The New Concept of making the Excellent Result in Mastopexy
Background: Breast ptosis is one of the more common issues seen in cosmetic surgeons’ offices, particularly those performing a significant amount of aesthetic breast surgery. Patients with ptosis generally desire the same result – youthful and “perky†breasts. However, due to wide variations in breast volume and tissue quality, ultimate results vary with each patient, and as a result, preoperative management of expectations is critical. There are many surgical options that can be customized to patients’ needs, but these generally address repositioning of the glandular tissue and nipple areolar complex and management of skin excess. Scar patterns include circumareolar, circumvertical (including J or L scar variations), and inverted-T patterns. If author’s new concept can eliminate the remaining skin excess that occur from approximately preoperative markings of traditional mastopexy and can decrease the scar pattern (J or L scar variations and inverted-T patterns), they are interesting to bring an alternative to reduce complications and more satisfactory results. Objective: Author study the new concept of surgical techniques of mastopexy in severe ptotic breasts. The new concept is the changing steps of procedure that performs repositioning and reshaping of the glandular tissue and repositioning of nipple areolar complex before, follow by design and excise the excess skin flaps. Surgical result, main complications and patient satisfaction are evaluated. Methods: The study has performed in 11 patients who have severe ptotic breasts with author’s techniques of mastopexy since July 2017 to march 2018. The techniques including repositioning and reshaping of the glandular tissue and repositioning of nipple areolar complex, skin flaps are designed and excised accurately. Postoperative care makes as standard protocols. Results: Of 11 patients who underwent mastopexy with author’s techniques, all patients have symmetric, only short vertical scar and beautifully shaped breasts and 2 patients have superficial necrosis of skin which at junction of inferior edge of areola and vertical incision, both sides and right side respectively. Three breasts which have superficial skin necrosis, manage include death tissue was removed, dress wet wound every day and make delay primary wound closure in some areas. Nipple sensation is usually normal. Some patients have decrease sensation and fully recover within three months. Conclusion: Author’s surgical techniques change steps of standard mastopexy, as new concept for severe ptotic breast. Repositioning and reshaping of glandular tissue and repositioning of nipple areolar complex firstly, these will help surgeon design and excise the excess skin flaps more accurately. But surgeons do not over excise skin flap to prevent skin necrosis especially junction area. Accordingly, author’s technique can decrease frequent complications of mastopexy including asymmetry, improper of flap excision and undesired J or L, inverted T scar.
Introduction
Breast ptosis is one of the more common issues seen in cosmetic surgeons’ offices, particularly those performing a significant amount of aesthetic breast surgery. Breast ptosis presents in many forms and can be congenital in nature, or acquired due to causes such as aging, weight changes, and pregnancy. Patients with ptosis generally desire the same result – youthful and “perky” breasts. However, due to wide variations in breast volume and tissue quality, ultimate results vary with each patient, and as a result, preoperative management of expectations is critical. There are many surgical options that can be customized to patients’ needs, but these generally address repositioning of the glandular tissue and nipple areolar complex and management of skin excess. Scar patterns include circumareolar, circumvertical (including J or L scar variations), and inverted-T patterns. Pedicles can be designed from all directions and are independent of the scar pattern. If author’s new techniques can eliminate the remaining skin excess that occur from approximately preoperative markings of traditional mastopexy and can decrease the scar pattern (J or L scar variations and inverted-T patterns), they are interesting to bring an alternative to reduce complications and more satisfactory results.
Material and Methods
The author retrospectively analyzed 11 patients (all are females, mean age, 33.7 years; age range, 22 to 49 years) with severe ptotic breast and different breast volumes classified by small, normal, and hypertrophic breast between July 2017 to march 2018. The author studied the many types of breast ptosis and the surgical options chosen. The modified Regnault’s classification of breast ptosis was used [1]. To study the surgical results, patient satisfaction and postoperative complications in all patients, the surgical procedures were chosen as mastopexy or reduction mammoplasty with a new concept of procedures for patients with severe ptosis (Figure 1). The author performed the necessary procedure during tumescent anesthetic breast surgery (TABS) in an office- based surgical clinic.
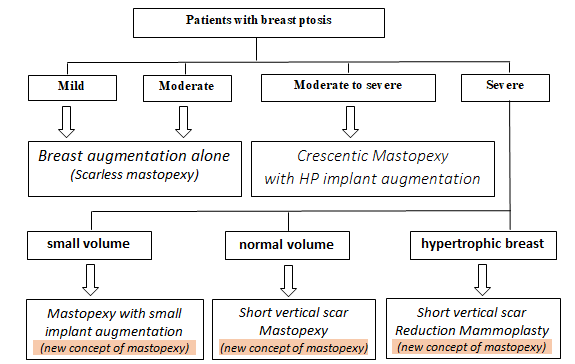
The management of patients with have severe ptosis and normal volume were managed by the short vertical scar mastopexy which is a new concept of procedures. New concept techniques enable the surgeon to more precise with the excision of the skin flap as breast tissue and NAC are repositioned and reshaped beforehand while the standard or traditional techniques of mastopexy make the excision of the planned skin flap (approximately) before and then reposition and/or reshape the breast tissue and reposition NAC at the end of the procedure [2, 3, 4, 5]. The excess skin can be excised accurately after subcutaneous tissue and breast tissues removed properly and completely. The excised skin must be ample but not too much to prevent tight skin closure and to ensure skin necrosis do not occur (Figures 2 & 3). Patients who have severe ptosis and small or large hypertrophic breasts are treated using the same new concepts in a vertical or short T-inverted scar mastopexy with small breast implant or the same new concepts of reduction mammoplasty, respectively. For secondary ptotic breasts, patients were managed by same manner. Redivac drains are placed postoperatively and removed around 1 or 2 days after surgery in each case. The type of ptotic breast, type of management and surgical result were analyzed retrospectively using medical preoperative and postoperative photographs and records. Assessment of results by the level of patient’s satisfaction was divided into poor, fair, good, and excellent. Complications were recorded each in patient.
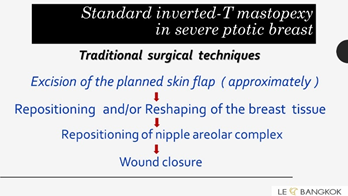
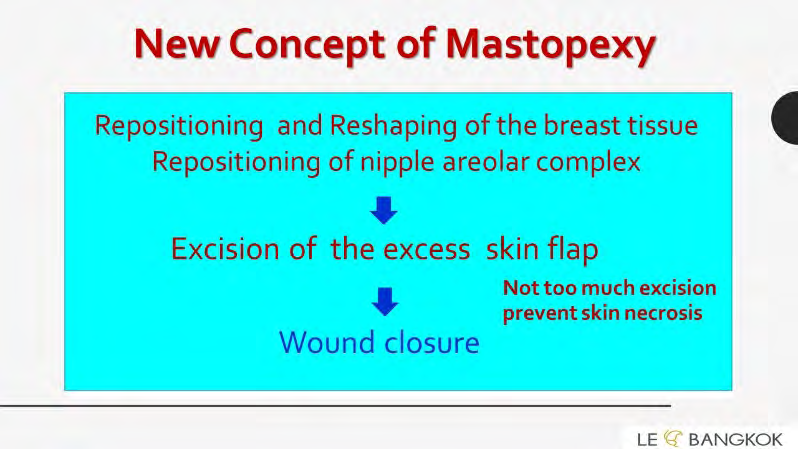
Figure 3: New concept techniques can more precise excision of skin flap because breast tissue and NAC are repositioned and reshaped before. The excess skin can excise accurately after subcutaneous tissue and breast tissues remove properly and before. Excision must be enough but not too much to prevent skin closure tightly and occur skin necrosis eventually.
Results
Of the 11 patients, of whom 9 had breast ptosis and 2 had remaining breast ptosis after previous surgery, the following surgeries were performed the short vertical scar for mastopexy and reduction mammoplasty with new concept procedure (Figures 4 and 5). Most patients had good to excellent satisfaction of the results and improved the shape of their breasts. There were two cases of major complications but they still resulted in good satisfaction. One patient, who underwent reduction mammoplasty, had superficial skin necrosis of right breast which was located at the junction of the inferior edge of areola and vertical incision. Another patient, who underwent secondary mastopexy, had superficial skin necrosis of the same area of both sides. Skin necrosis was managed by, removal of the death tissue, and redressing the wet wound every day to ensure delayed primary wound closure.



Other complications, including nipple sensations are relatively normal. Some patients have decreased sensation and this fully recovers within three months. Some patients have greater amount of bruising in cases of mastopexy or reduction mammoplasty (Table 1).
| Number of cases (total 11) | |
|---|---|
| Skin bruise | all |
| Superficial skin necrosis | 2 |
| Widening of wound | 0 |
| Hypertrophic scar | 0 |
| Temporal numbness of NAC | Fully recovery within 3 months |
Table 1: Postoperative complications.
Discussions
In cases of severe ptotic breasts, many surgical techniques of mastopexy should be chosen only if patients have normal breast volume and reduction mammoplasty is appropriate for hypertrophic breasts. For the standard surgical techniques of mastopexy in patients with severe ptotic breast, main complications are the remaining skin excess, asymmetry, not beautifully shaped breast and long scar patterns including circumvertical (including J or L scar variations), and inverted-T patterns. These complications usually occur what the causes are. Standard procedures excise the planned skin flap approximately before repositioning of the glandular tissue and nipple areolar complex. A departure from the standard techniques of the past is recommended. Step back and look carefully. If surgeons change steps of procedure that performs repositioning and reshaping of the glandular tissue and repositioning of nipple areolar complex before, we can design and excise skin flaps more accurately. Postoperative asymmetry and long undesired scar are solved. Author has yet performed the additionally reshaping procedure of glandular tissue to get beautiful lower pole of breasts too. This procedure uses atraumatic, long curved clamp to make convex shape of lower pole of breast. Mastopexy and reduction mammoplasty were performed for two patients who had only superficial skin necrosis at the areolar-vertical incision. Skin necrosis is caused by removing too much excess skin which makes the stitching too tight and is common in patients who underwent this step of surgery at the beginning of the operation or in patients who smoke excessively, this complication is discussed with patients preoperatively.
For secondary ptotic breasts, this was managed depending on the problem of each breast. Common management includes capsulotomy, partial capsulectomy and changing of the pocket of breast implant into the dual subpectoral plane I in capsular contracture, changing of the more size and /or higher profile of implant in more ptosis patients, changing of the more size and /or higher profile of implant of one side and mastopexy of another side in unequal ptotic breast, or a new mastopexy on both sides in patients with remaining severe ptosis after previous surgery [6] (Figure 6 to 7).
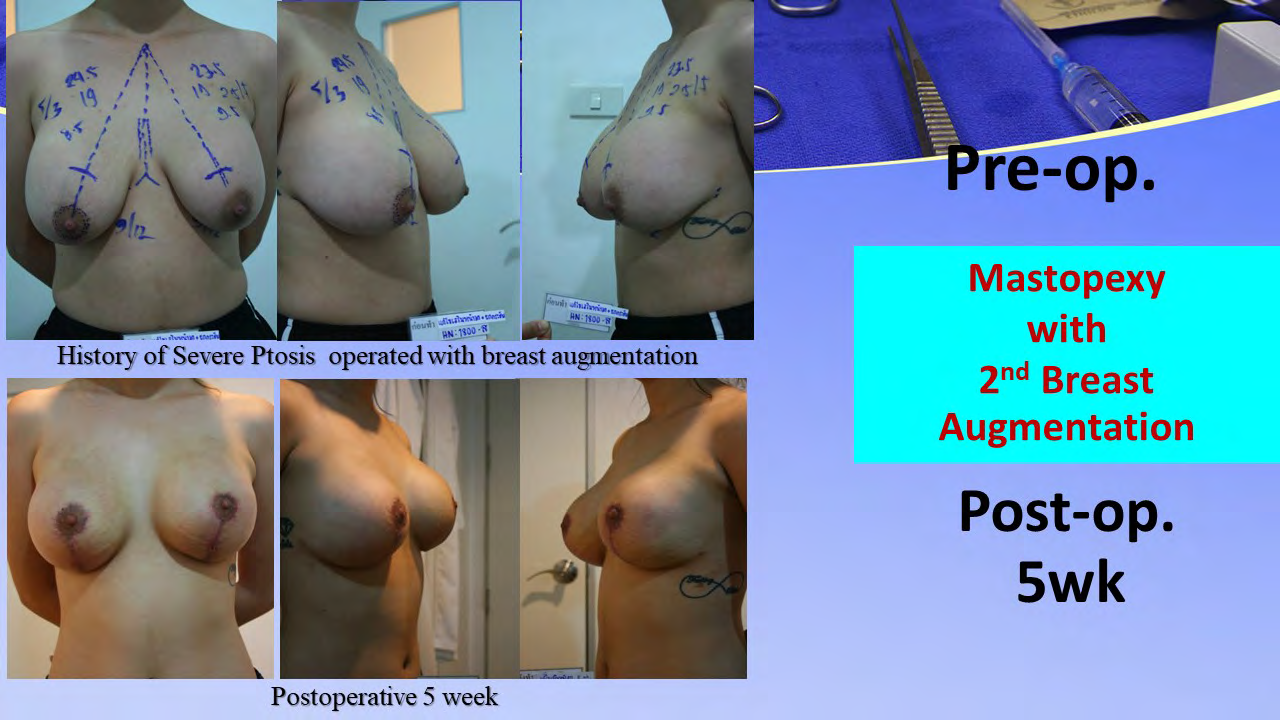

Figure 7: Case II: Patient with previous second mastopexy with breast augmentation. Her problems are multioperated, widening of periareolar and vertical scar, capsular contracture grade II and unequal breast. This case was managed by scar excision, areolar reduction, capsulotomy and partial capsulectomy, third mastopexy and breast augmentatiom. Pictures show preoperative markings, unequal breast, widening of scar both sides and two months postoperatively.
Conclusions
Degree of breast ptosis and breast tissue amount or breast volume are the key factors that determine surgical procedures. Selection of surgical procedure is important and is directly related to the results of the surgery that has been received. Cases with severe ptotic breast are managed by mastopexy with small implant for small breast volume, short vertical scar mastopexy in new concept for normal breast volume, and short vertical scar reduction mammaplasty using the new concept for hypertrophic breast. Standard mastopexy procedures excise the planned skin flap approximately before repositioning of the glandular tissue and NAC, therefore the main complications are skin excess, asymmetry, not perfectly shaped breast, long scar patterns including circumvertical (including J or L scar variations), and inverted-T patterns. Here a new concept of mastopexy was presented with excellent results. The concept consists of alterations in the steps of the procedure which performs repositioning and reshaping of the glandular tissue and repositioning of NAC followed by design and excision of the skin flaps to increase accuracy. Postoperative asymmetry and long undesired scarring are resolved with this new technique. There has yet to be an additional reshaping procedure of glandular tissue performed to obtained a beautiful convex lower pole of the breasts. J or L scars or inverted-T patterns can be decreased into short vertical scars only. Likewise, this concept can be used to reduce the common complications of reduction mammoplasty, such as postoperative asymmetry or, improper flap excision in addition to reducing the size of scarring too.
References
-
Mugea TT (2015) Breast augmentation and mastopexy. In: Mugea TT, Shiffman MA (Eds.), Aesthetic Surgery of the Breast. New York: Springer, pp: 693-721.
-
Nahabedian MY, Neligan PC (2017) Plastic surgery. 5th (Vol.), 4th (Edn.) Amsterdam: Elsevier Saunders.
-
Grotting JC, Mark AP. Mastopexy. 2nd (Edn.), In: Mathes SJ, Vincent RH(Eds.), Plastic surgery. Amsterdam: Elsevier Saunders, 5: 47-86.
-
Mugea TT (2015) Breast reduction/mastopexy with short inverted -T scar. In: Mugea TT, Shiffman MA (Eds.), Aesthetic Surgery of the breast. New York: Springer, pp: 767-796.
-
Spear SL, Newman MK (2009) Mastopexy with and without augmentation. In: Aston SJ, Steinbrech DS (Eds.), Aesthetic Plastic Surgery. Amsterdam: Elsevier Saunders, pp: 601-608.
-
Shestak KC (2006) Reoperative plastic surgery of the breast. Philadelphia: Lippincott Williams & Wilkins.
- Reconstruction of Nasal Defect Using a Local Flap Based in the Nanoperforants Concept: A Case Report
- Transplant Tourism in Japan: Insights from Nationwide Surveys and Emerging Ethical Challenges
- The Challenge of Peritoneal Vaginoplasty in Transgender Women: Review Literature and Personal Perspectives
- Algorithmic Paternalism: Autonomy Versus Automation
- Dermatoscopy in Gorlin Syndrome: Avoiding the Disfigurement in Patients
- How Artificial Intelligence is Ushering in a New Era of Innovation in General and Plastic Surgery: A Short Communication