Treatment of Pathological Scars with Nanofat Lipograft at the Hermanos Ameijeiras Hospital
Introduction: The healing is the result of the natural restoration of the organism before a corporal aggression produced by a surgical wound or trauma. Poor wound and injury healing represents a functional and aesthetic problem, which is why it deserves special attention. Objective: To evaluate the aesthetic results of the treatment of pathological scars with lipotransfer by nanofat. Method: A prospective longitudinal and descriptive study was carried out with 8 patients from Plastic Surgery Hospital ‘‘Hermanos Ameijeiras†with pathological scars, who received lipotransfer treatment by Coleman method and processing of adipose tissue by nanofat from January to June 2020. Results: 8 patients with ages between 25 and 50 years with a mean age of 39 years were included. The female sex predominated with 75%. The predominant skin color was grades 3 and 5 of the Fitzpatrick classification, both with 50%. The most frequent etiologies were post acne, postoperative and injection scars of allogenic substances, all with 25%. The main anatomical locations were the facial region and in the breasts with 3 patients each, followed by 2 cases in the gluteal region. The postoperative aesthetic results at three months were 100% good, observing macroscopic and microscopic positive changes with the nanograft. No patient presented complications. Conclusions: The treatment of pathological scars with lipotransfer by nanofat is an available, simple and reproducible option that offers objective improvement of the scar with rapid recovery.
Introduction
Healing is the product of natural restoration in the face of bodily aggression that causes a wound or trauma. Poor wound and injury healing represents a functional and aesthetic problem, which is why it deserves special attention [1].
The conventional surgical treatment to eliminate pathological scars is excision and plasty. However, scars after radiation therapy and allogenosis usually cover large areas, which are not amenable to direct excision. Scar depression, adherence to deep planes, and retraction are common features of abnormal scars that are associated with pain and possible functional limitation. The surgical treatment indicated for its correction can be substituted or complemented with fat transfer [2, 3].
Adipose tissue is a great source of Mesenchymal Stem Cells (MSCs) useful in regenerative therapy.1 The benefits of fat transfer are discussed in multiple articles, showing the effect of filling achieved and graft survival. However, the changes experienced by the skin after autologous adipose graft (biorepair, regenerative and revitalizing effect caused by MSCs) are not studied.2 However; the publications to date only use the visual clinical assessment of skin appearance to show the results of this procedure [4, 5, 6, 7].
The present research aims to evaluate the results of the treatment of pathological scars in eight patients of different etiologies and anatomical locations three months after carrying out the lipotransfer by nanofat.
Method
In the period between January and June 2020, at the Hermanos Ameijeiras Clinical Surgical Hospital, lipotransference was performed on eight patients with pathological scars according to the Coleman method and processing of the adipose tissue by nanofat [3, 8].
The following variables were analyzed: Age: In completed years. Sex: Female or Male. Skin color: Evaluated according to Fitzpatrick classification [9]: - Grade 1: Red hair, blond, very light skin. - Grade 2: Light to medium hair, light to medium skin. - Grade 3: Medium colored hair, medium to olive skin. - Grade 4: Dark hair, dark olive to light brown skin. - Grade 5: Dark hair, brown skin. - Grade 6: Dark hair, very dark skin.
Pathological scars: Hypertrophic, keloid, retractable,
dyschromic or enlarged scar.
Etiology: Post-acne, post-traumatic, postsurgical scars, post- radiotherapy radiodermatitis and iatrogenic allogenosis due to injection of allogenic substances.
Anatomical locations: Facial region, breasts and gluteal.
Aesthetic results: They were evaluated three months after having performed the procedure, taking into account the following parameters:
- Skin changes: Clinical evolution with photographic studies that show little visible scars.
- Pathological changes: Observed with the Skin Analyusis Apparatus Use Lens X 200 surface microscope, showing improvement in elasticity, resistance and hydration of the skin of the treated scar.
- Absence of complications: They did not present any complications.
- Patient satisfaction: Satisfied or not satisfied.
According to the fulfillment of the previous parameters, the following were considered:
- Good: If they met the 4 previous criteria.
- Regular: When they met between 3 and 2 of the previous criteria.
- Bad: When only 1 of the above criteria was met.
Complications: Categorized in presence or absence during follow-up.
Preoperative Period All patients underwent a complete blood count and hemochemistry that were within normal limits. Those operated on from March 2020 also underwent a PCR for Covid 19 with a negative report. In addition, all of them underwent a photographic study.
Surgical Technique The surgical technique was performed in an outpatient surgery regime and complying with the international standards of the ERAS protocols [10]. The patient was placed in the desired position, depending on the donor and recipient anatomical regions to be treated. Asepsis and antisepsis, placement of sterile drapes, infiltration of local anesthesia and then Klein solution [3] were performed in the donor region of the graft 100 ml of adipose tissue were liposuctioned and processed by the nanofat method [8]. The filtering result (50 ml) was injected into the scar to be treated with a 0.7 mm diameter infiltration cannula with a single distal hole. The filtrate was deposited in micro-shots in the subdermal plane uniformly fanned out and backtraced. A simple skin stitch was made in the donor region, covered with a sterile dressing and a medium compression girdle was placed.
Postoperative Period Relative rest, prophylactic antibiotic therapy, and analgesics for one week. Follow-up by outpatient consultation and photographic study at a week, 1 month and 3 months. Techniques and Procedures Information collection: The information sources were the interview and the clinical examination. With prior consent to participation, the surgical intervention was carried out according to the characteristics of each case. The patients were evaluated one week, one month and 3 months after the surgery.
Information Processing and Analysis: The data obtained were collected in a Microsoft Excel database and processed using the SPSS statistical package, version 23.0. Age was summarized as mean and standard deviation, minimum and maximum. The variables measured on a qualitative scale were summarized in absolute and relative frequencies (percentages). The results were presented in tables.
The research was approved and approved by the Scientific Council and by the Medical Ethics Commission of the institution. It was carried out in accordance with current national principles of medical ethics and the principles of the Declaration of Helsinki.
Results
Eight patients who received treatment of pathological scars with lipotransfer by nanofat are presented in the Plastic Surgery service of the Hermanos Ameijeiras Hospital, in the period from January 2020 to June 2020.
The patients were in the age range between 25 and 50 years, with a mean age of 39 years. As shown in Table 1, female patients predominated with 6 cases. Regarding the color of the skin, the Fitzpatrick classification [9] was used with a predominance of grades 3 and 5, both with 50%. The most frequent etiologies were post-acne, postsurgical scars and iatrogenic postalogenosis with 25% of the cases in each one. The most affected anatomical regions were the facial region and the breasts with 3 patients (37.5%) each.
| Sex | Skin color | Etiology | Anatomical Location | NO. | % |
|---|---|---|---|---|---|
| Male | Grade 3 | Post-acne | Facial | 2 | 25 |
| Female | Grade 5 | Post-traumatic | Facial | 1 | 12.5 |
| Female | Grade 5 | Postsurgical | Breasts | 2 | 25 |
| Female | Grade 5 | Posr-radiotherapy | Breasts | 1 | 12.5 |
| Female | Grade 3 | Postalagenosis | Gluteal | 2 | 25 |
In the photographic studies they showed pathological scars before and after the nanofat fat transfer treatment at 3 months. Significant positive macroscopic and microscopic changes in scars and skin condition were observed (Figures 1-4).
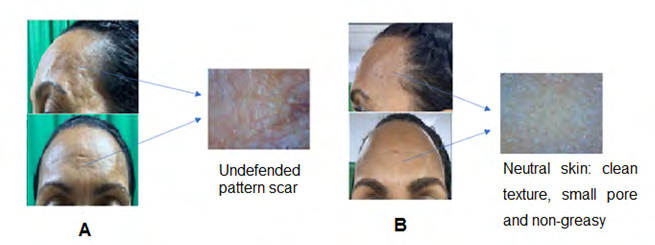
Figure 1: A. Preoperative: Female patient with a left superciliary post-traumatic scar of 3cm in length, depressed and adhered to deep planes associated with sign of aging. B. Postoperative: Little visible scar, with a filing effect that made it flat and uniform. In addition, reduction of wrinkles and depth of furrows, disappearance of marionette lines, smooth, resistant and flexible skin.
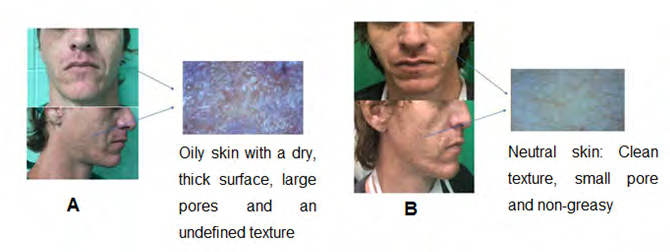
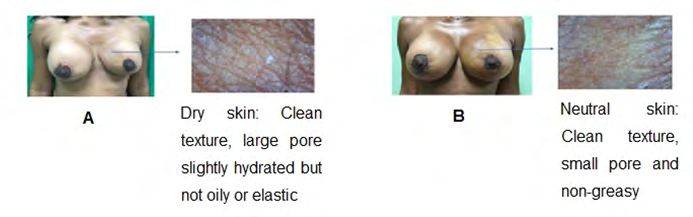
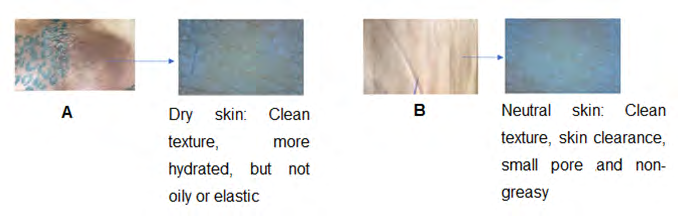
The postoperative aesthetic results at three months were good in 100% of the patients, demonstrated by the macroscopic and microscopic positive changes of the scars with a single application of the nanograft and the satisfaction of all patients.
No patient presented complications.
Discussion
Healthy skin is uniform in color, smooth in texture, well hydrated, adequately sensitive to touch, pressure and temperature. When the natural barrier of the skin is altered, both its protective function and its healthy appearance are compromised with an evident loss of moisture and elasticity, resulting in dry, rough, cracked and flabby skin [11].
Any wound can form a pathological scar, but within the local factors that alter healing as a result of the repair of massive tissue damage are: acne [12], radiation therapy (radiodermatitis) [13] and the injection of allogenic substances that both by compression and by immune response hyperpigment and atrophy the epithelium [14]. Atrophic scars can also appear as a consequence of an inflammatory response to an initial injury as in the case of burns and insect bites, which end with the formation of fibrous tissue. Trauma, infection, and epithelial cysts are processes that generate atrophic scars. These appear in a depressed form, with their center inverted and rigid in appearance [12].
The exact cause of pathological scars is completely unknown, although local immune phenomena may exist. However, there are certain predisposing factors such as: age, race and certain anatomical regions of tension [15]. The literature proposes that pathological scars are more frequent in young patients, directly proportional to the pigmented skin race and are located mostly in the areas of the face, the chest and those that suffer a prolonged stimulus such as the gluteal regions, as evidenced in this study [15, 16].
Acne can leave different types of scars: bulging, depressed, ice pick, drawer. Scars develop when a wound does not heal properly and very little functional tissue forms, develops underneath the surrounding tissue, and creates a small visible indentation [12]. Induced damage in radiodermatitis is directly correlated with radiation dose and ranges from early transient ischemia, permanent erythema to necrosis and ulcers. Factors that contribute to skin toxicity are high radiation doses, repeated interventions, short intervals between exposures, size of the irradiated site, nutritional status, clear skin phototypes, systemic diseases, and drug use. Lesions are characterized by erythema, edema, burning, and itching. Then a reddish brown or hypopigmented spot appears that resolves spontaneously in several weeks. In a more advanced degree, intense erythema, edema, vesicles and superficial ulcers may appear that can lead to necrosis [13].
The injection of allogenic substances can locally cause inflammation, irregularity, edema, erythema, keloid scars, hyper- or hypopigmentations, ulcerations, hardening, necrosis, sclerosis, fibrosis and fistulas. In addition, due to mechanisms of compression, migration and immune response, they can cause necrosis in other deeper planes [17].
Stem cell-enriched adipose tissue transfer produces noticeable clinical changes on aged or damaged skin. In this aspect we can say that it restores skin vitality, recovers elastic consistency, improves skin thickness and vascularity, stimulates secretions, improves its color and appearance; as well as the regenerative effect, regulates dermoepidermal and immunomodulatory remodeling and delays skin degenerative changes [18].
Fat grafting plays a double role in the revision of scars. It has a mechanical function because the layers of fat correct depressed scars, release adhesions and can release trapped nerves and tendons. In addition, they have a biological function because the stem cells present in the fat improve local regeneration, hydration and vascularization, which can be particularly relevant in unstable scars. The process can fill in sunken areas caused by age, acne scars, disease, injury and atrophic scars, sunken and wide scars [19].
Both collagen and fibroblasts are abnormally abundant in scars, leading to scar hyperplasia or contracture. Clinical studies have reported that wrinkles at the recipient site are reduced, pores are narrowed, pigmentation decreases, and the skin is smoothed after autologous fat transplantation [20]. In the cases presented, the clinical and microscopic effect that this therapy causes at the skin level was evidenced. After lipofilling treatment of scars, the thickness, color and elasticity of the scar tissue normalizes and patient satisfaction increases.
In pigmentation, a lightening and homogeneity of color is appreciated since MSCs have apocrine function when they secrete cytokines, especially a tyrosine regulator that is directly related to and inhibits melanin synthesis [21]. With aging, the skin loses collagen, elastin and moisture-retaining glycosaminoglycans, which make it thinner and weaker [22]. External factors can also accelerate this process. MSCs have the potential to be used in anti-aging treatments, because they can produce proteins that give them the ability to replicate and maintain their stability. The greater the amplitude of the chromatin, the greater the expression of the traits affected by the genes within the cell and the MSCs can maintain an open profile with aging [23].
Regarding the dermoepidermal structure, the changes obtained with regenerative therapy have been limited to biostimulation with platelet-rich plasma and other substances of synthetic origin. There are no publications that address skin changes with the administration of adipose tissue derived stem cells obtained by nanofat. In the cases presented, the improvement in terms of hydration, viscosity, flexibility and smoothness of the skin are similar to those described by Isaza et al. with the use of platelet-rich plasma. However, it only provides growth factors responsible for stimulating MSCs and promoting tissue regeneration [24].
The use of the lipograft as a vehicle for MSCs in the treatment of scars and bloody areas was described in 1893 by Gustav Neuber [3, 25]. The physical properties of scars depend on the collagen fibers they contain. Its maturation implies a gradual loss of red color and hardness until it becomes whitish, soft and does not adhere to underlying structures. In 2018 Fan, et al. [26] used lipoinjection for keloids and hypertrophic scars, which shows a reduction in fibrosis and pain and an increase in their elasticity and flexibility. At present, the benefits of adipose grafts are known, which when injected under or into the skin improve its quality, repair the appearance, elasticity and alleviate the symptoms of different skin lesions such as: wrinkles, pigmentations and different scars, including excess scars [27]. The injected MSCs create a microenvironment in the tissue that stimulates the creation of new vessels, secretes growth factors and promotes the creation of new molecules that regulate collagen deposition and increase elastic elements, creating a physical structure more similar to normal tissues [27]. The cells and the implanted tissue increase the viability and quality of the scars, in addition they create a new matrix within the skin marks, improving the architecture of the dermis and increasing its functional capacity, which improves the quality of life of the patients [28].
The autotransplantation of fat is an alternative to combat the effects of radiotherapy on the tissues, increase their thickness and prepare them for the performance of secondary procedures such as the placement of prostheses in the breasts [29]. Its usefulness was described for the first time in 2007 by Gino Rigotti in irradiated tissues attributing the regenerative property of MSCs [3, 25]. Revascularization is carried out through the formation of neoanastomosis between the recipient tissue and the graft and is the main element for its survival [30]. The properties of MSCs achieve regeneration in areas that present post-radiation therapy changes with increased tissue thickness, relaxation and detachment of adherent scars, closure of bloody areas and greater elasticity of the skin, with lightening of the same [29].
Fat grafting is a very suitable treatment for filling depressions in the skin due to the loss of underlying tissue, whether due to burns, trauma or surgery. As it is an autologous product, it rules out the possibilities of immune rejection and reduces the incidence of complications, which did not occur in any of the previously described cases. The changes at the microscopic level that are clinically evident after fat transfer are demonstrated in this study.
Lipotransfer with adipose tissue processed by the nanofat method is a safe, economical and effective option for skin rejuvenation.
Conclusions
Nanofat fat transfer treatment of pathological scars is an available, simple and reproducible option that offers objective scar improvement with rapid recovery.
References
-
Sanchez JC, Romero C, Muñoz LV, Rivera RA (2016) Adipose organ, a metabolic and endocrine regulating rainbow. Rev Cub Endocrine 27(1): 105-119.
-
Dominguez Martin N, Hernandez Hermida Y (2016) Stem cells in regenerative medicine. Degree work. Complutense University.
-
Meruane M (2016) Lipoinjection: Basic concepts and clinical application. Revista Médica Clínica Las Condes 27(1): 93-106.
-
Menkes S, Luca M, Soldati G, Polla L (2020) Subcutaneous Injections of Nanofat Adipose-derived Stem Cell Grafting in Facial Rejuvenation. Plast Reconstr Surg Glob Open 8(1): e2550.
-
Uyulmaz S, Sanchez Macedo N, Rezaeian F, Giovanoli P, Lindenblatt N (2018) Nanofat Grafting for Scar Treatment and Skin Quality Improvement. Aesthet Surg J 38(4): 421-428.
-
Gentile P, Scioli MG, Bielli A, Orlandi A, Cervelli V (2017) Comparing different nanofat procedures on scars: role of the stromal vascular fraction and its clinical implications. Regen Med 12(8): 939-952.
-
Pallua N, Kim BS (2020) Microfat and Lipoconcentrate for the Treatment of Facial Scars. Clin Plast Surg 47(1): 139-145.
-
Tonnard P, Verpaele A, Carvas M (2020) Fat Grafting for Facial Rejuvenation with Nanofat Grafts. Clin Plast Surg 47(1): 53-62.
-
Fitzpatrick TB (1975) Soleil et peau. J Med Esthet 2: 33- 34.
-
Simpson JC, Bao X, Agarwala A (2019) Pain Management in Enhanced Recovery after Surgery (ERAS) Protocols. Clin Colon Rectal Surg 32(2): 121-128.
-
Cotofana S, Fratila A, Schenck T, Redka Swoboda W, Zilinsky I, et al. (2016) The Anatomy of the Aging Face: A Review. Facial Plast Surg 32(3): 253-260.
-
Clark A, Saric S, Sivamani (2018) Acne Scars: How Do We Grade Them?. Am J Clin Dermatol 19(2): 139-144.
-
Muñoz Muñoz R, Alfaro Orozco L, Martinez Felix M (2019) Radiodermatitis secondary to fluoroscopy. Report of a case. Dermatology CMQ 17(4): 269-271.
-
Tamayo Carbon AM, Castellanos Prada AR, Aveiro Robalo TR (2018) Iatrogenic allogenosis and rheumatic diseases. Rev Cub Reumatol 20(2): 1-6.
-
Soler Vaillant R, Mederos Curbelo ON (2018) Surgery. Generalities. ECIMED, Havana 6 (Pt 1): 57-68.
-
Fernandez PR, Mottura A (2021) Efficacy analysis of rigotomy associated with fat graft to improve scars. Cir Plast Iberolatinoam 47(1): 87-94.
-
Tamayo Carbon AM, Orozco Jaramillo MA, Posada Ruiz DA (2019) Adjuvant substances and adjuvant- induced inflammatory autoimmune syndrome. Case presentation. Panorama Cuba and Health 15(1): 59-64.
-
Tamayo Carbon AM, Bencosme Escarraman YY, Orozco Jaramillo MA, Posada Ruiz DA, Estevez del Toro MH (2020) Effects of lipografts in immune-caused lipoatrophies. Case presentation. Colombian Journal of Rheumatology. Online ahead of print.
-
Blanco Moredo E, Dunan Mesa L, Perez Ferrer M (2020) Lipotransfer: an alternative for the treatment of acquired facial deformity. Rev Inf Cient 99(1): 63-70.
-
Terren J (2019) Facial rejuvenation with own gauze. Plastic and aesthetic surgery.
-
Planas J, Muñoz J, Gonzalez D (2017) escription of a new closed system to process fat and to obtain nanofat: analysis of clinical and cytometric results. Cir Plast Iberolatinoam 43(1): 23-32.
-
Zouboulis C, Hoenig L (2019) Skin aging revisited. Clin Dermatol 37(4): 293-295.
-
Escalona Garrido C, Montoro Garcia B (2015) Molecular mechanisms associated with aging. Degree work. Complutense University.
-
Isaza CA, Henao J, Aranzazu J (2018) Regenerative Medicine: Fundamentals and Applications. Rev Med Risaralda 24(2): 119-124.
-
Rigotti G, Marchi A, Galie M, Baroni G, Benati D, et al. (2007) Clinical treatment of radiotherapy tissue damage by lipoaspirate transplant: a healing process mediated by adipose-derived adult stem cells. Plastic and reconstructive surgery 119(5): 1409-1422.
-
Fan D, Xia Q, Wu S, Ye S, Liu L, et al. (2018) Mesenchymal stem cells in the treatment of Cesarean section skin scars: study protocol for a randomized, controlled trial. Trials 19(1): 155.
-
Tamayo Carbon AM, Posada Ruiz DA, Orozco Jaramillo MA, Cairos Baez JN (2020) Keloid Scars; review and experience in a comprehensive treatment. Rev Panorama, Cuba and Health 15(3): 90-97.
-
Balmelli B, Mussi D, Canese J, Sandoval J (2018) Treatment of late sequels of scars in burns using the Fraction of the Vascular Stroma (SVF) derived from the adipose tissue from human lipoaspirates. Rev Salud Publica Parag 8(1): 27-34.
-
Maione L, Vinci V, Lisa A, Barbera F, Balia L, et al. (2018) Autologous fat graft in irradiated orbit postenucleation for retinoblastoma. Orbit 37(5): 344-347.
-
Vyas K, Vasconez H, Morrison S, Mogni B, Linton S, et al. (2020) Fat Graft Enrichment Strategies: A Systematic Review. Plast Reconstr Surg 145(3): 827-841.
- Reconstruction of Nasal Defect Using a Local Flap Based in the Nanoperforants Concept: A Case Report
- Transplant Tourism in Japan: Insights from Nationwide Surveys and Emerging Ethical Challenges
- The Challenge of Peritoneal Vaginoplasty in Transgender Women: Review Literature and Personal Perspectives
- Algorithmic Paternalism: Autonomy Versus Automation
- Dermatoscopy in Gorlin Syndrome: Avoiding the Disfigurement in Patients
- How Artificial Intelligence is Ushering in a New Era of Innovation in General and Plastic Surgery: A Short Communication