (2018) Unplanned Autotransplantation for Complex Multi-Valve Replacement in a Super Morbid Obese Female: The Challenge of Intraoperative Decision Making. J Extra Corpor Technol 50(4): 248-251.
-
Zamora E, Ruyra X, Valle V (2008) Osteosarcoma in left atrium treated with autotransplant. Eur Heart J 29(19): 2446-2446.
-
Hussain ST, Sepulveda E, Desai MY, Pettersson GB, Gillinov AM (2016) Successful Re-Repeat Resection of Primary Left Atrial Sarcoma After Previous Tumor Resection and Cardiac Autotransplant Procedures. Ann Thorac Surg 102(3): e227-e228.
-
Ramlawi B, Al-jabbari O, Blau LN, Davies MG, Bruckner BA, et al. (2014) Autotransplantation for the Resection of Complex Left Heart Tumors. Ann Thorac Surg 98(3): 863-868.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review