“Fleur De Lys†Muscle-Aponeurotic Plication in Abdominoplasty and Lipoabdominoplasty
Muscle-aponeurotic plication is an essential component in abdominoplasty and lipoabdominoplasty because it allows correcting flaccidity and improves abdominal wall deformity. This plication can be vertical, horizontal, or mixed. Vertical plication is the most commonly used form, although there is a growing tendency to use horizontal plication as part of the TULUA technique. We propose the mixed plication in the form of “Fleur de Lys†as a more appropriate form of correction since it corrects the vertical and horizontal flaccidity. Material and methods: From February 2015 to May 2019, we operated abdominoplasty and lipoabdominoplasty patients associated with the "Fleur de Lys†plication. Results: In this period, 144 “Fleur de Lys†plications have been performed in 140 women (97.2%) and four men (2.8%), with ages ranging from 25 to 63 years (average 48 years). One hundred thirty-six cases (94.4%) were primary surgeries, and 8 cases (5.56%) were patients with previous abdominoplasty. We had no complications related to the increase in intra-abdominal pressure, only small dehiscences in 5 cases (3.5%) and seroma in 10 cases (7.8%). Conclusion: The mixed plication technique in “Fleur de Lys†is a more anatomical manner of correcting the muscleaponeurotic flaccidity because it fixes the vertical and horizontal flaccidity present in operated abdominoplasty and lipoabdominoplasty patients; its execution is technically easy and the results obtained are as expected, with minimal complications.
Introduction
The abdominal wall is the muscle-aponeurotic structure responsible for protecting the visceral content and maintaining the shape of the abdominal contour. Alterations in their tone and integrity, associated with skin flaccidity produce abdominal contour deformity of varying degrees [1, 2]. There is a direct relationship between excess abdominal skin and the degree of muscle- aponeurotic deformity; therefore, patients with great skin flaccidity have defects that are more complex in the abdominal muscle-aponeurotic system [1].
The abdominoplasty and lipoabdominoplasty are procedures that allow correcting the skin flaccidity and repairing the muscle-aponeurotic deformities of the abdominal wall; these corrections are carried out by various techniques of muscle-aponeurotic plication, which are classified into three types: vertical, horizontal, and mixed. The vertical plication is the most used and is performed along the rectus abdominal muscles [1, 2, 3], several variants have been described, and sometimes, it is associated with plication of the external oblique muscles [3]. On the other hand, the horizontal plication is performed perpendicular to the straight muscles and allows correcting the vertical elongation of the abdominal wall. It was initiated in 1996, with Gerow, et al. [4] proposing aggressive transverse plication at the waist level; later, plication techniques in the infraumbilical region were described such as that described by Villegas in the abdominoplasty with TULUA technique [5].
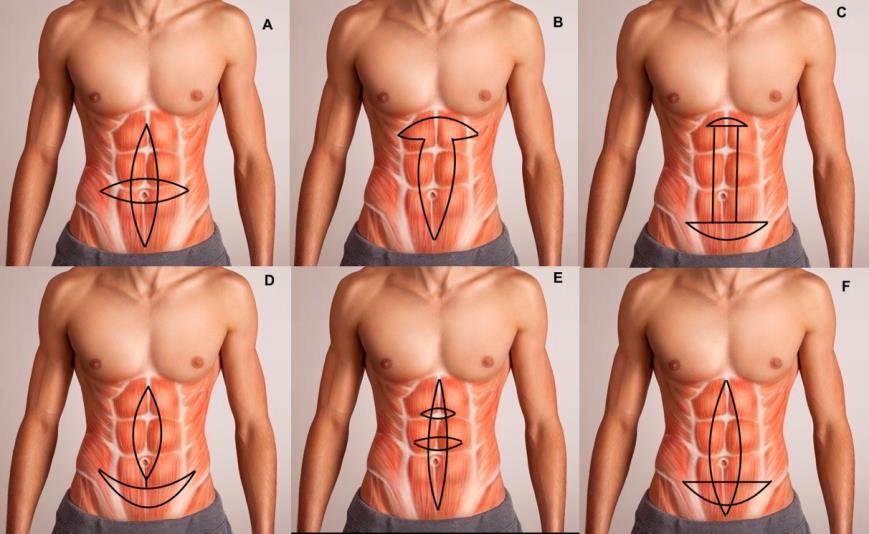
The mixed plication, unlike the previous ones, allows correcting both the vertical and horizontal elongation of the muscle-aponeurotic system of the abdominal wall, because it combines the techniques of vertical and horizontal plication at the same time. Jackson and Downie initially described it in 1978 [6] who performed periumbilical plication as a “four-legged helix." Later in 1990, Marques, et al. [7] described the “T-shaped plication” with vertical plication associated with a horizontal plication in the upper abdomen designed to correct epigastric prominence. Likewise, in 1999, Abramo, et al. [8] proposed the “horizontal H plication” as a vertical plication associated with a small horizontal plication in epigastrium and a more extensive plication in hypogastrium. Subsequently, in 2004 Cardenas & García [9] proposed the “anchor plication” as a vertical plication in the upper and middle abdomen, associated with a horizontal plication in the lower abdomen, but without intersection of both. In 2005, Serra-Renom, et al. [10] proposed the vertical plication associated with 1 or 2 small “horizontal plications on-demand” in the upper and middle abdomen, and in 2019 Soares published the “crossbow plication” [11] which consists of a vertical and a horizontal plication that intersect at the level of the lower abdomen (Figure 1).
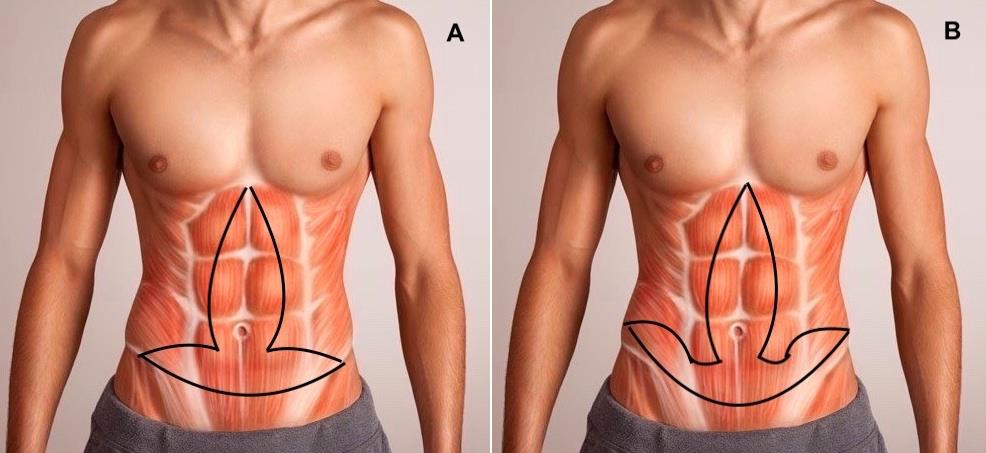
We began the mixed plication in 2014. The first cases were in patients who underwent “anchor” abdominoplasty, who due to their great skin flaccidity and aponeurotic muscle required corrections in a vertical and horizontal direction at the same time. In these patients, this type of plication not only helped correct more effectively the great vertical and horizontal flaccidity of their abdominal wall but also contributed to decrease the dead space by approaching the flaps to suture them with less tension. The initial design was in the form of “Tumi”, similar to that proposed by Marques, et al. [7], although unlike him, we performed the horizontal plication in the lower abdomen (Figure 2A); however, this initial design produced a lot of tension at the intersection of both plications in the lower midline, making it challenging to execute. Also, the design of the horizontal plication did not allow correcting the muscle-aponeurotic flaccidity at the level of the iliac fossa. For these reasons, in 2015, the proposal was redesigned, establishing the plication in the form of “Fleur de Lys” for all these cases (Figure 2B).
Material and Methods
From February 2015 to May 2019, operated abdominoplasty and lipoabdominoplasty patients associated with muscle-aponeurotic plication with the technique described were included in the study, excluding cases with the vertical or horizontal plication technique performed individually. The database was reviewed to obtain a list of patients undergoing abdominoplasty or lipoabdominoplasty with the described plications, and then we reviewed their medical and photographic records.
Lipoabdominoplasty patients were operated in a private clinic, and patients with abdominoplasty without
Surgical Technique
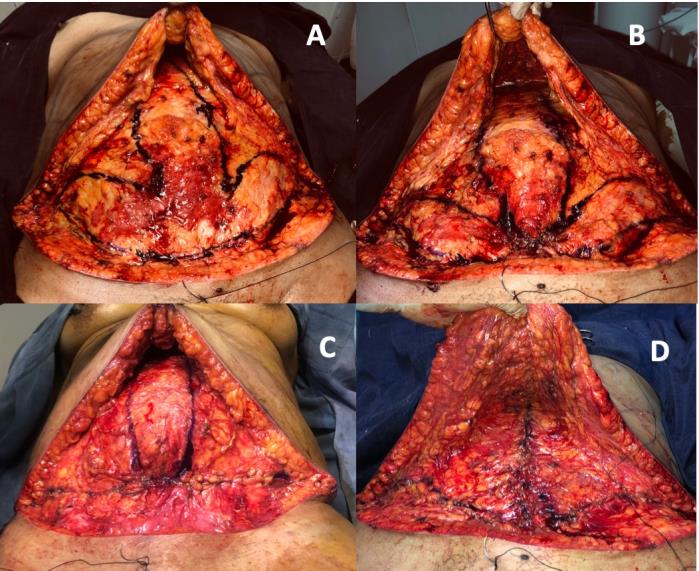
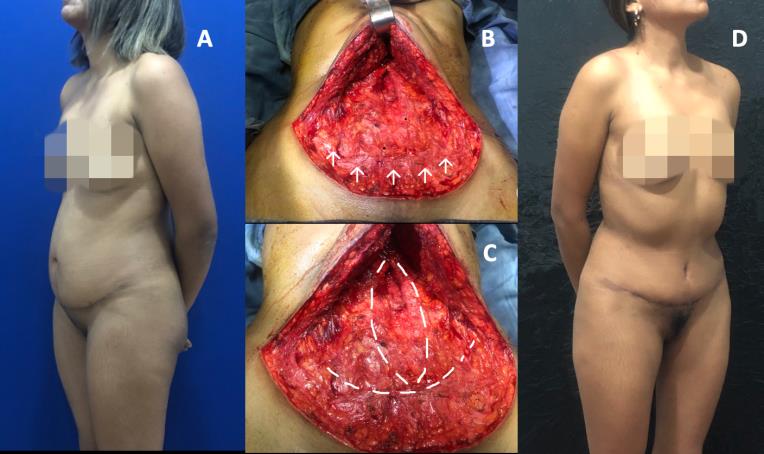
Patients underwent operation under general or regional anesthesia. After dissection, elevation, and resection of the abdominal flap, the vertical and horizontal plication is drawn on the exposed abdominal wall, following the proposed design (Figure 3A). Next, the plication is performed using non-absorbable Nylon 1/0 sutures, with separate points in the form of “inverted X," such that the knots are buried.
It begins with the horizontal plication with the first point that joins the lower poles of the vertical plication, with the lower midpoint of the horizontal plication at the pubic level (Figure 3B), continues until completing this horizontal plication (Figure 3C) after the vertical plication is performed (Figure 3D). Occasionally, we perform an additional continuous suture, using vicryl 2/0, along the vertical plication to reinforce and avoid palpation of knots. Finally, the closure of the abdominal flaps is performed in two planes, and it ends with umbilicoplasty or neoumbilicoplasty, as appropriate.
| Primary | Secondary | Total | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Abdominoplasty | 7 | 0 | 7 | ||||||
| Lipoabdominoplasty | 76 | 5 | 81 | ||||||
| Minilipoabdominoplasty | 16 | 1 | 17 | ||||||
| Anchor abdominoplasty | 8 | 0 | 8 | ||||||
| Anchor lipoabdominoplasty | 29 | 2 | 31 | ||||||
| Total | 136 | 8 | 144 |
Table 1: Characteristics of the types of body contour surgeries associated with plicatures in "Fleur de Lys".

Results
In the study period, 144 “fleur de Lys” plications have been performed in 140 women (97.2%) and 4 men (2.8%), with ages ranging from 25 to 63 years (average 48 years). 136 cases (94.4%) were primary surgeries, and 8 cases (5.56%) were secondary abdominoplasty or re- abdominoplasty, of which 5 cases with prior abdominoplasty, 2 cases with prior anchor lipoabdominoplasty, and 1 case of mini-abdominoplasty using previous TULUA technique.
129 plications (89.6%) were performed in the same number of cases of lipoabdominoplasty in its different variants and 15 cases (10.4%) associated with abdominoplasty without liposuction. In all cases, except mini-abdominoplasty, neoumbilicoplasty was performed (127 cases). All 129 cases of lipoabdominoplasty plications were operated at a local clinic, under epidural anesthesia with catheter: 81 plications (62.8%) in patients with lipoabdominoplasty with lower abdominal incision, 17 plications (13.2%) in patients with lipominiabdominoplasty with navel replacement and 31 plications (24%) in patients with anchor lipoabdominoplasty. The 15 cases of abdominoplasty without liposuction were performed in the Department of Plastic Surgery and Burns at the “Guillermo Almenara Irigoyen” Hospital, all of them under general anesthesia, 07 plications associated with abdominoplasty with lower incision and 08 cases associated with anchor abdominoplasty.
There were no complications related to the increase in intra-abdominal pressure. Small dehiscences were described in 5 cases (3.5%) and seroma in 10 cases (7.8%) that were managed conservatively without affecting the final results.
Discussion
Patients who request abdominoplasty tend to have excess skin and abdominal wall flaccidity of varying degrees. However, in the beginning, the abdominoplasty was limited only to the management of skin flaccidity without giving importance to the navel or the abdominal wall. In 1967, Callia introduced the medial plication of the straight muscles to improve the abdominal contour in post-pregnancy patients, since then, various techniques and plication variants involving the fascia of the straight muscles [1, 2], and in some cases, the external oblique muscles [3] have been proposed.
The proposed technique is a mixed plication in the form of “fleur de Lys” combining horizontal and vertical plication to anatomically correct the flaccidity of the abdominal wall, as this flaccidity is resulting from the elongation of the fibers from the muscle-aponeurotic system both vertically as horizontally. The technique can be used in various types of abdominoplasty and any degree of flaccidity, even in severe cases, avoiding the use of meshes and/or plications of the external oblique muscles. Another advantage offered by this technique is that it allows reducing the dead space (especially in anchor abdominoplasty), and it approximates the resection edges, which allows a closure with less tension. Similarly, the horizontal plication produces pubic lifting as described by Andre FS [12], and its lateral design allows the medial and inferior advance of oblique muscles to allow a better contour in these areas.
In 1978, Jackson and Downie introduced the mixed plication [6] performed at the periumbilical level in the form of a “four-legged helix." Later in 1990, Marques, et al. [7] described a “T-shaped plication”; and years later in 1999, Abramo, et al. [8] proposed the “horizontal H plication”, and in 2015, Serra-Renom, et al. [10] proposed the vertical plication with horizontal plications “on- demand”. Although these proposals achieved the aim of correcting the muscle-aponeurotic flaccidity, their execution requires an extensive dissection of the abdominal flap, going against the current principles of the abdominoplasty, which is the limited dissection of the abdominal flap that allows preserving the perforating vessels, and decreasing the risk of necrosis and seromas.
Likewise, in 2004, Cardenas & García [9], and 2019, Soares [11] published mixed plication techniques similar to the one proposed in this work, although with some visible differences. Thus, Cardenas & Garcia described an “anchor plication” consisting of a vertical plication in the upper and middle abdomen, associated with a horizontal plication in the lower part, without intersection of both, as two independent plications, unlike our proposal, which is continuous and non-independent. On the other hand, Soares published the “crossbow plication." In this proposal, the vertical plication intersects and exceeds the horizontal plication at the lower abdomen level; this is the difference with our proposal. Also, the location of the horizontal plication is more superior, and the design of the horizontal plication does not efficiently corrects flaccidity in that area.
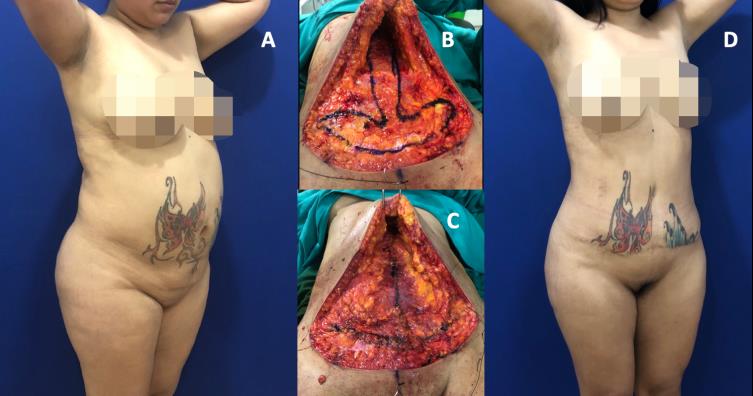
Our priority is to perform the horizontal plication first. At the end of this phase, we observe an abdominal “bulge” (Figure 3C), which occurs above this plication and is directly proportional to the degree of diastasis of the rectus muscles. We consider that this occurs due to the rearrangement of the visceral content in the new reduced abdominal space, the same that is observed when we perform abdominoplasty with muscular diastasis using only horizontal plication, such as the TULUA technique, as occurred in the case of Figure 6, which was corrected with a complementary vertical plication becoming a mixed plication like the one we propose in this study.
On the other hand, we must consider that the horizontal plication displaces the position of the navel in a caudal direction; therefore, the possibility of performing neoumbilicoplasty should be considered in the applicable cases. For several years, we have carried out neoumbilicoplasty in all our cases of abdominoplasty and lipoabdominoplasty requiring umbilical transposition. This allows not only to reconstruct a new navel by discarding the original but also to optimize the execution of the vertical plication since it can be performed uniformly without the fear of “hanging” the umbilical stem, as we have shown in the clinical cases presented.
We have not registered any associated cases of breathing problems or other related to increased intra- abdominal pressure. Under normal conditions, the intra- abdominal pressure is subatmospheric, although the muscle-aponeurotic plication is a procedure that increases the intra-abdominal pressure by reducing the volume of the continent. Cases of symptoms of abdominal hypertension, respiratory compromise, and gastroesophageal reflux have been reported in patients with rectus plication. However, few studies have measured intra-abdominal pressure and correlated with symptomatology, with contradictory results. Losken, et al. [13] has shown a significant increase in intra-abdominal pressure (20 mmHg) after the use of the TRAM flap, especially bipediculate, with primary closure of the abdominal wall, which exhibited severe thromboembolism problems. In contrast, Al-Basti, et al. [14] carried out intra-abdominal pressure measurements before and after plication in obese and multiparous patients. They found an increase in intra-abdominal pressure, but without clinical significance; in the same way, through intravesical measurements, Huang, et al. [15] concluded that there is an increase in intra- abdominal pressure during the abdominoplasty, but it was not clinically significant. Marin VJA, et al. [16] have shown that the increase of intra-abdominal pressure post- abdominoplasty with plication is less than 10 mmHg. Usually, pressures up to 10 mmHg or 13.6 cm H2O do not cause any hemodynamic or respiratory changes and pressures greater than 20 mmHg are considered intra- abdominal hypertension.
Seroma is the most common postoperative complication in abdominoplasty and lipoabdominoplasty. For prevention, various surgical alternatives have made developed, although their effectiveness is variable. Seretis, et al. [17] conducted a systematic review and meta-analysis to evaluate the effects of preventive surgical measures on patients with abdominoplasty, finding strong positive evidence in their reduction using preservation of the fascia scarp, tissue adhesives or progressive tension sutures. Other published works reinforce the importance of preserving the fascia of Scarpa in the prevention of seroma [18, 19] among others; although Tourani, et al. [20] based on an anatomical study of abdominal lymphatic vessels in fresh cadavers conclude that the preservation of the Scarpa fascia in abdominoplasty would not preserve the lower abdominal lymphatic collectors, and, Har-Shai, et al. [21] they argue that the presence of an "adhesive interface" between the deep adipose compartment and the abdominal flap could explain the contradiction between the clinical success of seroma reduction with the preservation of the scarp fascia and the new find in the abdominal wall lymphatic anatomy. The plicature technique proposed in this work does not allow preserving of the fascia of Scarpa. However, our incidence of seromas (7.8%) is similar to the average of abdominoplasty patients using prevention measures, and who have been published [17]; in fact, these positive results are due to two reasons: on the one hand, the decrease of dead space by the double musculoaponeurotic plication, and, to the adhesion points or "progressive tension sutures" of the abdominal flap to the fascia that we perform in all our cases. The effectiveness of these adhesion points has been demonstrated in various published works [22, 23] and systematic and meta-Analysis reviews [17, 24].
Conclusion
The mixed plication technique “Fleur de lys” is a more anatomical manner of correcting the muscle-aponeurotic flaccidity, because it corrects the vertical and horizontal flaccidity present in patients who will undergo abdominoplasty and lipoabdominoplasty; its execution is technically easy and the results obtained are as expected, with minimal complications.
References
-
Nahas FX, Ferreira LM (2010) Concepts on correction of musculoaponeurotic layer in abdominoplasty. Clin Plastic Surg 37(3): 527-538.
-
Barcelos FVT, Avelar LET, Bordoni LS, Barcelos RVT (2017) Análise anatomis da abdominoplastia. Rev Bras Cir Plast 32(2): 272-281.
-
Bozola AR (2013) Abdominoplastias: efectividade da classifiçao de Bozola e Psillakis – 27 anos de observaçao do autor. Rev Bras Cir Plást 28(4): 633- 642.
-
Gerow FJ, Walker LE, Spira M (1996) The French-line abdominoplasty. Ann Plast Surg 36(5): 530-535.
-
Villegas Alzate FJ (2011) Abdominoplasty without flap elevation, full liposuction, transverse infraumbilical plication and neoumbilicoplasty with skin graft (TULUA). Can J Plastic Surg 19: 95.
-
Jackson IT, Downie PA (1978) Abdominoplasty. The waistline stitch and other refinements. Plast Reconstr Surg 61(2): 180-183.
-
Marques A, Brenda E, Ishizuka MA, Abramo AC, Andrews JM (1990) Abdominoplasty: modified plication. Br J Plast Surg 43(4): 473-475.
-
Abramo AC, Casas SG, Oliveira VR, Marques A (1999) H-Shaped, double-contour plication in abdominoplasty. Aesthetic Plast Surg 23(4): 260-266.
-
Cardenas Restrepo JC, Garcia Gutierrez MM (2004) Abdominoplasty with anchor plication and complete lipoplasty. Aesthetic Surg J 24(5): 418-422.
-
Serra-Renom JM, Martinez-Teixido L, Serra-Mestre JM (2015) Abdominoplasty with Customized Transverse Musculoaponeurotic Plications. Plast Reconstr Surg 136(6): 741-749.
-
Soares FI (2019) Abdominal wall treatment with plication using the crossbow technique. Rev Bras Cir Plást 34(1): 23-30.
-
Andre FS (2009) Abdominoplastia e lifting do pubis. Rev Bras Cir Plást 24(3): 345-350.
-
Losken A, Carlson GW, Jones GE, Hultman CS, Culbertson JH, et al. (2002) Significance of intraabdominal compartment pressures following TRAM flap breast reconstruction and the correlation of results. Plast Reconstr Surg 109(7): 2257-2264.
-
Al-Basti JB, El-Khatib HA, Taha A, Sattar HA, Bener A (2004) Intraabdominal pressure after full abdominoplasty in obese multiparous patients. Plast Reconstr Surg 113(7): 2145-2150.
-
Huang G, Bajaj AK, Gupta S, Petersen F, Miles DA (2007) Increased intraabdominal pressure in abdominoplasty: Delineation of risk factors. Plast Reconstr Surg 119(4): 1319-1325.
-
Marin Valladolid JA, Saucedo Ortiz JA, Fuentes Orosco C, López Pérez S, Segura Castillo JL, et al. (2004) Variación de la presión intraabdominal causada por abdominoplastía en mujeres sanas. Rev Gastroenterol Mex 69(3): 156-161.
-
Seretis K, Goulis D, Demiri EC, Lykoudis EG (2017) Prevention of Seroma Formation Following Abdominoplasty: A Systematic Review and Meta- Analysis. Aesthet Surg J 37(3): 316-323.
-
Xiao X, Ye L (2017) Efficacy and Safety of Scarpa Fascia Preservation during Abdominoplasty: A Systematic Review and Meta-analysis. Aesthetic Plast Surg 41(3): 585-590.
-
Iannelli A, Ciancio F, Annoscia P, Michelangelo V, Rosario Emanuele P, et al. (2018) Abdominoplasty with "Scarpa Fascia" preservation: Case Report. Int J Surg Case Rep 47: 100-103.
-
Tourani SS, Taylor GI, Ashton MW (2015) Scarpa Fascia Preservation in Abdominoplasty: Does It Preserve the Lymphatics?. Plast Reconstr Surg 136(2): 258-262.
-
Har-Shai L, Hayun Y, Barel E, Ad-El DD (2018) Scarpa Fascia and Abdominal Wall Deep Adipose Compartment Preservation in Abdominoplasty- Current Clinical and Anatomical Review. Harefuah 157(2): 87-90.
-
Macias LH, Kwon E, Gould DJ, Spring MA, Stevens WG (2016) Decrease in Seroma Rate After Adopting Progressive Tension Sutures Without Drains: A Single Surgery Center Experience of 451 Abdominoplasties Over 7 Years. Aesthet Surg J 36(9): 1029-1035.
-
Bromley M, Marrou W, Charles-de-Sa L (2018) Evaluation of the Number of Progressive Tension Sutures Needed to Prevent Seroma in Abdominoplasty with Drains: A Single-Blind, Prospective, Comparative, Randomized Clinical Trial. Aesthetic Plast Surg 42(6): 1600-1608.
-
Jabbour S, Awaida C, Mhawej R, Bassilios Habre S, Nasr M (2017) Does the Addition of Progressive Tension Sutures to Drains Reduce Seroma Incidence After Abdominoplasty? A Systematic Review and Meta-Analysis. Aesthet Surg J 37(4): 440-447.
- Reconstruction of Nasal Defect Using a Local Flap Based in the Nanoperforants Concept: A Case Report
- Transplant Tourism in Japan: Insights from Nationwide Surveys and Emerging Ethical Challenges
- The Challenge of Peritoneal Vaginoplasty in Transgender Women: Review Literature and Personal Perspectives
- Algorithmic Paternalism: Autonomy Versus Automation
- Dermatoscopy in Gorlin Syndrome: Avoiding the Disfigurement in Patients
- How Artificial Intelligence is Ushering in a New Era of Innovation in General and Plastic Surgery: A Short Communication