Ronaldo Pontes’s in Block Resection Abdominoplasty Technique
Introduction: Abdominoplasty is a procedure not only with aesthetic characteristics, but also of structural reconstruction of the abdominal wall. Objective: The purpose of this study is to show the author’s experience in abdominoplasties, focusing on the aesthetic results of the scar and the evolution of these patients using the techniques of in block resection of Professor Ronaldo Pontes (RP). Method: The study was a series retrospective case of 124 patients, between March 2014 and March 2017, submitted to in block abdominoplasties RP technique. Results: In our series, it showed a minimal incidence of complications found with the RP Block technique, compared to those found in the literature, and also demonstrated a small number of cases of scaring disturbances.
Introduction
The first to use the expression abdominal lipectomy was Kelly [1] in 1889, where he performed transverse dermoadipous excision including the umbilicus.
Abdominoplasty is one of the most commonly performed aesthetic procedures that encompass not only aesthetic features but also structural reconstruction of the abdominal wall [2].
Due to the number of variations and modifications of abdominoplasty procedures, it is critical to select the appropriate technique based on patient characteristics to minimize postoperative morbidity and disability while providing a desirable and predictable outcome [3].
Initially, abdominoplasties were performed, characterized by a low incision, a cranial flap dissection, treatment of rectus abdominis diastasis, caudal traction of the flap, resection of the excess of tissue, transposition of the umbilicus and wound closure.
This type of procedure often resulted in asymmetric scar due to flap traction irregularity. In the adipose abdomen, this problem was aggravated by the difficulty of supporting an extremely heavy flap during dissection [4, 5].
For this reason, in the early 60's, a resection of the previously marked flap with a block dissection was performed, which would facilitate the surgical procedure, providing better control over the bleeding, as well as reducing the operative time. With the improvement of the technique and to tailor it for different cases, in 1971, four types of block resection were conceived and its application in countless cases, always following the same principle [4].
The aim of this article is to show our experience with this abominoplasty technique, focusing on the aesthetic results of the scar and the evolution of these patients applying the techniques of In Block Resection of Professor Ronaldo Pontes.
Method
The study was a retrospective observational series, performed through data collection of medical records, comprising a total of 124 patients, 122 female and 2 male, who underwent block abdominoplasty surgery (Figure 1), performed by the technique described by Professor Doctor Ronaldo Pontes (RP), from March 2014 to March 2017, applying the different types of resection techniques described (Chart 1).
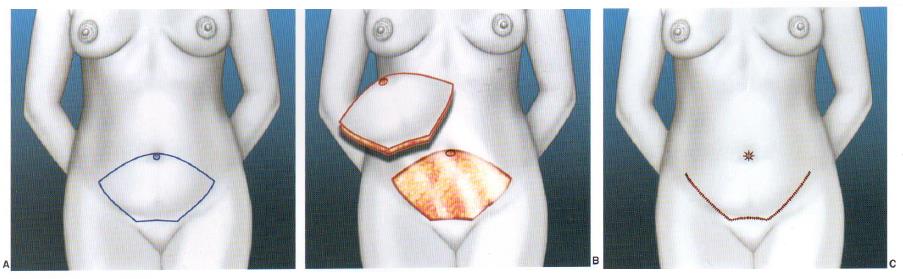
Type III (RP3): Indicated exclusively for patients with high umbilical scar and infra-umbilical flaccidity. The marking is identical to that of Type II, except that the umbilical scar is sectioned at its base, and after cranial dissection and plication of the rectus abdominis, it is reinserted below its original point, with the lowering of the umbilicus about 2 cm. Type IV (RP4): Indicated for patients with supra and infra umbilical laxity, in which there is no indication of other variants. The marking is similar to type I, but the ellipse's cranial outline passes just below the umbilical scar, where it later has its original point closed longitudinally, as it is not included in the area to be resected. Then the flap descends normally and the umbilicus is transposed similar to a typical abdominoplasty (RP1), resulting in an inverted T-incision. Vertical: For cases where there is a previous supra umbilical vertical scar or in cases with skin redundancy in which the cost-benefit favors the existence of the vertical scar.
In the abdominoplasty techniques, the adhesion stiches of Professor Baroudi were used.
- Block abdomen incision marking (RP technique) with patient in standing and lying down positions
- Fitting intermittent compression boots
- Patient in horizontal supine position with asepsis and antisepsis, placement of sterile fields under general aponeurotic system
12. omphaloplasty, resulting in Equilateral Triangle (directing to the pubis)Síntese do retalho em três planos 13. Dressing of the sergica wounds * 0.9% saline solution with 20ml of Xylocaine 2%, 20ml of Ropivacaine and 1ml of Adrenaline 1: 1000 ** Technique used in the forms of RP1, RP2 and RP4. In RP3, the umbilicus is detached of the aponeurosis. Chart 1: Surgical Technique of Block Abdominoplasty.
Inclusion criteria were: patients over 18 and under 65 years old with supraumbilical and infra-umbilical skin flaccidity, presence of rectus abdominis diastasis, satisfied offspring, and body mass index above 20.
| BMI | Frequencies | Percentages | ||||||
|---|---|---|---|---|---|---|---|---|
| 20-22 | 10.40% | |||||||
| 23-25 | 48 | 38.80% | ||||||
| 26-28 | 35 | 28.20% | ||||||
| 29-31 | 15 | 12.10% | ||||||
| 32-34 | 8 | 6.50% | ||||||
| ≥35 | 5 | 4.00% |
Table 1: Relation of the Body Mass Index of the patients.
All patients underwent a detailed physical examination and thoroughly discussed with patients all the implications of abdominal plastic surgery, as well as guidance on fertility, time required for recovery, ambulation with some abdominal flexion, length of stay and the use of Suction drains. Routine laboratory Postoperatively, all patients underwent prophylaxis for deep venous thrombosis, with the use of pneumatic boots, peri- and postoperatively, and postoperative use of enoxaparin. Informed consent was provided and photographic documentation was performed on a routine basis.
| Types of | Frequencies | Percentages | ||
|---|---|---|---|---|
| Comorbidities | ||||
| No known comorbidities | 84 | 67.74% | ||
| Diabetes | 4 | 3.22% | ||
| High Blood Pressure | 15 | 12.09% | ||
| Hypothyroidism | 8 | 6.45% | ||
| Others | 15 | 12.09% |
Table 2: Frequency of Comorbidities.
The patients were followed daily on the first two postoperative days and weekly during the first month, followed once a month. The aesthetic outcome was evaluated after 6 months of surgery.
Results
The average age was 44.5 years (range 18 to 63 years). The average surgical time was 154 minutes (range 100 to
250 minutes). The drains were removed on average 7 days. The surgeries associated with abdominoplasty are presented in chart 3.
| Ages | Frequencies | Percentage | ||||||
|---|---|---|---|---|---|---|---|---|
| 18 to 30 years old | 20 | 16,12 % | ||||||
| 31 to 45 years old | 67 | 54% | ||||||
| 46 to 60 years old | 33 | 27% | ||||||
| 61 to 65 years old | 4 | 3% |
Table 3: Frequency of Ages.
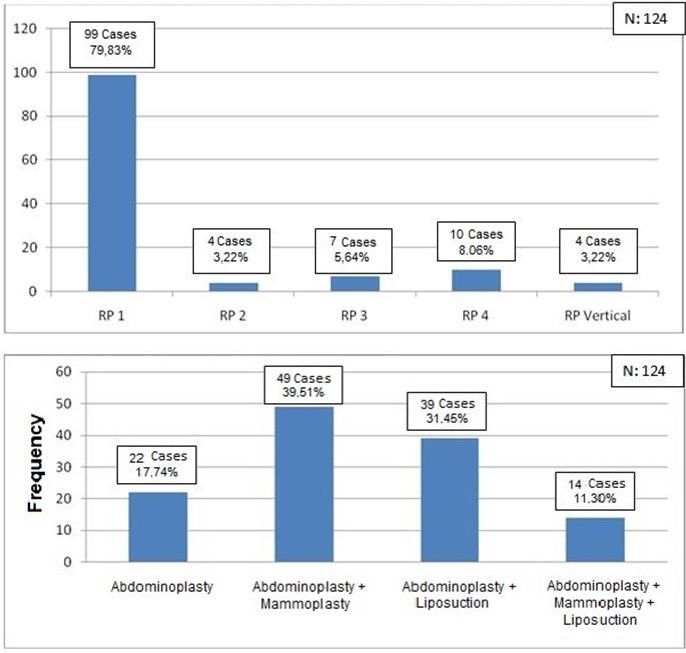
Chart 2: Frequency of the different Variants of the In Block Resection Abdominoplasty RP in 3years.
of scaring disturbances (Table 5). The operated patients had a high degree of morphological and functional satisfaction.
| Types of Complications | Frequencies | Literature | ||||||
|---|---|---|---|---|---|---|---|---|
| Seromas | 1.61 % (2 cases) | 1,0 a 4,2% | ||||||
| Hematomas | 0.80 % (1 cases) | 5,0 a 6,1% | ||||||
| Surgical site infections | 0.00 % (0 cases) | 2,2 a 7,3% | ||||||
| Flap necrosis or distress | 0.80 % (1 cases) | 4,8 a 6,0% | ||||||
| Deep venous thrombosis | 0.00 % (0 cases) | 1,0 a 1,1% | ||||||
| Pulmonary embolism | 0.00 % (0 cases) | 0,5 a 0.8% |
Table 4: Frequencies of the Complications.
| Types of complications | Frequencies (n = 124) | Percentages | ||||||
|---|---|---|---|---|---|---|---|---|
| Without complications | 118 | 95.18% | ||||||
| Wound dehiscence | 0 | 0.00% | ||||||
| Hypertrophic scars | 2 | 1.61% | ||||||
| Keloid scars | 1 | 0.80% |
Table 5: Scaring disturbances.




Procedure for Ensuring Ethical Aspects
The study was conducted with data obtained from the surgeon's personal file. To obtain the list of patients who met the inclusion and exclusion criteria, there was no direct contact with the patients, so no informed consent was required. The identity of the patients participating in the study remained anonymous, since their identities were not necessary for the study.
Authorization for the display of the preoperative and postoperative fotos where granted by the patients.
We agree to abide by the ethical and moral principles that should govern all research involving humans, such as: The Helsinki Declaration, Belmont Report, Good Clinical Practice and the Ethical Standards and Criteria set forth in the confidentiality codes of ethics and / or laws. current. We also undertake to respect the confidentiality of data obtained from clinical records and any other method of data collection, and not to disclose information to identify study subjects.
Authorizations were requested from the authorities of Hospital Niteroi D'Or, as well as the review and approval of the Institutional Ethics Committee.
Discussion
The methods and approaches differ greatly from each other, thus leaving the literature reviews [6, 7, 8, 9] and comparisons with controversial retrospective studies. In this way, we try to circumvent the discrepancies by defining the facts with a simple objective, comparing the most common complications with our evidence.
As the practice of combined surgeries increases the risk of morbidity, consequently increasing: length of stay, intra and postoperative blood transfusion index, incidence of thromboembolism and serious infections [10, 11, 12]. We believe that common sense is fundamental to evaluate the cost-effectiveness of the procedure, knowing the safety of performing combined surgeries and abdominoplasty.
The advantages of the Ronaldo Pontes technique are simplifying resection, eliminating the need to hold a very long and heavy flap during dissection, facilitating bleeding control, ensuring better symmetry of the resulting scar, dramatically reducing procedure time, stimulating better planning. As the flap to be resected is usually marked on the day before or on the ward, it reduces the time of use of the operating room and the anesthesia time of the patient [4]. Thus, greatly minimizing cases of complications and scarring defects.
We emphasize that, among all complications, deep venous thrombosis and pulmonary embolism are the most dramatic. The incidence of DVT in patients undergoing general surgery has been reported in about 6 to 12% [9] and pulmonary embolism in 1.5% 9. These events were avoided in our cases by knowing their pathophysiology and preventive measures and short surgical time [13, 14, 15].
Conclusion
The described technique and its variants meet the need for several types of cases and guarantee safe and effective surgeries, being a reproducible technique.
Prevention of hematomas and seromas becomes effective, due to strict hemostasis, the use of flap adhesion stiches and the use of suction drains, preventing through prolonged active drainage, minimizing the rates of these complications associated with proper postoperative orientations.
Therefore, knowledge of the pathophysiology, prophylactic measures and the use of a technique with shorter surgical time reduce the risk of thromboembolic events, consequently the drastic pulmonary embolism. Thus, we fulfill our duties towards patients, ensuring their safety and delivering a high degree of morphological and functional satisfaction.
References
-
Kelly HA (1910) Excision of the flat abdominal wall lipectomy. Surg Gynec Obstet 10: 229.
-
Callia W (1963) Contribuição para o estudo da correção cirúrgica do abdome pêndulo e globoso- técnica original [Tese de doutorado]. São Paulo: Universidade de São Paulo, Faculdade de Medicina.
-
Grazer FM (1973) Abdominoplasty. Plast Reconstr Surg 51(6): 617-623.
-
Pontes Ronaldo (2004) Abdominoplastia - Ressecção em Bloco e sua Aplicação em Lifting de Coxa e Torsoplastia.
-
Pitanguy I (2000) Evaluation of body contouring surgery today: a 30-year perspective. Plast Reconstr Surg 105(4): 1499-1516.
-
Dillerud E (1990) Abdominoplasty combined with suction lipoplasty: a study of complications, revisions and risk factors in 487 cases. Ann Plast Surg 25(5): 333-343.
-
Nurkim MV, Mendonça LB, Martins PAM, Silva JLB, Martins PDE (2002) Incidência de hematoma e seroma em abdominoplastia com e sem drenos. Rev Soc Bras Cir Plast 17: 69-74.
-
Jaimovich CA, Mazzarone F, Parra JFN, Pitanguy I (1999) Semiology of the Abdominal Wall: its Value in Planning Abdominoplasty. Rev Soc Bras Cir Plas 14(3): 21-50.
-
Abs R (2000) Thromboemboliques en chirurgie plastique: revue de la literature et proposition d´un algorithme de prophylaxie. Ann Chir Plast Esthet 45(6): 604-609.
-
Anger J, Baruzzi AC, Knobel E (2003) U A Prevention Protocol for Deep Vein Thrombosis in Plastic Surgery. Rev Bras Cir Plast 18(1): 51-54.
-
Weinmann EE, Salzman EW (1994) Deep-vein thrombosis. N Engl J Med 331(24): 1630-1641.
-
Jatene PR, Jatene MC, Barbosa AL (2005) Abdominoplasty: clinical experience, complications and review of literature. Rev Bras Cir Plast 20(2): 65- 71.
-
Almeida EG, Almeida GL (2008) Abdominoplastia: Estudo Retrospectivo. Rev Bras Cir Plast 23(1): 1-10.
-
Oliverira EA, Valera F, Monte AL , Lopez C (2008) Prevention of Seroma in Lipossuction Associated Abdominoplasty Without Active Drainage. Rev Soc Bras Cir Plást 23(1): 41-47.
-
Arantes EL, Rosique RG, Rosique MJ, Mélega JM (2009) Is there need for drains to prevent seroma in abdominoplasty with adhesion suture? Rev Bras Cir Plást 24(4): 521-524.
- Reconstruction of Nasal Defect Using a Local Flap Based in the Nanoperforants Concept: A Case Report
- Transplant Tourism in Japan: Insights from Nationwide Surveys and Emerging Ethical Challenges
- The Challenge of Peritoneal Vaginoplasty in Transgender Women: Review Literature and Personal Perspectives
- Algorithmic Paternalism: Autonomy Versus Automation
- Dermatoscopy in Gorlin Syndrome: Avoiding the Disfigurement in Patients
- How Artificial Intelligence is Ushering in a New Era of Innovation in General and Plastic Surgery: A Short Communication