Total Palate Reconstruction with Unilateral Angular Artery-Based Nasolabial Flap
Introduction: Pleomorphic adenoma is a mixed tumor consisting of differentiation of epithelial and mesenchymal cells. They are the most common benign tumors encountered at the salivary glands. Several flap options have been described for the reconstruction of palate. Case Report: A 48-year-old male patient was admitted to our outpatient clinic with a complaint of a mass at the palate. The mass was extending from the oral cavity to the nasal cavity. Hemi-maxillectomy was applied and the reconstruction was achieved using a reverse flow unilateral angular artery-based fasciocutaneous flap. Conclusion: Pleomorphic adenoma should be kept in mind when evaluating the lesions of hard palate. Angular artery-based fasciocutaneous flap is a reliable method for hard palate reconstruction.
Introduction
While salivary gland tumors constitute 1-4% of all neoplasms in humans, they constitute less than 7% of all tumors occurring in the head and neck region [1]. Pleomorphic adenoma is a mixed tumor consisting of differentiation of epithelial and mesenchymal cells. They are the most common benign tumors encountered at the salivary glands. The tumor is mostly seen at the parotid gland (75%)-usually in the superficial lobe, submandibular gland (5-10%) and minor salivary glands. Among the minor salivary glands, it is most commonly located on the hard palate. Rarely, they can be seen in ectopic localizations within extra-oral areas [2].
Pleomorphic adenoma (PA) is characterized by a painless, mobile and slowly growing mass. Despite its slow growth, it can reach large sizes. Treatment of the tumor constitute of a wide surgical excision.
Inadequate resection may cause recurrence of the lesion. Although the tumor is benign, it may show metastasis and malignant transformation [3]. Although the lesion can be seen in a wide age range, it is most commonly seen in the 5th and 6th decades. PA is more common in women than in men [4]. Here, we present a case with a massive invasive PA treated with a unilateral angular artery-based nasolabial flap.
Case Report
A 48-year-old male, diabetic patient was admitted to our outpatient clinic with a complaint of a mass at the palate. The patient stated that the mass started to appear about 28 years ago. The physical examination revealed a 3x2 cm hard mass with ulcerated components at the mucosa of the hard palate (Figure 1).

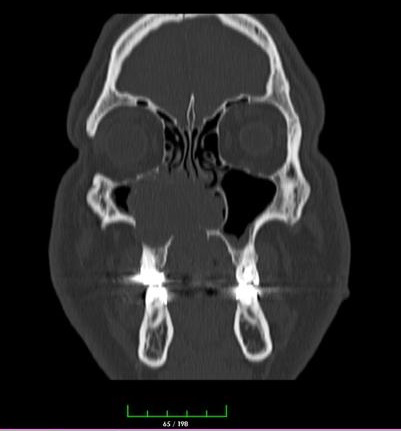
The mass led to nasal obstruction and hypo-nasality signs. The patient also mentioned that he is experiencing pain at the right cheek for the last two months. The patient’s history was unremarkable for previous surgery, trauma, surgery or smoking. No lymphadenopathy was detected. The MRI report revealed a heterogeneous mass of approximately 3x2 cm at the base of the right nasal cavity and the right maxillary sinus, with a component of approximately 2x1.5 cm extending towards the oral cavity causing erosive change in the palate (Figure 2).
The patient was operated under general anesthesia. The skin flaps were elevated through a right lateral rhinotomy incision. This incision was combined with a right gingivobuccal incision. Hemi-maxillectomy was applied with the help of powered-saw. The right nasal turbinates, nasal mucosa and septum were excised due to tumoral invasion. The component in the palate was exposed with the help of Dingman retractor and the tumoral mass was excised from the surrounding soft tissues and alveolar bone. The reconstruction operation was planned to be after the pathology report.
The pathology report of the mass revealed a “pleomorphic adenoma” and all surgical borders were tumor-free. For the reconstruction of the defect we designed a reverse angular artery-based fasciocutaneous flap from the left nasolabial region (Figure 3).

The flap was elevated over the muscles with a size of 9x4 cm. The flap then was tunneled under the lip and inserted to the oral cavity to cover the palate. The flap’s donor area was closed using a poster auricular fasciocutaneous flap. No complications were encountered during or after the operation (Figure 4).

Discussion
Pleomorphic adenoma appears as a slowly growing, asymptomatic, unilateral hard mass. The smaller the affected salivary gland, the higher the chance of it turning into a malignant tumor. The treatment method includes a wide surgical resection in order to eradicate the possibility of malignant transformation and to reduce the risk of recurrence [5]. With advanced imaging methods such as CT and MRI, the operation is planned by revealing the location and size of the tumor and its relationship with the surrounding structures. The most common surgical complications are capsular penetration and tumor rupture.
If these complications develop during surgery or if wide excision cannot be achieved, recurrence may be observed as multiple, nodular masses in the salivary gland or surrounding tissues a few years after the first operation [6]. The pleomorphic adenoma in this case was excised together with the affected bone segment of the maxilla, and reconstruction was applied after the pathology report.
Although free flaps are the first choice for large defects in the palate, other pedicled flaps can be used in the presence of small-medium sized defects and in the presence of additional comorbidities. These include pedicled extraoral locoregional flaps such as the submental flap, facial artery musculo mucosal (FAMM) flap, or the more recently described deep lingual artery axial flap [7].
In addition, facial and angular artery-based pedicle flaps are preferable options for the repair of midface defects due to minimal donor site morbidity and reliable vascular circulation. The results obtained using facial artery perforator flaps in the repair of midface defects may be at least as good as those obtained from local flaps [8].
They provide greater design freedom and can be easily rotated ≥180° to close the defect. In addition, they are very functional flaps with many advantages. For example, if there is an intact cutaneous area between the defect and the donor area, they can be easily transferred to the defect site via a subcutaneous tunnel without leaving any deformity [9, 10].
The presence of diabetes in our patient prompted us to consider pedicled flaps. Based on the size and localization of the defect we considered a contralateral reverse angular artery-based flap. The designed flap was elevated as a fasciocutaneous flap without including the muscles. The flap was tunneled under the intact skin of the left part of the upper lip and palate reconstruction was achieved.
Conclusion
Even the pleomorphic adenoma is a benign tumor, it should be widely excised because of its recurrence and malignant transformation risks. As a result, the localization of the minor salivary glands should be well known and the lesions occurring in these areas should be carefully evaluated in terms of tumoral formations. Although many flaps have been described for the reconstruction of intraoral defects, the use of a reverse flow angular artery-based fasciocutaneous flap for palate reconstruction is a reliable alternative.
References
-
Rivera-Bastidas H, Ocanto RA, Acevedo AM (1996) Intraoral minor salivary gland tumors: a retrospective study of 62 cases in a Venezuelan population. J Oral Pathol Med 25(1): 1-4.
-
Brookstone MS, Huvos AG (1992) Central salivary gland tumors of the maxilla and mandible: a clinicopathologic study of 11 cases with an analysis of the literature. J Oral Maxillofac Surg 50(3): 229-236.
-
Rahnama M, Orzędała-Koszel U, Czupkałło L (2013) Pleomorphic adenoma of the palate: a case report and review of the literature. Contemp Oncol (Pozn) 17(1): 103-106.
-
Li W, Lu H, Zhang H (2019) Sinonasal/nasopharyngeal pleomorphic adenoma and carcinoma ex pleomorphic adenoma: a report of 17 surgical cases combined with a literature review. Cancer Manag Res 11: 5545-5555.
-
Pons Vicente O, Almendros Marqués N, Berini Aytés L (2008) Minor salivary gland tumors: A clinicopathological study of 18 cases. Med Oral Patol Oral Cir Bucal 13(9): 582-588.
-
Manucha V, Ioffe OB (2008) Metastasizing pleomorphic adenoma of the salivary gland. Arch Pathol Lab Med 132(9): 1445-1447.
-
Britt CJ, Hwang MS, Day AT (2019) A Review of and Algorithmic Approach to Soft Palate Reconstruction. JAMA Facial Plast Surg 21(4): 332-339.
-
Schultz JJ, Viviano SL, Ayyala HS, Lee BB (2021) Superficial temporal artery perforator flaps for reconstruction of intraoral defects. Microsurgery 41(2): 119-123.
-
Horta R, Barreiro D (2019) The Facial Artery Perforator Flap as a New Option for Reconstruction of Intraoral Defects: Surgical Tips and Clinical Series. J Craniofac Surg 30(5): 1525-1528.
-
Du YF, Zhou WN, Li J, Jiang HB (2014) A new design of facial artery perforator flaps for the reconstruction of small- to medium-sized intraoral defects. J Craniofac Surg 25(6): 2098-2100.
- Reconstruction of Nasal Defect Using a Local Flap Based in the Nanoperforants Concept: A Case Report
- Transplant Tourism in Japan: Insights from Nationwide Surveys and Emerging Ethical Challenges
- The Challenge of Peritoneal Vaginoplasty in Transgender Women: Review Literature and Personal Perspectives
- Algorithmic Paternalism: Autonomy Versus Automation
- Dermatoscopy in Gorlin Syndrome: Avoiding the Disfigurement in Patients
- How Artificial Intelligence is Ushering in a New Era of Innovation in General and Plastic Surgery: A Short Communication