Contribution of Pharmaceutical Interventions in the Therapeutic Monitoring of Renal Transplants under Tacrolimus: Experience of the Pharmacovigilance Service at Ehu Oran-Algeria
The clinical pharmacy approach consists of a direct pharmaceutical intervention “PI†on the prescription, based on the pharmaceutical analysis of the latter, proposing, if necessary, modifications of the drug therapy. It is accompanied by pharmaceutical advice and the targeted dissemination of information to the prescriber. The objective of this work is to evaluate the pharmaceutical analysis and its impact on the improvement of the drug treatment of the kidney transplant under Tacrolimus. This is a descriptive retrospective study, over a period of three months, of Tacrolimus-treated kidney transplant recipients who received therapeutic monitoring at the EHU pharmacovigilance department Oran- Algeria. The collection of information was based on the analysis of patient file summary sheets using a PI form prepared by the Therapeutic Opinion Service Unit. For the pharmaceutical analysis of prescriptions, various bibliographic references have been used: VIDALExpert®, Drugs.com, THERIAQUE,... The study involved 60 kidney transplant recipients aged 16 to 55 with a sex ratio of 1: 1. The most common age group was 30 to 40 years old. The majority of cases treated came from the kidney transplant unit (80%) for a transplant exceeding one year (85%). Only 8% of the renal transplant recipients studied was switched to Ciclosporin following the onset of side effects. The problems detected are mainly related to drug interactions (48.35%), followed by overdose (36.65%) and underdosing (11.65%). Most AMIs is of low severity (82%). The most common drug combination was: Tacrolimus + Cellcept + Corticoid + antihypertensive (46.70%). Among the observed side effects, the most common were: increased tacrolemia (35.15%), increased muscle IA and rash at equal percentages (22.45%). The most common pharmaceutical intervention was to re-administer Tacrolimus and recheck tacrolemia in 32% of cases. It was accepted by clinicians in 86.65% of the cases studied. Pharmaceutical intervention in the context of therapeutic monitoring allows, after a careful pharmacotherapeutic analysis, to identify the existing problems and to propose thereafter appropriate therapeutic opinions.
Introduction
Immunosuppressive drugs used in transplantation include those used in the immediate environment of transplantation when the patient is hospitalized, from those once the patient returns home. Drug treatment should solve the problem of graft rejection and / or graft- versus-host disease [1]. Because of their low therapeutic index and the high intra- and inter individual variability that characterize their pharmacokinetics, calcineurin inhibitors require regular therapeutic monitoring aimed at preventing graft rejection and their toxicity.
The clinical pharmacy approach consists of a direct pharmaceutical intervention on the prescription, based on its pharmaceutical analysis, proposing, if necessary, modifications of the drug therapy [2]. It is accompanied by pharmaceutical advice and the targeted dissemination of information to the prescriber. The objective of this work is to evaluate the pharmaceutical analysis and its impact on the improvement of the drug treatment of the kidney transplant under Tacrolimus.
Materials and Methods
This is a descriptive retrospective study, over a period of three months, focused on the records of renal transplant patients treated with Tacrolimus who have benefited from therapeutic monitoring in the pharmacovigilance department at the Oran EHU - Algeria.
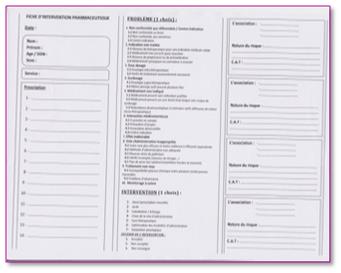
The collection of information was based on the analysis of patient record summary sheets using a PI sheet (Figure 1) developed by the Therapeutic Opinion Service Unit. For the pharmaceutical analysis of prescriptions, various bibliographical references have been used (the VIDALExpert® dictionary, the prescribe journal, the websites: Drugs.com, THERIAQUE, ...).
Results and Discussion
Our study was conducted on 60 renal transplant patients treated with Tacrolimus, with a sex ration of 1:1. Their age ranged between 16 and 55 years with an average age of 35.5 years and a slight predominance of the age group [30 - 40 years]. 79.25% of patients had a weight less than or equal to 75Kg. Of the 60 patients studied, 82% were followed at the kidney transplant unit and 11.70% at the Nephrology department. 85% of the patients studied had a transplant that is more than a year old.
Only 8.30% of the study population was switched to Ciclosporin following the onset of digestive side effects.
The results we have obtained show that out of 94 prescriptions analyzed, corresponding to 60 kidney transplant recipients, 186 problems were identified, i.e. an average of 3.1 problems per prescription. This means that these patients are at high iatrogenic risk given the importance of their essentially immunosuppressive medication.
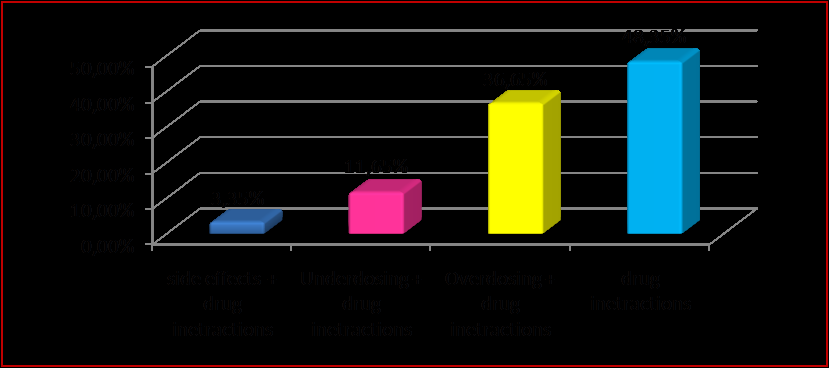
These detected problems are mainly related to drug interactions (48.35%), followed by overdose (36.65%) and under dosing (11.65%). Considering drug interactions, they represent the most common problem in our study, because renal transplant patients are polymedicated (Figure 2).
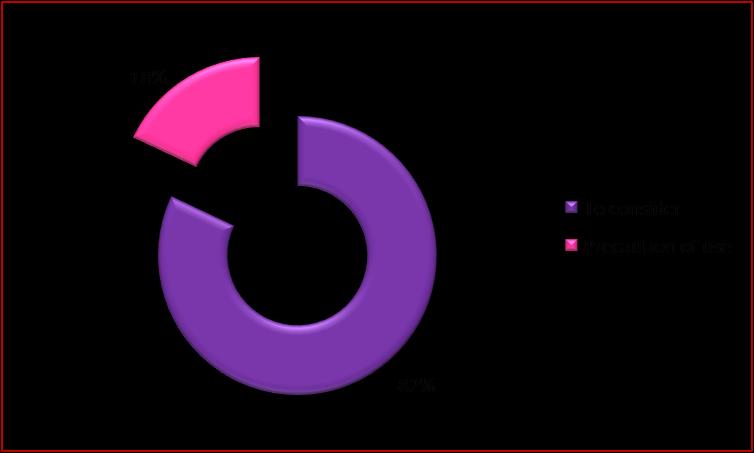
Most drug interactions are of low severity (82%), essentially the risk of increased adverse effects of associated drugs. Being essential drugs for these patients, it was recommended to monitor the occurrence of one of these undesirable effects. These results are superior to those found by Venardet, et al. in 2005 on the validation of hospital prescriptions where they found that 30,9% of the problems concerned drug interactions [3]. These data underscore the importance of medicament interactions analysis, which can have many clinical consequences (Figure 3).
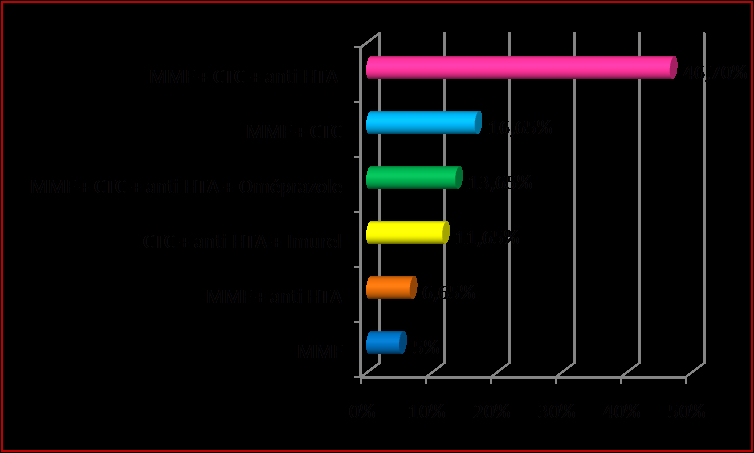
The most common drug combination was: Tacrolimus + Cellcept + Corticoid + antihypertensive (46.70%) (Figure 4).
Immunosuppressive therapy, the example of Tacrolimus, causes a lot of side effects. A study conducted in Nantes shows that 37.7% of PIs are due to the occurrence of adverse drug reactions, half of which has generated therapeutic optimization by the hospital pharmacist [4, 5, 6].
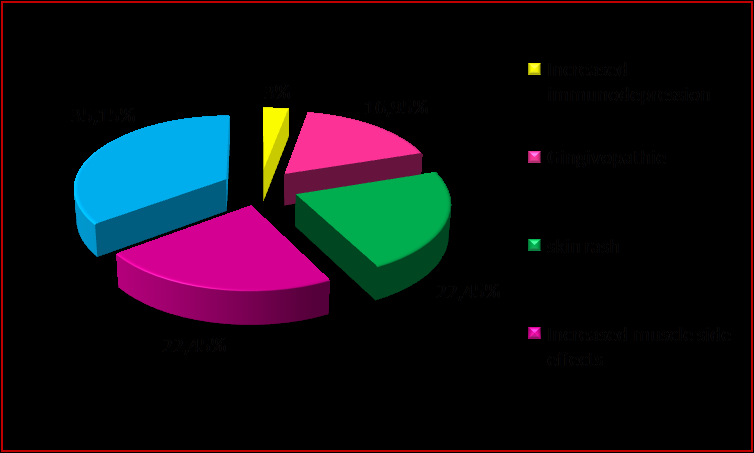
Regarding the side effects observed the most frequent were: increased tacrolemia (35.15%), increased muscle side effects and rash at identical percentages (22.45%). Being dose-dependent, these effects are related to often high concentrations. They can be corrected by a simple dose reduction. In other cases, they persist despite the decrease of the latter because of the combination of several factors: physiological (renal failure), family history of diabetes, association with other drugs with the same effect (Figure 5) [7, 8].
The proposal of therapeutic follow-up with readministration of Tacrolimusa constituted, after pharmaco-therapeutic analysis, the important part of the IPs emitted (32%). PIs concerning the need to monitor renal function (20%) were issued with the objective of nephrotoxicity problems related to immunosuppressive therapy.
Dose adjustment was also recommended in 20% of cases. Through these results, PI seems to play a key role in dose adjustment based on clinical and pharmacokinetic data (Figure 6).
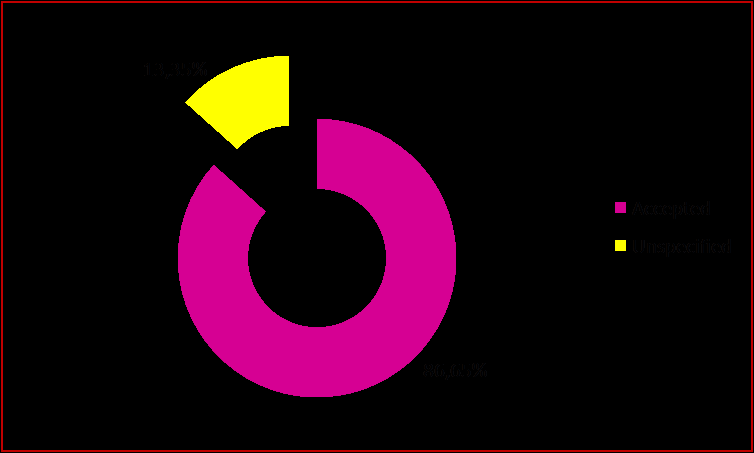
![Figure 6: Distribution by PI type. The acceptance of PIs by clinicians, a relevant factor in the quality of these, was observed in 86.65% of the cases studied and unspecified in the rest of the cases. In addition, several factors can contribute to PI acceptance, such as direct communication of results with the clinician. Our estimate of PI acceptance by prescribers is close to published estimates (90% rate). It is lower than the rate published by Bedouch, et al. (47.1%) in 2005 in his study on the dissemination of PIs in the context of a clinical pharmacy activity (Figure 7) [9-11].](/fulltextimages/2673/fig_6.png)
Figure 6: Distribution by PI type. The acceptance of PIs by clinicians, a relevant factor in the quality of these, was observed in 86.65% of the cases studied and unspecified in the rest of the cases. In addition, several factors can contribute to PI acceptance, such as direct communication of results with the clinician. Our estimate of PI acceptance by prescribers is close to published estimates (90% rate). It is lower than the rate published by Bedouch, et al. (47.1%) in 2005 in his study on the dissemination of PIs in the context of a clinical pharmacy activity (Figure 7) [9, 10, 11].
This work has highlighted the interest of pharmaceutical interventions in the management of renal transplant patients after pharmaco-therapeutic analysis of drug prescriptions. However, it has many potential limitations, namely:
- Restricted selection of kidney transplant recipients monitored at the Pharmacovigilance department at the EHU Oran-Algeria.
- Difficulty comparing pharmaceutical interventions acceptance results with literature data given the non- similarity of the methodology and the study population.
Conclusion
Pharmaceutical intervention in the context of therapeutic monitoring allows, after a careful pharmaco- therapeutic analysis, to identify the existing problems and to propose thereafter appropriate therapeutic opinions. A multicenter, larger patient population study representative of the nationally-inpatient population will provide statistically more significant and reliable results for PI's contribution to the management of kidney transplant under Tacrolimus.
References
-
Skalli S, Nouvel M, Faudel A, Fougère S, Parat S, et al. (2013) Renal transplantation and immunosuppressants: the part of the clinical pharmacist in the therapeutic management. Journal de Pharmacie Clinique 34(4): 201-218.
-
Calop J (1994) Clinical and therapeutic pharmacy. 3rd (Edn.), pp: 11.
-
Vernardet S, Bossaert S, Livrozet A, Bridge E, Charpiat B (2005) Pharmaceutical validation of hospital prescriptions: intervention and analysis over five years. Presse Med 34(14): 990-996.
-
Glock S (2013) Management of the transplanted organ patient: cross-views of pharmacists and patients and setting up pharmaceutical interviews. University of Lorraine, pp: 54-55.
-
Canivet S (2009) Contribution of the pharmacodynamic follow-up of immunosuppressors in organ transplantation. Toulouse.
-
Garnier S (2007) Clinical pharmacy in practice: creation of a training tool for internal and pharmacy students. University of Nancy, pp: 3.
-
Spinexine A (2003) Clinical pharmacy, a new pharmaceutical orientation serving patients: realization abroad and possibility in Belgium. 122: 127-139.
-
Bond CA, Raehl CL (2007) Clinical pharmacy services, pharmacy staffing and hospital mortality rates. Pharmacotherapy 27(4): 481-493.
-
Martini M (2010) Improvement of the medication management of patients and professional pharmaceutical practices: the quality of pharmaceutical analysis of drug treatments at the Luneville hospital. pp: 23.
-
Bedouch P, Allenet B, Labarere J, Brudieu E, Chen C (2005) Dissemination of pharmaceutical opinions in the context of a clinical pharmacy activity in a care unit. Therapy 60: 515-522.
-
Abramowicz D, Wissing KM, Broeders N (2000) Immunosuppression strategies in renal transplantation at the beginning of the third millennium. Adv Nephrol Necker Hosp 30: 9-28.
- Reconstruction of Nasal Defect Using a Local Flap Based in the Nanoperforants Concept: A Case Report
- Transplant Tourism in Japan: Insights from Nationwide Surveys and Emerging Ethical Challenges
- The Challenge of Peritoneal Vaginoplasty in Transgender Women: Review Literature and Personal Perspectives
- Algorithmic Paternalism: Autonomy Versus Automation
- Dermatoscopy in Gorlin Syndrome: Avoiding the Disfigurement in Patients
- How Artificial Intelligence is Ushering in a New Era of Innovation in General and Plastic Surgery: A Short Communication