Thigh Cellulite Treatment Using Laser-Assisted Liposuction: A Consecutive Descriptive Case Series
Cellulite is a highly prevalent condition affecting up to 90% of post pubertal females. The most common reasons patients seek cellulite treatment include emotional, psychological, and practical motivations. Laser-assisted liposuction is a minimally invasive procedure able to produce skin and subcutaneous changes. This research was elaborated as a prospective longitudinal study, aiming to estimate the repercussions of laser-assisted liposuction on thigh cellulite aspects and distribution. Consecutive outpatients with preoperative thigh cellulite submitted to laser-assisted liposuction, using the Lipo One Step HD device, were recruited from the senior author's private practice. Preoperative and 3 months following surgery pictures were obtained. These photographs were assessed by two independent plastic surgeons to evaluate thigh cellulite appearance before and after surgery using the Clinician Reported Photonumeric Cellulite Scale (CR-PCS). Twelve patients entered the study. All patients were female and white. The mean age was 42.5 years (SD ± 9.3), and the mean Body Mass Index was 26.7 kg/m2 (SD ± 2.1). The mean CR-PCS preoperative was 3.75, and 3 months following laser-assisted liposuction was 2.53 (p=0.02). We have obtained comprehensive results demonstrating the role of laser-assisted liposuction on thigh cellulite. In addition, the evidence from our research suggests that laser-assisted liposuction reduces thigh cellulite.
Introduction
Cellulite is a term used to describe one of the most investigated cosmetic concerns, affecting up to 90% of post pubertal females [1]. Also called gynoid lipodystrophy, cellulite is a characteristic topography alteration with dimpled and knotty skin, which occurs mainly in body areas with more significant fat deposits, such as thighs and buttocks [2]. Cellulite pathophysiology is not yet defined. Several theories aim to explain the origin of the alteration. However, to date, authors consider it multifactorial, and there are indications that endothelial dysfunction and microcirculatory disorders are essential factors for developing this phenomenon [3]. Overall, cellulite depressions are directly associated with a significant increase in subcutaneous fibrous septae, tethered to the underside of the dermis by fat accumulation [4]. These septa lead to adipose tissue lobulation, determining the structure of the skin surface, especially in females, since it is a connection to the skin-fascia interface is perpendicular, as opposed to what occurs in the male population [5]. Although not life-threatening, cellulite is a cosmetical dysfunction [6]. The most common reasons patients seek cellulite treatment include emotional, psychological, and practical motivations [Maisel, 2018]. Nevertheless, the alteration is also considered a predisposition for systemic diseases, as it is a dysfunction that affects lipid hypodermal tissue – which has a complex endocrine activity [3].
Historically, there have been efforts in search of treatment for this highly prevalent skin alteration; liposuction is an alternative for this pathology. Other options beyond traditional suction-assisted lipoplasty include ultrasound- assisted liposuction, power-assisted liposuction, and laser lipolysis, also known as laser-assisted liposuction [7].
Laser-assisted liposuction is considered to be a minimally invasive procedure. A flexible optical fiber is inserted into the hypodermis by a small-caliber cannula. It acts by thermal and thermomechanical effects: the adipocytes absorb the energy and rupture. Furthermore, the cannula is moved back and forth in the fat tissue, effectively rupturing the subcutaneous fibrous septae. Therefore, this procedure leads to a fat volume reduction and remodeling of the collagenous tissue, with clinically evident skin retraction. It may also increase collagen and elastin fibers, tightening the skin [8]. Traditional liposuction leads to a more extended recovery; however, laser-assisted liposuction decreases operation effort and bleeding and smoothes the skin more evenly. Hence, to better comprehend the treatment mentioned above on specific body fat deposits, this paper is a preliminary attempt to study the effect of laser-assisted liposuction on thigh cellulite.
Patients and Methods
Study Design
This manuscript was elaborated as a prospective longitudinal study, aiming to estimate the repercussions of laser-assisted liposuction on thigh cellulite aspects and distribution. The Strengthening Reporting of Observational Studies in Epidemiology script for observational studies was followed during the manuscript elaboration. The Helsinki Declaration principles were followed in this research.
Participants
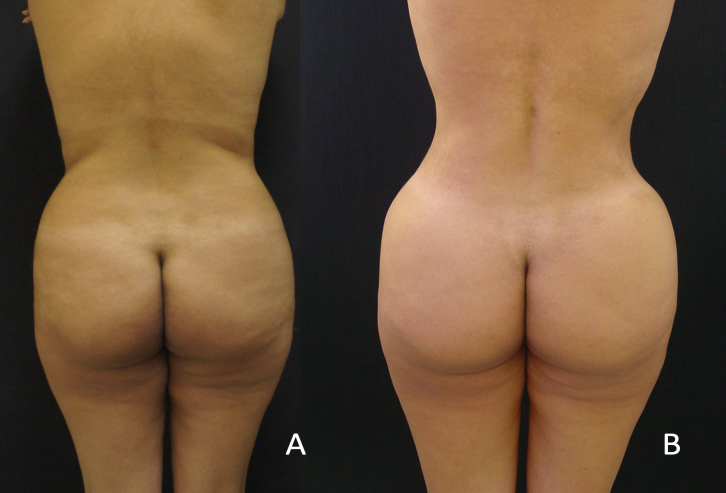
Consecutive outpatients with preoperative thigh cellulite submitted to laser-assisted liposuction were recruited from the senior author private practice, between January 2022 and October 2022. Written informed consent was obtained using a printed form. Preoperative and 3 months following surgery pictures were obtained. These photographs were assessed by two independent plastic surgeons to evaluate thigh cellulite appearance before and after surgery using the Clinician Reported Photonumeric Cellulite Scale (CR-PCS) [9]. This scale utilizes photographs to rate cellulite severity as a single item on a 5-point scale, ranging from none (0) to severe (4).
Surgical Technique
Patients were submitted to laser-assisted liposuction using the Lipo One Step HD device (DMC Equipment, São Paulo, Brazil). This device consists of an infrared 1210-nm wavelength laser diode [10]. Patients underwent a single treatment procedure in the bilateral thighs under epidural anesthesia. The skin was prepared with a chlorhexidine antiseptic with patients lying prone on the surgical table. One 1 cm incision was made on each gluteal crease. Using the dry technique, a 2 mm cannula front-firing fiber tip was passed through the incision, delivering energy to the subcutaneous layer. The cannula fiber was then caudally passed fan-shaped to subcise the septae and melt the excess fat. Each patient has worn a compression garment for the first two weeks post treatment. Lymphatic drainage was indicated two times a week for the first two months.
Data Analysis
The raw data were exported to the SPSS v.22 statistical package (IBM, New York, USA). The results of continuous quantitative variables were expressed as mean ± standard deviation. Paired t-test was performed to identify the differences between the CR-PCS values preoperatively and 3 months after the procedure. Values of p<0.05 were considered significant.
Results
Twelve patients entered the study. All patients were female and white. The mean age was 42.5 years (SD ± 9.3), and the mean Body Mass Index was 26.7 kg/m2 (SD ± 2.1). The mean CR-PCS preoperative was 3.75, and 3 months following laser-assisted liposuction was 2.53 (p=0.02).

Discussion
Cellulite (gynoid lipodystrophy) is prevalent worldwide, affecting 80% to 98% of women of all races after puberty [11]. Despite its high prevalence, it remains a major cosmetic concern for women. They are characterized by skin surface alterations with depressions and elevations that make the orange skin effect, mainly on the buttocks and thigh areas. Cellulite’s physiopathology is a multifactorial pathology of unknown etiology; studies confirmed that depressions on cellulite occur by increased fibrous septa on the subcutaneous tissue [2]. Local alterations in lymphatic and vascular microcirculation of subcutaneous tissue can be responsible for it, with increased capillary permeability and deposition of glycosaminoglycan on capillaries walls, resulting in vascular edema, congestion, and local hypoxia. At this time glycosaminoglycan stimulates neovascularization and inflammatory events that stimulate fibrous septae development [6]. Factors like the polymorphism on subcutaneous genes were associated with cellulite because the gene (ACE rs1799752) assists model ACE activity and tissue oxygenation, and the gene (HIF1A rs11549465) has an anti-fibroinflammatory function and a protective role against tissue micro-hipoxyas [12]. On addiction to it, low adiponectin levels, a hormone produced by adipocytes that have anti-inflammatory, antifibrotic and vasodilatory effects, can be associated with the pathogenesis of cellulite [13].
Bennardo, et al. demonstrated in a prospective study with 26 female patients with a mean age of 38 years old, that radiofrequency treatment improved the total mean Cellulite Severity Scale on 6,2 points after three months, the total mean on the end of the study was 4.5 [5]. In our study with 12 female patients, the mean age was 42.5 years, demonstrating the total mean CR-PCSS preoperative was 3.75, and three months after Laser-assisted Liposuction, the CR-PCSS was
2,53 (p= 0,02). Both studies demonstrate promising results in the treatment of cellulite.
Tanzi, et al. tested in their prospective study on the effectiveness of cellulite treatment through acoustic subcision an improvement of 1.01 on the Cellulite Severity Scale (CSS), with a mean baseline score of 3.41 after 12 weeks [14]. In addition, our study showed a decrease of 1.22 in the CR-PCSS in the treatment of cellulite with the use of laser-assisted liposuction after three months of follow-up, corroborating the findings of the current literature.
Bass, et al. performed a pooled analysis of two double- blind, randomized clinical trials to identify the effectiveness of mesotherapy as a treatment for cellulite, presenting clinically inspired results with an improvement in the CR- PCSS greater than 1 point after 71 days of collagenase clostridium histolyticum administration [15]. These results are consistent with our degree of improvement in the appearance of cellulite using laser-assisted liposuction.
Janette et al performed a trial to evaluate different techniques for treating cellulite of the buttocks and thighs [9]. Sixty-three women with buttock or thigh cellulite received ≥1 collagenase clostridium histolyticum dose. These techniques differed in various ways, such as the collagenase concentration and volume per injection, and injection depth, needle angle. The results showed that different collagenase injection techniques are needed for buttock cellulite versus thigh cellulite due to differences in efficacy and safety. Despite these differences, collagenase was efficacious and improved the appearance of cellulite in the buttocks and thighs using any combination of injection techniques. Comparatively, our study enrolled 12 female patients submitted to thigh cellulite treatment using laser-assisted liposuction. Our results were also promising, as there was a reduction of 1.22 points on the CR-PCS scale. Although both approaches are effective in treating cellulite, it is essential to consider that mesotherapy’s degree of efficiency and safety relies on the chosen technique.
DiBernardo, et al. guided a multicenter study in which fifty-seven patients underwent cellulite treatment using Nd: YAG laser energy [16]. At six months after treatment, blinded evaluators rated at least a 1-point improvement in the appearance of cellulite in 96% of treated sites. The laser treatment described by DiBernardo et al. presents satisfactory results in patients with a mean age similar to that used in this study. In addition, DiBernardo et al. study measured techniques’ efficacy in a six-month follow-up, reinforcing the success of this approach for an even more extended period than that analyzed in our study. Therefore the results presented by DiBernardo are encouraging as they corroborate our findings.
The photothermal energy causes the effects of laser- assisted liposuction. The laser light is converted to heat energy in the collagenous tissues and fat. Denaturation of structural proteins in the reticular dermis and collagenous fibrous septae should theoretically stimulate collagen remodeling. In addition, cytokines and growth factors released by laser-induced inflammatory cells are thought to correlate with increased collagen production causing tissue tightening. Laser-assisted liposuction is reported to reduce patient pain, increase safety, enhance tissue response, facilitate suctioning, and reduce recovery time [17, 18].
For this study, patients were treated bilaterally, with the baseline photo serving as a control for plastic surgeons’ evaluation; one limitation of our research is that patients may have different perceptions of treatment response than clinicians do. Studies with a short period are great to avoid confounding variables, however new studies involving a longer follow-up period will be of great value in defining the role of laser-assisted liposuction on thigh cellulite.
Conclusion
We have obtained comprehensive results demonstrating the role of laser-assisted liposuction on thigh cellulite. In addition, the evidence from our research suggests that laser- assisted liposuction reduces thigh cellulite.
References
-
Nürnberger F, Müller G (1978) So-called cellulite: an invented disease. J Dermatol Surg Oncol 4(3): 221-229.
-
Friedmann DP, Vick GL, Mishra V (2017) Cellulite: a review with a focus on subcision. Clin Cosmet Investig Dermatol 10: 17-23.
-
Tokarska K, Tokarski S, Woźniacka A, Sysa-Jędrzejowska A, Bogaczewicz J (2018) Cellulite: a cosmetic or systemic issue? Contemporary views on the etiopathogenesis of cellulite. Postepy Dermatol Alergol 35(5): 442-446.
-
Ponto T, Benson HAE, Wright A (2022) Reliability of a standardized tool for evaluating severity of cellulite in the female posterior thigh. J Cosmet Dermatol 5: 44-50.
-
Bennardo L, Fusco I, Cuciti C, Sicilia C, Salsi B, et al. (2022) Microwave Therapy for Cellulite: An Effective Non-Invasive Treatment. J Clin Med Res 11(3): 66-72.
-
Lim Y, Wulkan A, Avram M (2022) FDA MAUDE database reported adverse events on noninvasive body contouring, cellulite treatment, and muscle stimulation from 2015 to 2021. Lasers Surg Med 8: 71-88.
-
Przylipiak AF, Galicka E, Donejko M, Niczyporuk M, Przylipiak J (2013) A comparative study of internal laser-assisted and conventional liposuction: a look at the influence of drugs and major surgery on laboratory postoperative values. Drug Des Devel Ther 7: 1195-1200.
-
Shapira E, Plonski L, Menashe S, Ofek A, Rosenthal A, et al. (2022) High-Quality Lipoaspirate Following 1470-nm Radial Emitting Laser-Assisted Liposuction. Ann Plast Surg 89(6): e60-e68.
-
Kaufman-Janette J, Katz BE, Vijayan S, Xiang Q, Kaminer MS (2022) Evaluation of five collagenase clostridium histolyticum-aaes injection techniques for the treatment of cellulite on the buttock or thigh. J Cosmet Dermatol 21(4): 1448-1453.
-
Centurión P, Gamarra R, Caballero G, Kaufmann P, Delgado P (2020) Optimizing harvesting for facial lipografting with a new photochemical stimulation concept: One STEP techniqueTM. European Journal of Plastic Surgery 43: 733-742.
-
Soares JLM, Rocha VA, Sanudo A, Miot HA, Bagatin E (2022) Prevalence and factors associated with gynoid lipodystrophy in Brazilian adolescent girls: a cross- sectional study. Int J Dermatol 61(7): 861-866.
-
Emanuele E, Bertona M, Geroldi D (2010) A multilocus candidate approach identifies ACE and HIF1A as susceptibility genes for cellulite. J Eur Acad Dermatol Venereol 24(8): 930-935.
-
Emanuele E, Minoretti P, Altabas K, Gaeta E, Altabas V (2011) Adiponectin expression in subcutaneous adipose tissue is reduced in women with cellulite. Int J Dermatol 50(4): 412-416.
-
Tanzi EL, Capelli CC, Robertson DW, LaTowsky B, Jacob C, et al. (2022) Improvement in the appearance of cellulite and skin laxity resulting from a single treatment with acoustic subcision: Findings from a multicenter pivotal clinical trial. Lasers Surg Med 54(1): 121-128.
-
Bass LS, Kaufman-Janette J, Joseph JH, Kaminer MS, Clark J, et al. (2022) Collagenase Clostridium Histolyticum- aaes for Treatment of Cellulite: A Pooled Analysis of Two Phase-3 Trials. Plast Reconstr Surg Glob Open 10(5): e4306.
-
DiBernardo BE, Sasaki GH, Katz BE, Hunstad JP, Petti C, et al (2016) A Multicenter Study for Cellulite Treatment Using a 1440-nm Nd:YAG Wavelength Laser with Side- Firing Fiber. Aesthet Surg J 36(3): 335-343.
-
Centurion P, Caballero G, Weiss M (2019) Comment to: “Laser-Assisted Liposuction (LAL) Versus Traditional Liposuction: Systematic Review”. Aesthetic Plast Surg 43(4): 1122-1123.
-
Valente D, Gazzi G, Tuon A, Bellani DN, Sebastiany L, et al. (2022) Laser-Assisted Liposuction for Autologous Fat Grafting Following Elective Breast Explant Surgery. American Journal of Surgery and Clinical Case Reports 5(1): 1-8.
- Reconstruction of Nasal Defect Using a Local Flap Based in the Nanoperforants Concept: A Case Report
- Transplant Tourism in Japan: Insights from Nationwide Surveys and Emerging Ethical Challenges
- The Challenge of Peritoneal Vaginoplasty in Transgender Women: Review Literature and Personal Perspectives
- Algorithmic Paternalism: Autonomy Versus Automation
- Dermatoscopy in Gorlin Syndrome: Avoiding the Disfigurement in Patients
- How Artificial Intelligence is Ushering in a New Era of Innovation in General and Plastic Surgery: A Short Communication