Oncoplastic Surgery of Phyllodes Tumor of the Breast: Experience at Hermanos Ameijeiras Hospital
Introduction: Oncoplastic surgery of the breast in the treatment of Phyllodes Tumor allows wider oncological margins with better aesthetic results. Objective: To evaluate the different oncoplastic surgical techniques in the treatment of Phyllodes tumor. Method: Descriptive, longitudinal and ambispective study in 21 patients operated on for Phyllodes Tumor at the Ameijeiras Hospital from January 2006 to December 2018. Results: The average age was 49 years. There was a predominance of 42.9% of tumors with intermediate grade of malignancy, 14.3% benign and 43% malignant. The predominant tumor size was greater than 5 cm with 52.7%, followed by tumors between 2 and 5 cm with 28.6%. The surgical technique that prevailed was simple mastectomy in 57.1% and conservative surgery in 42.9%. 47.6% had free surgical margins, 33.3% undefined, 14.3% narrow, and 4.8% infiltrated. This corresponds to a Ki 67 ≤10% in 38.1% of the total. 80% underwent flap reduction mastoplasty, followed by breast implants with mastopexy of the healthy breast and Toreck technique with 9.5% each. Local recurrence occurred in only one patient 3 months after surgery, 2 years later, and then 3 years later. No complications were reported. All patients were satisfied and there were no deaths. Conclusion: Oncoplasty techniques constitute a fundamental pillar in the treatment of Phyllodes Tumor as part of multidisciplinary therapy.
Introduction
Oncoplastic breast surgery has evolved from conservative surgery by expanding its general indication in search of achieving wider tumor excision margins without compromising aesthetic results. Its objective is to carry out the surgical treatment of breast cancer without deviating from oncological principles, managing to remove a large amount of breast tissue safely and with a reduction in the number of new excisions and mastectomies [1].
Within the indications for this surgical technique are tumors of more than 20% of the breast, central, middle and lower, with resection of large regions of skin in the area of mastoplasty, axillary dissection and periareolar incisions and ptosis severe breast or other conditions where a breast reduction is considered. It is contraindicated in patients with tumors that compromise the skin, who present little breast volume, when it is not possible to ensure clean margins without mastectomy and those with mammography who present extensive malignant microcalcifications [2].
The principles on which oncoplasty is based are: obtaining wide excisions, immediate reconstruction of the breast, symmetry with the contralateral breast if necessary, and making incisions that are not very visible or noticeable. When planning an oncoplastic approach it is helpful to identify the five aesthetic components of the breast to achieve an optimal result, which are the site and extent of the tumor, size and volume of the natural breast, presence and degree of excess skin, desired location of the nipple and evaluation of the symmetry of the contralateral breast [3].
The choice of technique must also take into account the stage of the disease, the condition of the underlying muscles, and the availability of flap donor sites. Strategies for relocating mammary structures include glandular tissue rotation techniques and the use of muscle flaps [4].
Phyllodes Tumor (PT) is a rare fibroepithelial neoplasm, representing 0.3 to 1% of all breast tumors. It was first described in 1774 as a giant type of fibroadenoma and was named as cystosarcoma phyllodes by Muller in 1838. They are benign in most cases and malignant one’s account for 10 to 15% of cases. The benign ones are fast growing and reach a large size, they do not metastasize, but they are locally aggressive with a greater tendency to recur. Malignant ones spread hematogenously. It is usually diagnosed in women in the fifth decade of life. Its etiology has not yet been fully described, but it is believed that hyperestrogenism and breast trauma play a fundamental role in its development. They are usually identified as a well-defined, firm, mobile and painless breast lump or mass [5, 6, 7].
Surgery is the treatment of choice for these tumors. According to the National Comprehensive Cancer Network (NCCN), surgical treatment for these malignant tumors is complete excision with 1-cm margins without standard axillary lymph node dissection. This is due to the fact that the metastatic dissemination of these tumors is by hematogenous and not lymphatic route, so they have a low incidence of lymph node metastases. Currently, oncological surgical strategies are reduced to prophylactic diagnostic surgery, conservative surgery, mastectomy and oncoplastic surgery. The latter is only applicable in patients with this neoplasm [8].
The importance in this type of tumor is to approach from the beginning an analysis of the conduct to follow with a multidisciplinary team made up of mastologists, oncologists and plastic surgeons. Depending on the size of the resulting bloody area after tumor removal, the depth of the resection with or without exposure of noble structures, as well as the indication for adjuvant therapy, the choice of reconstructive technique will be chosen. These are divided into two large groups: with autologous tissues or with alloplastic materials. The ideal and safest thing is to guarantee closure with local flaps that provide similar characteristics of the external coverage in the mammary region. In most articles they refer to the use of the latissimus dorsi musculocutaneous flap. However, sometimes the placement of implants is enough to rescue breast harmony and symmetry. This study is presented with the objective of evaluating the different oncoplastic surgical techniques in the treatment of Phyllodes Tumor.
Method
Descriptive, longitudinal and ambispective study in women with a history of Phyllodes Tumor who were treated in a multidisciplinary breast pathology consultation at “Hermanos Ameijeiras” Hospital for tumor excision and concomitant oncoplasty in the period between January 2006 and December 2018. Patients older than 19 years were included, whose frozen or paraffin biopsy results reported Phyllodes Tumor, complementary within normality, who agreed to participate in the research, with prior written informed consent and without psychiatric history. Patients with chronic decompensated diseases, with dermatological lesions or scars in the skin of the flap donor area, smokers, alcoholics, drug addicts, with previous radiotherapy treatment, in treatment with drugs that compromise healing or coagulation and operated on other conditions were excluded, institutions that attended with local recurrence. The exit criteria were those patients who, after starting the study, did not wish to continue and who did not attend the scheduled consultations. The sample was made up of 21 patients who were selected intentionally.
Operationalization of Variables
• Age: According to chronological age up to the time of the study.
- Histological diagnosis - Benign - Intermediate - Malignant - Low grade malignant - Malignant of intermediate degree - Bilateral high-grade malignant
- Tumor size - Tumor greater than 2 cm and less than 5 cm - Tumor greater than 5 cm - Unknown
- Type of operation - Conservative Surgery: Exeresis of the tumor with tumor-free surgical section edges (between 0.5 and 1 cm) and part of the breast is preserved. It includes several options such as: wide exeresis, lumpectomy, quadrantectomy and partial mastectomy. - Mastectomy: complete removal of the tumor and the mammary gland with tumor-free surgical section edges (between 0.5 and 1 cm). The technical variants were: Simple Mastectomy (Sanitary or Total) when only the resection of the mammary gland is performed and Modified Radical Mastectomy when axillary lymph node dissection of Berg levels I, II and III is added.
- Surgical section borders - Free - Infiltrators - Narrow - Not specified
- Oncoplasty techniques used - Reductive flap mammoplasty: Excision of excess breast tissue through the use of flaps nourished by one or two main artery pedicles, with repositioning of the Nipple-Areola Complex (NAC) and adaptation of the skin to the new breast shape. This technique can be monopedunculated or bipedunculated according to the amount of breast parenchyma to be resected [2, 3]. - Reduction mastoplasty with breast implants and mastopexy of the healthy breast using the Thorek technique: Excision of excess breast parenchyma with a monopedicle or bipedicle technique plus placement of a retromuscular breast implant, associated with symmetrization of the contralateral breast with a mastopexy technique with a free graft of the NAC on which is covered with a Brown dressing for five days, with subsequent discovery for its survival evaluation [4, 3]. - Rotation of the thoracoabdominal dermal-fat flap: Technique by which fatty tissue is removed to cover defects secondary to tumor exeresis. The adipose tissue, as well as the dermis supplied from the upper abdomen, gives greater thickness to the lower quadrants of the breast, resulting in an aesthetically acceptable scar [2]. - Autologous oncoplasty with adipose tissue graft: It consists of obtaining adipose tissue from the donor area, which can be the periumbilical region by means of liposuction with a blunt-ended cannula, and grafting it at the level of the mammary region in order to give volume. and screening using patients’ own tissue [7].
- Ki 679 - Negative - Less than or equal to 10% - Greater than 10% - Not assessable
- Presence of recurrence - Yes - Not
- Complications - Yes - Not
- Satisfaction - Yes - Not
- Survival - Yes - Not
Techniques and Procedures
Preoperative
Surgical Technique
Excision of the tumor with tumor-free surgical section margins (between 0.5 and 1 cm) and part of the breast is preserved. It includes several options such as: wide exeresis, lumpectomy, quadrantectomy and partial mastectomy.
Complete exeresis of the tumor and the mammary gland with tumor-free surgical section margins (between 0.5 and 1 cm). The technical variants were: Simple Mastectomy (Sanitary or Total) when only the resection of the mammary gland is performed and Modified Radical Mastectomy when axillary lymph node dissection of Berg levels I, II and III is added.
The cornerstone of surgical treatment of PT of the breast consists of oncoplastic surgery, which consists of the aesthetic restoration of the breast as a complement to conservative surgery, post-mastectomy and for the closure of large defects after oncological resections.
In cases where muscle and sufficient breast volume were preserved with skin coverage, cohesive silicone gel implants were placed and symmetrized with contralateral mastopexy. In very large tumors and gigantomastia, oncoplasty was performed with a free graft of the NAC. In the rest, the tumor was removed according to the breast reduction pattern using pedunculated flaps.
Posoperative Care
Dry healing at 24 hours to assess the vitality of the flaps and coping with the wounds. In cases where the use of drains was necessary, this was removed when the count was less than 50cc. Hospital discharge and weekly outpatient follow-up up to one month and quarterly up to one year with photographic record. Withdrawal of points between 15 and 21 days.
The sources for obtaining the information were the interview, physical examination, clinical history, report and operative announcement of each patient. A data collection form was used in which the variables of interest were recorded. The patients were chosen by consecutive attendance at the surgery consultation. The patients were informed of the details of the investigation, voluntariness, the right to withdraw whenever they wished, and informed consent was signed.
The information obtained was transferred to a database using the Excel Microsoft Office version XP application, which was subsequently exported to the Statistical Package for Social Sciences (SPSS) version 23.0 system for analysis. The statistical program Epidat 3.1 was used to estimate the measures of the effect of the treatment under study.
Qualitative variables were summarized in absolute numbers and percentages. Quantitative variables in mean and standard deviation.
The results were compared with the existing national and international literature. The findings were discussed based on the stated objectives. Finally, the coincidences and contradictions in relation to the proposed research and other related studies were verified, which allowed reaching the conclusions of the study.
The research was carried out from an ethical point of view in accordance with the provisions of the 64th General Assembly of the Declaration of Helsinki [10].
Results
Patients in the age group between 40 and 50 years prevailed with 90.4%, and the average age was 49 years. 42.9% of the tumors were in the intermediate range of malignancy, 14.3% were benign and 43% malignant (Table 1).
| Histological Diagnosis | No. | % |
|---|---|---|
| Benign | 3 | 14,3 |
| Intermediate | 9 | 42,9 |
| Malignant | 1 | 4,8 |
| Low grade malignant | 6 | 28,6 |
| Malignant of intermediate degree | 1 | 4,8 |
| Bilateral hight-grade malignant | 1 | 4,8 |
Table 1: Range of malignancy, 14.3% was benign and 43% malignant.
Regarding the histological characteristics, tumors larger than 5 cm predominated in 52.7% (Figure 1), followed by tumors larger than 2 cm and up to 5 cm with 28.6% and the tumor size was unknown in 19%.

The surgical technique for tumor removal that prevailed was simple mastectomy in 57.1% while conservative surgery represented 42.9% (Figure 2).
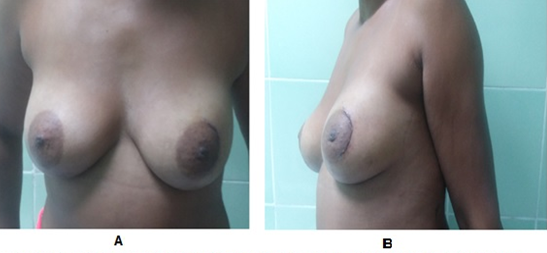
The 47.6% of the sample presented free surgical section edges, 33.3% unspecified, 14.3% narrow, and 4.8% infiltrates were found, which led to a reoperation of a patient who she had undergone conservative surgery and the mastectomy was completed. This corresponds to a Ki 67 less than or equal to 10% in 38.1% of the total. Regarding oncoplasty, 80% of the patients underwent flap reduction mastoplasty, followed by breast implants with mastopexy of the healthy breast and Thorek’s technique with 9.5% each (Figures 3 & 4).

Local recurrence occurred in a single patient with an intermediate grade of malignancy, a tumor size of 9 cm that infiltrated the pectoralis major muscle, tumor-free surgical section edges, and Ki 67 > 20%. Surgical treatment was Modified Radical Mastectomy, but despite applying the appropriate technique, the patient presented local recurrence 3 months after surgery, 2 years later, and then 3 years later. For this reason, he had 3 reinterventions, each time more aggressive. In the first reintervention, a wide excision was performed, in the second-wide excision with oncoplasty with rotation of a thoraco-dorsal dermo-fat flap and in the last wide excision plus autologous oncoplasty with a free graft to close the defect.
No complications occurred in any of the patients. 100% of the patients were satisfied and overall survival.

Discussion
Oncoplastic surgery refers to the treatment of breast cancer. PT, although it can present in a malignant variant, is par excellence a benign tumor that requires aggressive surgical conduct that involves the use of the same oncoplastic techniques. In the study published by Hasdemir, et al. [12] in 2020 they report an average age of 39.8 years. Alkushi, et al. [13] in 2021 report a mean age of 42 years. The present study agrees with the stated results, which may be related to the fact that estrogen levels decrease during the menopausal period, increasing the possibilities of changes in the breast tissue.
Alkushi, et al. [13] carried out a retrospective cohort study in 46 patients diagnosed with this pathology, classifying 58.6% of the resected tumors as benign, 23.9% as intermediate, and 17.4% as malignant. Of them, 86.7% received conservative surgery and 13.3% mastectomy. In the present investigation, unlike what was published by Alkushi, tumors classified with an intermediate degree of malignancy predominated and simple mastectomies were performed the most. This may be related to the fact that the indicated surgery is related to the degree of malignancy, therefore, if benign tumors predominate, conservative surgery is the best option, while if the risk of malignancy predominates, the ideal is mastectomy to avoid recurrence.
Miyoshi, et al. [14] in 2020 carried out a study in 44 patients, where the average tumor diameter was 39.2 mm with a positive margin in 13.6%. In the present study, more than half of the sample presented sizes greater than the Miyoshi study, followed by the range between 2-5 cm with a minority without size definition. In agreement, most of the patients were free of tumor, with a low percentage with positive borders.
Ki 67 is used as a cell proliferation marker in breast cancer. In a study conducted in 2020 by Zhu [15] in 1,800 patients with breast tumors, 62.5% reported a Ki 67 > 30% associated with a worse prognosis for survival overall and disease-free survival, mainly in tumors less than or equal to 2 cm. Results with which the present investigation does not agree, which may be related to the fact that most PTs are benign with larger sizes.
There are multiple denominations that have been given to oncoplasty techniques, some based on the pedicle and others on the type of closure. Savioli, et al. [16] in 2021 conducted a study on 50 patients operated on with oncoplastic procedures where 78% underwent volume displacement reduction mastoplasty, Benelli-type reduction in 4%, and tennis racket mastoplasty, slice of melon, wing bat and fish tail at 2% each. They also performed immediate contralateral symmetrization in 48% of the sample and oncoplastic conservation of volume replacement in 10%. In the present investigation, the techniques were named after the flap that preserved the NAC, which were mostly monopedunculated, leaving the NAC graft for those patients in whom the extreme resection of the tumor with a safety margin could constitute a risk of necrosis of the same.
The PT, although mostly benign, have a risk of recurrence. In an article developed in 2019 by Ditsatham, et al. [17] in 181 patients, 9 were diagnosed with recurrence, five benign with local recurrence, one intermediate, and three malignant, of which one developed pulmonary metastasis. In the present study there were no cases of local or distant recurrences.
As stated by Canturk, et al. [18] in 2021 there is no difference in surgical complications when comparing oncoplastic surgery with breast-conserving surgery when the key points referred to in their article are met, such as performing the surgical procedure without deviating from oncological principles. and the use of the oncoplastic technique according to the established level. A study carried out in 2015 [19] in 113 in whom breast implants and expanders were used as oncoplasty techniques, asymmetry predominated as a complication in 89%, poor healing in 43% of cases, capsular contracture in 45% of implants and late exposures at 4%. Singh [20] in 2018 reported surgical site infection in 15 patients, marginal skin necrosis in two patients and superficial necrosis in one. Shankhdhar [21] in 2021 reported partial skin necrosis, suture line dehiscence, surgical wound infection, seroma, and fat necrosis. None of these complications were reported in the present study.
In Plastic and Reconstructive Surgery, satisfaction and good final aesthetic results are the essential part of every surgical procedure. In these patients it becomes more important because they feel mutilated after the surgical procedure of tumor removal with great affectation of self- esteem and quality of life. In the present study, the entire sample was satisfied with the results obtained after breast reconstruction, in agreement with the results of Zhang, et al. [22] in 2021 and Walker, et al. [23] in the same year.
Oncoplasty techniques constitute a useful practical element in the treatment of Phyllodes Tumor which, although rare, requires oncoplastic therapy when it occurs.
References
-
Panda N, Haynes AB (2020) Prioritizing the Patient Perspective in Oncologic Surgery. Ann Surg Oncol 27(1): 43-44.
-
Weber WP, Morrow M, Boniface J, Pusic A, Montagna G, et al. (2020) Knowledge gaps in oncoplastic breast surgery. Lancet Oncol 21(8): e375-e385.
-
Chu CK, Hanson SE, Hwang RF, Wu LC (2021) Oncoplastic partial breast reconstruction: concepts and techniques. Gland Surg 10(1): 398-410.
-
Gilmour A, Cutress R, Gandhi A, Harcourt D, Little K, et al. (2021) Oncoplastic breast surgery: A guide to good practice. Eur J Surg Oncol 47(9): 2272-2285.
-
Fede ABS, Pereira Souza R, Doi M, De Brot M, Osorio CABT, et al. (2021) Malignant Phyllodes Tumor of the Breast: A Practice Review. Clin Pract 11(2): 205-215.
-
Pascarella S, Maher Z, Goldbach A, Hava S, Choksi R, et al. (2020) Giant phyllodes tumor of the breast. Breast J 26(3): 550-552.
-
Rayzah M (2020) Phyllodes Tumors of the Breast: A Literature Review. Cureus 12(9): e10288.
-
Lissidini G, Mulè A, Santoro A, Papa G, Nicosia L, et al. (2022) Malignant phyllodes tumor of the breast: a systematic review. Pathologica.
-
Davey MG, Hynes SO, Kerin MJ, Miller N, Lowery AJ (2021) Ki-67 as a Prognostic Biomarker in Invasive Breast Cancer. Cancers (Basel) 13(17): 4455.
-
Viglino D, Collomb Muret R, Mabiala Makele P, Clape C, Gros R, et al. (2020) Adequacy of oral information given to research participants regarding the Declaration of Helsinki. Eur J Emerg Med 27(1): 65-66.
-
Gort N, van Gaal BGI, Tielemans HJP, Ulrich DJO, Hummelink S (2021) Positive effects of the enhanced recovery after surgery (ERAS) protocol in DIEP flap breast reconstruction. Breast 60: 53-57.
-
Hasdemir S, Tolunay S, Özşen M, Gökgöz MŞ (2019) Phyllodes Tumor of the Breast: A Clinicopathological Evaluation of 55 Cases. Eur J Breast Health 16(1): 32-38.
-
Alkushi A, Arabi H, Al Riyees L, Aldakheel AM, Al Zarah R, et al. (2021) Phyllodes tumor of the breast clinical experience and outcomes: A retrospective cohort tertiary hospital experience. Ann Diagn Pathol 51: 151702.
-
Miyoshi T, Wakatsuki K, Shiobara M, Suda K, Miyazawa K, et al. (2020) Study of Phyllodes Tumor of the Breast in 44 Cases of Resection. Gan To Kagaku Ryoho 47(13): 1972-1973.
-
Zhu X, Chen L, Huang B, Wang Y, Ji L, et al. (2020) The prognostic and predictive potential of Ki-67 in triple- negative breast cancer. Sci Rep 10(1): 225.
-
Savioli F, Seth S, Morrow E, Doughty J, Stallard S, et al. (2021) Extreme Oncoplasty: Breast Conservation in Patients with Large, Multifocal, and Multicentric Breast Cancer. Breast Cancer (Dove Med Press) 13: 353-359.
-
Ditsatham C, Chongruksut W (2019) Phyllodes tumor of the breast: diagnosis, management and outcome during a 10-year experience. Cancer Manag Res 11: 7805-7811.
-
Cantürk NZ, Şimşek T, Özkan Gürdal S (2021) Oncoplastic Breast-Conserving Surgery According to Tumor Location. Eur J Breast Health 17(3): 220-233.
-
Micolo T (2015) Breast reconstruction: review of 1,713 reconstructions in 45 years of personal experience. Plastic surgery 25(3): 177-191.
-
Singh G, Kohli PS, Bagaria D (2018) Lateral Oncoplastic Breast Surgery (LOBS) - A new surgical technique and short term results. Am J Surg 216(6): 1166-1170.
-
Shankhdhar VK, Jaiswal D, Bhansali C, Despande R, Yadav PS, et al. (2021) Reduction Mammoplasty Approach to Oncoplasty-Zone-Wise Planning in Indian Patients. Indian J Plast Surg 54(3): 264-271.
-
Zhang X, Cai L, Yin B, Han X, Li F (2021) Total breast reconstruction using large-volume condensed and viable fat grafting after mastectomy. J Plast Reconstr Aesthet Surg 74(5): 966-973.
-
Walker NJ, Park JG, Maus JC, Motamedi V, Rebowe RE, et al. (2021) Prepectoral Versus Subpectoral Breast Reconstruction in High-Body Mass Index Patients. Ann Plast Surg 87(2): 136-143.
- Reconstruction of Nasal Defect Using a Local Flap Based in the Nanoperforants Concept: A Case Report
- Transplant Tourism in Japan: Insights from Nationwide Surveys and Emerging Ethical Challenges
- The Challenge of Peritoneal Vaginoplasty in Transgender Women: Review Literature and Personal Perspectives
- Algorithmic Paternalism: Autonomy Versus Automation
- Dermatoscopy in Gorlin Syndrome: Avoiding the Disfigurement in Patients
- How Artificial Intelligence is Ushering in a New Era of Innovation in General and Plastic Surgery: A Short Communication