The Use of Ultrasonic Cutting Devices to Decrease Risks in Temporomandibular Eminectomy
Purpose: This study aims to evaluate two different cutting devices in temporomandibular eminectomies. Materials and Methods: This retrospective cross-sectional, observational analytical study included a sample of 41 historical records of patients diagnosed with unilateral chronic condylar luxation who underwent eminectomy between January 2011 and May 2018. Patients records were divided into two groups: Group 1 consisted of 16 patients who underwent eminectomy with an ultrasonic device (Piezosurgery Medical II; Mectron), and Group 2 included 25 patients who underwent eminectomy with a traditional cutting device (reciprocating saw). Results: In group 1, mean pain was 3 and in group 2 the mean pain was 5. Patients in group 1 have a mean of 41 mm +/-2 in mouth opening and in group 2 a mean of 35 mm +/- 2.5. Also, there was a case of skin infection (6.25%), and only one patient in group 2 had facial nerve injury in their temporal branch (4%). Conclusions: Today, there are sufficient reasons to consider the use of ultrasonic devices in osteotomies, such as eminectomy, to increase patient safety by reducing the risks of perforations to critical anatomical structures where complications can be severe and postoperative outcomes improved should be another indication.
Introduction
Is defined joint luxation as the blockage of the condyle beyond the joint eminence, during its excessive translation in maximum opening movements; This can occur anterior, medial, lateral, or posterior to the joint fossa being the most frequent one is anterior to it. Furthermore, it can occur unilaterally (deviation of the mandible to the contralateral side) or bilaterally (mouth fully opened with limited movement) [1]. Different treatment suggested in the literature, where eminectomy is a viable option to solve this problem [2].
To manage these recurring events, it was Myrhaug, who first described this procedure in 1951, performing it in two patients who had habitual dislocation where he obtained good results by removing the articular eminence, avoiding this mechanical lock, and allowing the condyle to return to its glenoid cavity [3]. In 1987, Pogrel [4] published a study in which 15 patients were treated with an eminectomy to manage the temporomandibular joint’s dislocation because the condyle head was blocked in front of the joint eminence during maximum opening preventing normal closure. In a few cases, surgical treatment was necessary when block events become chronic, generating discomfort for the patient. Similarly, eminectomy has other uses in different disorders apart from condylar dislocation. Where eminectomy plays the role of a complementary procedure to provide more space for joint movements [5]. Recently, the use of piezoelectric devices has been increasing to perform osteotomies, due to the reduced risk of soft tissue injury, decreased bleeding, and providing accurate and safe cuts compared to traditional devices. All these advantages are due to the decrease in macro-vibrations that provide greater control during osteotomy [6].
This retrospective cross-sectional, observational analytical study aims to evaluate two different cutting devices in temporomandibular eminectomies concerning pain and maximal mouth opening, and risk of complications due to scarce information in this temporomandibular procedure.
Materials and Methods
This study included records of patients diagnosed with unilateral chronic condylar luxation who underwent eminectomy between January 2011 and May 2018 at the Hospital Universitario Fundación Santa Fe de Bogotá, Bogotá, Colombia. The same surgeon performed all the procedures through the modified endaural approach with sharp dissection under general anesthesia. Records were divided into two groups: Group 1 consisted of patients who underwent eminectomy with an ultrasonic device (Piezosurgery Medical II; Mectron), and Group 2 included patients who underwent eminectomy with a traditional cutting device (reciprocating saw).
Inclusion Criteria
The inclusion criteria were a series of patients diagnosed with unilateral chronic condylar luxation that requires eminectomy.
Exclusion Criteria
Patients who did not complete visits for complete data collection.
Demographic Information
The participants were asked to complete a questionnaire, providing their age (in years) and gender (male or female).
Clinical Diagnosis
The patients were diagnosed and classified following the clinical criteria.
Facial Palsy
Evaluated by the House and Brackmann facial nerve grading system (House and Brackmann 1985). Facial nerve function was evaluated among all patients postoperative immediate, fifth postoperative day, fifteen days, one month, six months, and a one-year follow-up [7].
Pain Evaluation
Visual analog scale (VAS) was used to evaluate pain. T1, a mean between immediately and eight hours later. T2 was the fifth postoperative day and T3 was 15 days later.
Range of Maximum Mouth Opening (MMO)
The TheraBite Scale (Lorenz Surgical, Jacksonville, Fla.) was used to record MMO (fifth postoperative day), asking patients to open their mouth as wide as possible at three different times, and placing the scale between the incisal edges of the upper and lower central, according to the recommendations of the maker. The average of the 3 measurements was reported as MMO.
Data Collection Process
The selection process began with reviewing records between January 2011 and May 2018. The patient information was organized in an Excel® sheet. Data collected included postoperative pain, the device employed, surgery year, age, gender, complications, and follow-up period.
Results
We analyzed 41 patients for the study (16 with piezosurgery and 25 with traditional cutting devices). The mean age of the patients evaluated was 26.9 years, with a range between 16 and 32 years old. In group 1, 37.5% (n: 6) corresponded to male patients and 62.5% (n: 10) were female patients. In group 2, 36% (n: 9) were male patients and 64% (n: 16) were female. Of the procedures performed (n: 41), 15 cases were on the left side, and 26 cases on the right side and all of them were unilateral. In group 1, there was a case of skin infection (6.25%), and only one patient in group 2 had facial nerve injury in their temporal branch (4%) (Table 1).
| Item | Patients |
|---|---|
| Patients (n=41) | |
| Sex | |
| Female | 26 |
| Male | 15 |
| Mean Age (y) | 26.9 |
| Surgery Side | |
| Right | 26 |
| Left | 15 |
| Allocation | |
| Group 1 (Piezoelectric cutting device) | 16 |
| Group 2 (Conventional cutting device) | 25 |
| Complications | |
| Group 1 | |
| Skin infection | 1 |
| Other | 0 |
| Group 2 | |
| Facial Nerve Injurie | 1 |
| Other | 0 |
| Mean VAS (Pain) | |
| Group 1 | 3 |
| Group 2 | 5 |
| Mean MMO | |
| Group 1 | 41 mm +/-2 |
| Group 2 | 35 mm +/-2.5 |
Table 1: Demographic And Clinical Data Of The Two Groups Evaluated.
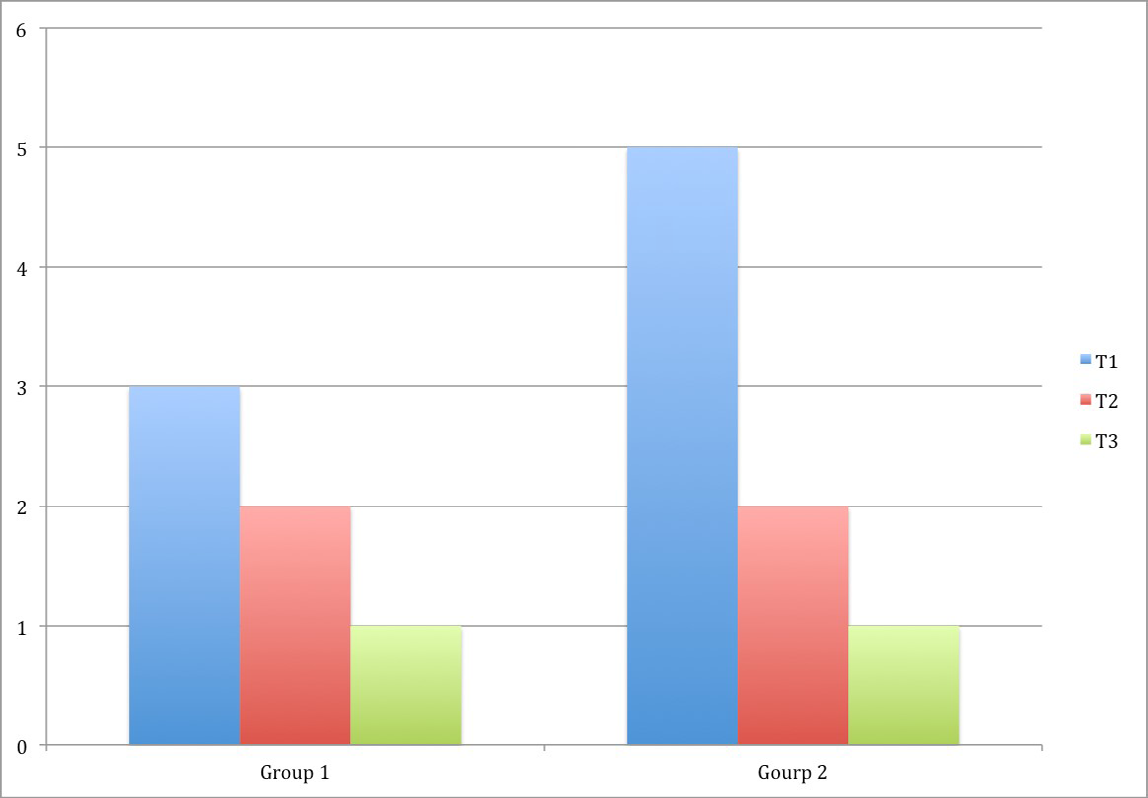
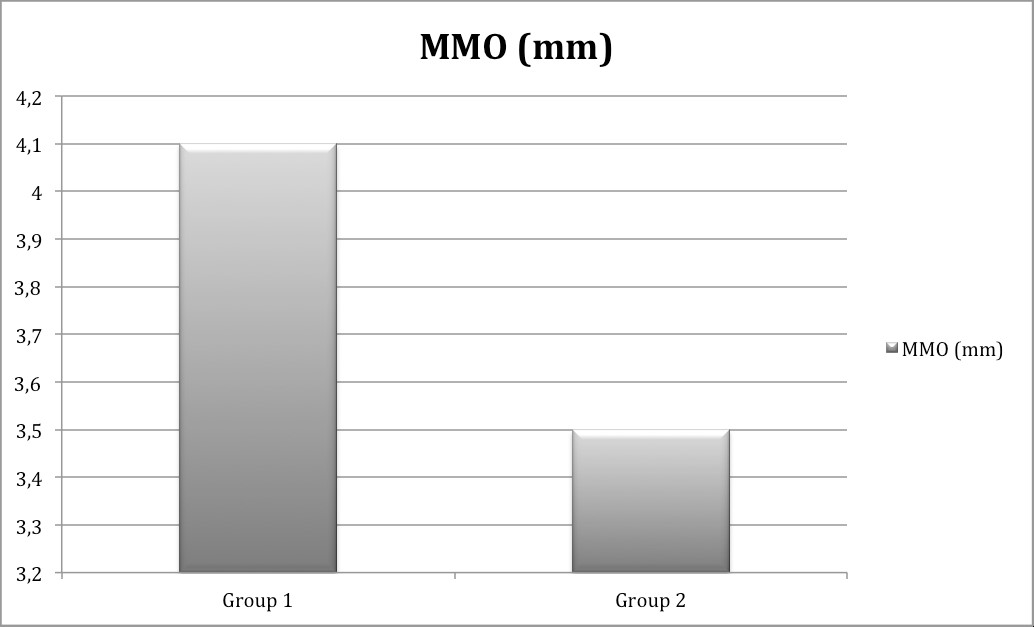
This lesion was found in a female patient, and this was successfully solved at the first control appointment after the fifth postoperative day. No other complications associated with surgery were presented, including those related to the middle cranial fossa in either of the two studied. Facial edema was significantly less in patients in group 1 than group 2. However, we do not have digital photographs to support the evidence. The postoperative pain in T1 was 3 in group 1, and in group 2 was 5. On the other hand in T2 and T3 there was no difference between groups being 2 in both groups in T2 and 1 in both groups in T3 (Figure 1). Finally, patients in group 1 have a mean of 41 mm +/-2 in mouth opening and in group 2 a mean of 35 mm +/- 2.5. (Figure 2).
Discussion
The risks of eminectomy are basically all related to the open and arthroscopic approaches that are carried out in the TMJ interventions. Among them, nerve damage and branches of the external carotid artery must be included [8]. Knowledge of the present anatomical structures related to the area and the dimensions of the articular eminence is vital to avoid penetrating the infratemporal fossa or the middle cranial fossa. Therefore, in the study by Hall, et al. [9] the importance of different measures is mentioned that will serve as a reference to avoid penetration of the middle cranial fossa. Are also the dimensions mentioned in different studies. The prior use of computed tomography is recommended to measure the degree of eminence pneumatization and prevent a possible perforation in the middle cranial fossa that causes a spinal fluid leak or exposure of the temporal lobe [10]. Taking this into account, a bone with significant pneumatization will be a bone that exerts little resistance and we can perforate easily. This increases the risk of causing damage to intracranial structures and its magnitude also depends on the cutting instruments used.
Goode, et al. [11] published a study in which they described their experience with eminectomy. In their paper, they mention the importance of the osteotomy being performed in the medial portion of the articular eminence. Since they had to re-intervene in a patient for incomplete bone resection due to persistent pain and the appearance of noise. Helman, et al. [12] published this time a study in 8 patients in which they observed through tomography the case of a patient who had no improvement due to incomplete osteotomy in the medial portion. This means that deepening the osteotomy in the middle direction, implies inserting more of a cutting instrument blindly.
Conventionally, the technique is performed with the help of chisels, rotary instruments, or an osteotomy saw. However, it is also mentioned the use of piezoelectric for these types of procedures. The latter provides different advantages regarding soft tissue safety and viability of bone tissue. Silva, et al. [8] compared the ultrasonic devices with a reciprocating saw in TMJ reconstruction where they found less bleeding and precise safe cuts [13]. Also, Spinelli, et al. [14] compared ultrasonic with different mechanical cutting devices where they found less bleeding and more precise cuts, making osteotomies safer and more controllable for the operator with a decrease in edema. However, it is reported the increase in the surgical times of the osteotomy. Gonzalez- Lagunas added the benefit of the decreased risk of damage to the meningeal vessels in case of perforation of the middle cranial fossa during eminectomy procedures [15]. For his part, in 2018, Isler, et al. [16] published a case report, showing their experience with the use of the piezoelectric for eminectomy, obtaining results of reduced bleeding and broad surgical vision during the osteotomy of the articular eminence. On the other hand, Charlote, et al. [17] carried out an anatomical study in corpses. They described the anatomical relationship of the articular eminence and other vital structures where a perforation in the dura or middle meningeal artery, a spinal fluid leak, or hemorrhage could occur in an eminectomy. The aforementioned are arguments that favor the use of instruments that reduce the risk of significant injuries.
Concerning pain in a previous study with a similar design to this one where ultrasound was used in condylectomies vs conventional cutting devices in a sample of 60 patients. We found that in the group where ultrasound was used, pain decreased from 4 to 1 on the visual analog scale. The hypothesis is that conventional devices, by generating greater reheating of the bone and more tissue damage producing greater edema and pain. Additionally, the need to work more on the flaps to protect the soft tissue from conventional cutting devices requires greater retraction and greater tissue manipulation which is reflected in postoperative pain and edema [18].
Although different studies have widely studied the benefit of ultrasonic cutting devices, postoperative pain in eminectomy has not been studied. However, one of the benefits of its use in these procedures could be the use of a cutting tool that can protect soft tissues, especially in an area where critical anatomical structures are very close to the surgical area. Most of the sample included women and this may be related to the largest number of consultations for atm symptoms in this gender. Regarding the only reversible facial nerve injury that there was, it is believed that it was due to a greater retraction of the tissue to achieve a cut protecting the soft tissue around it. Even though one of the major limitations of this study was the subjective evaluation of edema, we believe that it may be an influencing factor in the difference in postoperative pain. Finally, on the other hand, edema and pain also influenced the opening range, which was higher in group 1 since, having less pain, they started opening therapy earlier.
Conclusion
Although fortunately in our study there were no major intracranial complications, we believe that there are sufficient reasons to consider the use of ultrasonic devices in these osteotomies. The most important is to increase patient safety by reducing the risks of perforations to critical anatomical structures where complications can be severe and also better postoperative for patients.
References
-
Martins WD, Ribas Mde O, Bisinelli J, França BH, Martins G (2014) Recurrent dislocation of the temporomandibular joint: a literature review and two case reports treated with eminectomy. Cranio 32(2): 110-117.
-
Liddell A, Perez DE (2015) Temporomandibular joint dislocation. Oral Maxillofac Surg Clin North Am 27(1): 125-136.
-
Myrhaug H (1951) A new method of operation for habitual dislocation of the mandible; review of former methods of treatment. Acta Odontol Scand 9(3-4): 247- 260.
-
Pogrel MA (1987) Articular eminectomy for recurrent dislocation. Br J Oral Maxillofac Surg 25(3): 237-243.
-
Williamson R, McNamara D, McAuliffe W (2000) True eminectomy for internal derangement of the temporomandibular joint. Br J Oral Maxillofac Surg 38(5): 554-560.
-
Labanca M, Azzola F, Vinci R, Rodella LF (2008) Piezoelectric surgery: twenty years of use. Br J Oral Maxillofac Surg 46(4): 265-269.
-
House JW, Brackmann DE (1985) Facial nerve grading system. Otolaryngol Head Neck Surg 93(2): 146-147.
-
Undt G (2011) Temporomandibular Joint Eminectomy for Recurrent Dislocation. Atlas Oral Maxillofac Surg Clin North Am 19(2): 189-206.
-
Hall MB, Randall WB, Sclar AG (1984) Anatomy of the TMJ articular eminence before and after surgical reduction. J Craniomandibular Pract 2(2): 135-140.
-
Jeyaraj P (2017) Chronic Recurrent Temporomandibular Joint Dislocation: A Comparison of Various Surgical Treatment Options, and Demonstration of the Versatility and Efficacy of the Dautrey’s Procedure. J Maxillofac Oral Surg 17(1): 95-106.
-
Goode RL, Linehan JE (1973) Recurrent mandibular dislocation, relieved by removal of articular eminence. Arch Otolaryngol 98(2): 97-99.
-
Helman J, Laufer D, Minkov B, Gutman D (1984) Eminectomy as surgical treatment for chronic mandibular dislocations. Int J Oral Surg 13(6): 486-489.
-
Silva R, Gupta R, Tartaglia G, Connelly S (2017) Benefits of using the ultrasonic BoneScalpel™ in temporomandibular joint reconstruction. J Craniomaxillofac Surg 45(3): 401- 407.
-
Spinelli G, Valente D, Mannelli G, Raffaini M, Arcuri F (2017) Surgical management of ankyloses of the temporomandibular joint by a piezoelectric device. J Craniomaxillofac Surg 45(4): 441-448.
-
Gonzalez-Lagunas J (2017) Is the piezoelectric device the new standard for facial osteotomies? J Stomatol Oral Maxillofac Surg 118(4): 255-258.
-
Isler SC, Cakarer S, Yalcin BK, Sitilci T (2018) Management of the bilateral chronic temporomandibular joint dislocation. Ann Maxillofac Surg 8(1): 154-157.
-
Charlote W, Iwanaga J, Oskouian RJ, Tubbs RS (2018) Anatomical Examination of Mandibular Condyle Protrusion Into the Middle Cranial Fossa. J Craniofac Surg 29(4): 1069-1071.
-
Tumiñan AP, Morales CL, López JP, Orjuela MP (2020) Piezoelectric Cutting Devices for Osteotomy in Temporomandibular Joint Condylectomy. J Craniofac Surg 31(8): e800-e802.
- Reconstruction of Nasal Defect Using a Local Flap Based in the Nanoperforants Concept: A Case Report
- Transplant Tourism in Japan: Insights from Nationwide Surveys and Emerging Ethical Challenges
- The Challenge of Peritoneal Vaginoplasty in Transgender Women: Review Literature and Personal Perspectives
- Algorithmic Paternalism: Autonomy Versus Automation
- Dermatoscopy in Gorlin Syndrome: Avoiding the Disfigurement in Patients
- How Artificial Intelligence is Ushering in a New Era of Innovation in General and Plastic Surgery: A Short Communication