Is There a Superior Method of Reconstruction After Mohs Surgery in Terms of Cosmesis?: A Case Report and Review of Literature
Background: Mohs micrographic surgery (MMS) offers extreme precision and effectiveness when excising skin cancer. Careful reconstruction after Mohs surgery can minimize postoperative complications and determine the patient’s cosmetic outcome. There are several methods of reconstruction that a surgeon may opt for based on the defect size, location, depth, and the patient's skin laxity. The most common techniques for reconstruction after Mohs surgery are adjacent tissue transfer (ATT), full-thickness skin grafts (FTSG), and secondary intention (SI). All of these surgical techniques have proven to be safe and effective methods of reconstruction after Mohs surgery, however there is a long standing debate of which reconstructive technique produces the most desirable cosmetic outcomes. Methods: We report the case of a 78 year old female patient who underwent Mohs surgery and reconstruction at our practice, for three separate cases of basal cell carcinoma on the face. The first reconstruction was performed through ATT, the second through SI with the use of topical bovine collagen powder, and the third was closed through secondary intention with three applications of an amniotic graft. The outcomes were compared to assess if the reconstructive method after Mohs surgery has a significant impact on cosmesis. Verbal and written consent from the patient was obtained for publication. Results: The cosmetic results after reconstruction were graded as excellent, good, moderate, hypertrophied, or keloid, based on a modified Vancouver Scar Scale. Our findings showed that ATT produced a superior result compared to secondary intention with the use of collagen powder. The defect treated with the amniotic graft showed a faster wound healing rate compared to the defect closed by SI and collagen powder. Based on the wound closure rate and findings in related literature, we expect that the defect treated with the amniotic membrane will produce a more appealing cosmetic result than the defect treated with collagen powder.
Introduction
Skin cancer is the most common type of malignancy in the United States, a statistic that is expected to continue to rise [1]. Basal cell carcinoma (BCC) is the most common skin cancer across all races and ethnicities, closely followed by squamous cell carcinoma (SCC) [2, 3]. BCC and SCC make up 99% of all non-melanoma skin cancers (NMSC) [4].
Cutaneous malignancies are most often found on the face due to consistent sun exposure, in fact, about 80% of all cases of basal cell carcinoma are found on the face [5]. Skin cancer can be treated with radiation, topical treatments, or surgically, depending on the size of the lesion, as well as the patient’s and provider’s preference. Standard surgical excision of skin cancer uses predetermined margins and is most often used for tumors on the trunk or extremities [6]. When performed on small (<1cm) facial malignancies with smaller margins, the percent of positive margins can be as high as 24% [7]. When operating on facial tumors, surgeons typically want to spare tissue in order to minimize the cosmetic defects, however this can lead to positive margins and recurrence of cancerous cells.
The Mohs Micrographic Surgery (MMS) is an excellent choice for removing skin cancer from the face because it maximizes the amount of healthy tissue left intact, while also consistently leaving clean margins [8]. MMS is the most precise and effective method of removing skin cancer, with a 99% cure rate for primary BCC [6]. Mohs surgery is performed by a Mohs micrographic surgeon and involves removing thin layers of tissue from the affected area. The tissue is prepared by a histotechnician and is evaluated by the surgeon under a microscope to determine if the surgical margins are clear. If it is determined that cancerous cells are persisting, the patient is returned to the operating room for a second stage of Mohs surgery [9]. This method leaves as much healthy tissue as possible and has shown to be incredibly effective.
After removing several layers of skin and tissue, the patient is left with a rather large open wound that needs to be properly closed to avoid infection and minimize scarring. This is where reconstructive surgery plays a role. Malignancies on the face present an anatomical challenge during reconstruction. Not only is it crucial to retain original function, but it is also important to consider the cosmetic outcome for patients during reconstruction of facial defects. Reconstruction after Mohs surgery requires careful and deliberate technique, and it is up to the surgeon to choose the proper method of reconstruction for the patient’s needs. Many factors play a role in the surgeon’s decision, such as the defect size, location, depth, the surgeon’s experience, and the patient’s skin laxity [10]. There are several different methods of reconstruction, such as a linear direct closure, adjacent tissue transfer, skin grafts, and secondary intention. Despite there being a long standing debate of which method of reconstruction produces superior cosmetic results, there is not much data published on the topic. This can be a difficult topic to study when comparing results from multiple patients because individuals have different rates of wound healing based on age, genetics, medical conditions, and lifestyle. It is also challenging to compare results produced from different reconstructive surgeons because they may differ in skillset or expertise. We present a unique case in which a single patient underwent three Mohs surgeries with the same Mohs micrographic surgeon, and three different methods of reconstructive surgery with the same plastic surgeon. This allows us to compare the results of ATT, SI with collagen powder, and SI with an amniotic graft, while controlling for the patient’s individual rate of wound healing and the surgeon’s skill.
Case Presentation
Case Report and Surgical Technique
We report the case of a 78 year old female who was diagnosed with basal cell carcinoma three separate times at our practice. The patient has a history of breast cancer, chronic obstructive pulmonary disease (COPD), hypertension, and was a former smoker. In 2020, the patient came into the office with a growth on the right lateral nasal sidewall, as shown in Figure 1, and had a biopsy performed. The results of the biopsy confirmed that the growth was basal cell carcinoma. The lesion required tissue conservation for optimal results, therefore Dr. Michael Messina, a board certified dermatologist and Mohs micrographic surgeon, elected Mohs surgery as the best option for the patient. The risks of bleeding, infection, discomfort, recurrence, and scar formation were explained to the patient in lay terms. The growth was outlined with a sterile surgical marker, and was excised using a 45 degree bevel excision. The tissue was divided and prepared by a histotechnician and observed under a microscope. It was determined that there were cancerous cells persisting, so the patient was returned to the operating room for a second stage of surgery. The tissue was again oriented, mapped, dyed, and submitted for Mohs frozen sections. The specimens were once again inspected under a microscope and it was determined that the margins were clear. The resultant defect, shown in Figure 2, measured 1.3 x 1.7 cm. The patient was referred to board certified plastic surgeon, Dr. Natalie Driessen, for reconstruction. Considering the defect size and location, the patient’s skin laxity, and the objective of achieving maximal preservation of function and appearance, it was elected to create an advancement flap as the closure method. The proposed lines of the flap were marked with a sterile marking pen in the lateral positions. Incisions were made along the marked lines and the flap was elevated. After achieving appropriate undermining and complete hemostasis, the flap was advanced into position and secured with 3-0 Monocryl sutures. The superficial cuticular margins were then approximated with 6-0 Prolene sutures. The results immediately after the reconstruction can be seen in Figure 3.



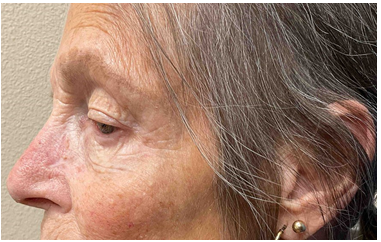
The patient returned in 2021 for a spot on the left nasal sidewall, seen in Figure 4, which was again confirmed through biopsy to be basal cell carcinoma. Dr. Messina recommended MMS in order to retain maximum function and cosmetic appearance. The risks of the procedure were once again explained to the patient and any questions were answered. The region was outlined with a sterile surgical marker and was excised with a 45 degree bevel excision. The surgery was performed as described above, again requiring 2 stages in order to achieve clean margins. The full-thickness defect after Mohs surgery is shown in Figure 5, and measured 1.5 x 1.3 cm. The patient was referred to Dr. Driessen for reconstruction. The different alternatives of closure methods were discussed with the patient, and based on the defect size and location it was decided that the best closure method for the patient would be secondary intention.


The patient was instructed to keep the wound clean and dry and to apply topical bovine collagen powder and 2% mupirocin ointment daily to increase the rate of healing and avoid infection.

Lastly, in 2023 the patient returned to our office for a small growth on the left medial cheek, shown in Figure 6, which was confirmed through biopsy as BCC. The patient underwent Mohs surgery a third time with Dr. Messina in early 2024. The margins were clear after 2 stages of the procedure and the patient was referred to Dr. Driessen for reconstruction. The defect measured 0.8 x 0.5 x 0.2 cm and is shown in Figure 7. After thoroughly discussing the alternatives, it was decided to use an amniotic graft to help increase the rate of wound closure through secondary intention. The graft was applied, along with 2% mupirocin ointment, adaptic, telfa, tegaderm, and brown tape in order to secure the graft. The patient was instructed to keep the dressing dry and to leave in place for 7 days until follow up.

Post-Operative Outcomes
Six days after the adjacent tissue transfer on the right lateral nasal sidewall in 2020, the patient returned to the office for a follow up and suture removal. The wound appeared to be healing nicely with no signs of postoperative complications. The reconstruction is considered a success due to the preservation of function, overall appearance, and minimal scarring. The patients’ result from one year post- op is shown in Figure 8. After the second Mohs surgery on the left lateral nasal sidewall in 2021, the patient allowed the wound to close through secondary intention and applied collagen powder to assist in the healing process. By 12 weeks, the wound had completely closed. The patient experienced no complications, and the result from the 17 month follow up is shown in Figure 9.


Following the third Mohs surgery on the left medial cheek, an amniotic graft was applied to the wound and secured with dressings. The patient was instructed to keep the dressings dry for one week and return to the office for a follow up. At the one week follow up appointment, the wound appeared to be healing well, however it was still open, which is expected at only one week post-op. An amniotic graft was applied again and the patient returned one week later. At the two week follow up, the granulating wound appeared to be smaller in size and looked to be healing nicely. An amniotic graft was applied a third and final time to increase the rate of wound closure. By the three week follow-up, the wound was assessed and it was decided to allow the wound to close through secondary intention without any more applications of the amniotic graft. The results from the one week, three week, five week, and eight week follow up appointments are shown in Figures 10-13.



Discussion
The most common methods of reconstruction after Mohs surgery includes adjacent tissue transfer (ATT), full-thickness skin grafts (FTSG), direct linear closure, and secondary intention (SI). Adjacent tissue transfer, also referred to as a skin flap closure, involves moving the adjacent skin to cover a neighboring defect. There are several different types of flaps that can be created depending on the size, shape, and location of the defect. For defects on the nasal tip, a horizontal advancement flap, also called an East-West flap, is often used [11]. This is a fairly simple surgical technique that can repair larger, full-thickness defects. The bilobed transposition flap is also commonly used for nasal defects [12]. Since this approach creates two lobes, it produces a more even distribution of tension, resulting in a more appealing cosmetic result, and can increase the speed of wound healing [13, 14]. Skin flaps are the most common type of closure after Mohs surgery because they consistently produce excellent cosmetic results and low postoperative complications [15, 16].
Autografts, a type of skin graft in which the patient is both the donor and recipient, are also a common choice for post-Mohs reconstruction. Skin grafts, which can either be full-thickness or split-thickness, are pieces of healthy skin that are removed from a donor site on the patient and reattached on the affected area. A full-thickness skin graft (FTSG) includes the full thickness of the dermis and epidermis, while a split-thickness graft includes the full epidermis and a variable thickness of the dermis [17]. Due to the depth of a typical Mohs surgery, full-thickness skin grafts are more commonly used in reconstruction. Unlike skin flaps, skin grafts are completely detached from the blood supply until they are reattached at the recipient site. Angiogenesis must occur in order to revascularize the skin graft, which typically occurs around 48 hours after surgery [18]. Revascularization is critical for the survival of the skin graft and without it the patient is at risk for complications such as necrosis, infection, or contracture [19]. Skin grafts can also be more time consuming than other methods due to the creation of a second surgical site [20]. There are some instances where skin grafts must be used instead of ATT, for example, if the defect is so large that creating a flap will pull on the surrounding skin and cause visual deformities. However, studies have shown that in cases where both ATT or FTSG can be used, ATT should be preferred due to better cosmetic results [15, 16]. Since skin grafts are taken from a different part of the body, typically the abdomen or behind the ear, there can be a mismatch in skin color and texture. This mismatch can cause the final cosmetic result to be not as appealing as those produced from ATT.
Direct linear closures are also a common reconstructive technique after Mohs surgery. This method is less complex and time-consuming compared to flap closures and skin grafts, and consistently produces acceptable clinical results. In order to perform a direct linear close without distorting surrounding tissue, the patient must have enough skin laxity, and the lesion should not be greater than 10mm [21].
For more superficial defects or in concave regions such as the nasal sidewall or ala, secondary intention has shown to produce superior cosmetic results [22]. This method allows the wound to close on its own, eventually being filled with granulation tissue [23]. Healing through secondary intention occurs in four stages: Hemostasis, an inflammatory stage, a proliferative stage, and a remodeling stage [22]. The hemostasis stage mainly consists of vasoconstriction of smooth muscle cells in order to stop further blood loss. Platelets then coagulate at the wound site and release cytokines, which begin the first signaling cascade in wound healing. Platelet derived growth factor (PDGF), interleukin-1 (IL-1), transforming growth factor (TGF)-α and TGF-β, epidermal growth factor (EGF), and insulin growth factor (IGF) are all released and begin to attract neutrophils and macrophages to the site [24]. These immune cells help clear bacteria from the wound, which is critical in the wound healing process. The inflammatory stage involves the amplification of this signal that is recruiting immune cells to the area. Hydrogen peroxide is released, which further attracts neutrophils, activates angiogenesis, and regenerates keratinocytes [25]. Macrophages then begin to phagocytose cellular debris and release molecules that activate endothelial cells, keratinocytes, and fibroblasts. The proliferative stage, also called the granulation stage, occurs when activated fibroblasts begin to release a new extracellular matrix and stroma, and new blood vessels are formed. This is the beginning of tissue repair and wound contraction. Eventually, the wound closes through a type II epithelial-mesenchymal transition (EMT), which explains how keratinocytes loosen their cell-cell connections and begin to cover the wound site. Finally, in the remodeling stage, the granulation tissue is remodeled and degraded by tissue inhibitors of metalloproteinases released by myofibroblasts [26]. Part of this process includes replacing collagen type III which is present in the granulation tissue with collagen type I, a stronger type of collagen fiber. Disturbances in the remodeling stage can cause chronic wounds, hypertrophic scars, and keloid scarring [27, 28, 29]. Wound healing occurs in an upward and inward direction, often resulting in a scar that is much smaller than the original wound. Healing through SI after Mohs-surgery is often overlooked, however it can be preferred in specific situations depending on the wound characteristics. Healing through secondary intention typically takes longer and can cause more discomfort to the patient compared to other methods of closure [21]. This has sparked research focused on developing tools that increase the rate of wound healing through SI. Amniotic tissue derived allografts (ATDA), have shown to increase the speed of wound healing in diabetic and refractory wounds, and are now being used on post-Mohs surgery wounds [30].
The amniotic membrane (AM) is the inner lining of the placenta, offering protection, transportation of essential molecules, growth factors, and cytokines to the fetus [31]. This membrane has several beneficial properties that have made it of interest to biomedical researchers for wound healing, including, an antibacterial effect, anti-scarring, anti-adhesive, anti-inflammatory, regulation of angiogenesis, promotion of epithelization, and the support for cell adhesion and growth. Native amniotic membrane is processed into an acellular, lyophilized membrane that contains extracellular matrix (ECM), growth factors, and cytokines, which as described in the previous paragraph, support wound healing. These are essential molecules in wound healing and help to avoid the development of chronic wounds, hypertrophic scars, and keloid scars [27, 28, 29]. There have been several clinical trials studying the effects of using human amniotic membrane to support healing in ophthalmic wounds, burns, dermatitis, surgery, and diabetic ulcers [32]. The use of a lyophilized amniotic membrane showed to enhance the healing process and support the complete epithelialization of diabetic foot ulcers [33]. In a study comparing the wound healing rates of ulcers, it was found that zero out of the 11 control groups’ ulcers reduced in size over the study period, while 14 of the experimental groups’ ulcers treated with the amniotic graft completely healed within 14-60 days [34]. In a preliminary study by Seaton, et al., the effects of ADTA on wound healing after Mohs-surgery were studied [30]. Although there was no significant difference in the rate of wound healing found between the ADTA and the control group overall, when the initial defect size was normalized, there was a significant difference found. Suggesting that the use of ADTA does have an effect on wound healing rate, but the size of the wounds must be similar when comparing. Another study focused on maxillofacial defects, found a significant difference in scar pliability and pigmentation 3 months post-op between wounds treated with an amniotic membrane and those treated with a collagen membrane [35]. The results showed better cosmetic results for the wounds treated with the human amniotic membrane. Although larger studies are needed to confirm the results, these studies suggest that the use of ADTA may increase the speed of wound healing and produce more appealing cosmetic outcomes. It is important to remember that individual patients may differ in speed of wound healing due to differences in medical history, age, and lifestyle habits such as smoking, which may affect their cosmetic outcomes as well. This is extremely difficult to control for when studying wound healing on multiple patients. Our report presents a unique case because three different closure methods were used on the same patient, therefore controlling for the potential differences in individual wound healing rates.
The patient’s first case of BCC on the right lateral nasal sidewall was closed by creating an advancement flap and suturing, shown in Figure 3. The twelve month follow up is shown in Figure 8. The resulting scar is scored based off of a modified Vancouver Scar Scale (VSS), which assigns a score for four categories: Pigmentation, pliability, vascularity, and height. A total score of 0 means that the scar was normal in all of these categories and represents the best possible cosmetic outcome [36]. A score of 13 represents the worst possible cosmetic outcome. The scar from the patient’s first Mohs surgery scored 0 in all of these categories, which is considered an “excellent” cosmetic outcome [36]. The second case of BCC which occurred on the patient’s left nasal sidewall, shown in Figure 4, was slightly smaller than the first, and was inferior and medial on the nose. It was elected to allow the wound to heal through secondary intention along with the use of bovine collagen powder, which is thought to increase the speed of epithelialization in wound healing [37]. The result from 17 months post-op is shown in Figure 9. Using the criteria from the VSS, the patient appears to have normal vascularity, pliability, and height on the area. The scar does appear to have a slight difference in pigmentation, scoring a 1 in this category. This qualifies the cosmetic result to be considered a “good” outcome on the VSS. Although both methods produced appealing cosmetic results, the outcome from ATT is superior to the result from secondary intention. The defect from the patient’s third Mohs surgery on the left medial cheek was closed through secondary intention with an amniotic graft. The progress of wound closure can be seen in Figures 10-13. By five weeks post-op and three applications of the amniotic graft, the wound was completely closed and much smaller in size compared to the initial defect. This is much sooner than the time it took the previous defect to close through SI with collagen powder. Based on the criteria in the VSS, the third defect shows normal height, pliability, and vascularity. There is slight hyperpigmentation, scoring 1 point in the category. This qualifies the third defect to be considered a “good” outcome, similar to the previous defect on the left lateral nasal sidewall. It is important to point out that this outcome is only 8 weeks post-op, while the other defects are over a year post-op. Based on how quickly the wound from the third Mohs surgery healed, as well as the findings in related literature, we expect that the defect treated with the amniotic graft will produce a better cosmetic outcome than the defect closed through secondary intention with collagen powder, but that ATT will be superior to both methods. Additional studies are needed to explore this concept further.
Conclusion
In conclusion, we present a unique case in which an individual patient underwent three different methods of reconstruction after Mohs surgery. The defects were similar in size and anatomical area, had the same Mohs surgeon for excision, and the same plastic surgeon for reconstruction. These controls allow the outcomes from the different methods of reconstruction to be compared to determine if there is a superior method of reconstruction in terms of cosmetic outcome. Our findings suggest that adjacent tissue transfer produces superior results compared to secondary intention with collagen powder based on the total score on a modified Vancouver Scar Scale for postoperative scars.
Although both methods produced highly acceptable results and had no postoperative complications, the scar from ATT showed normal pigmentation, while the scar from SI showed hypopigmentation. The results were comparable because they were in similar anatomical regions, close in size, and the images were taken around one year post-op. The third case of reconstruction healed through secondary intention with an amniotic graft and although the final result cannot be compared due to the timing of the surgery, the rate of wound closure was much faster than the previous defect that closed through secondary intention with collagen powder. This scar also scored well on the VSS despite only being 8 weeks post- op. Based on the literature and the impressive healing time, we expect that the defect treated with the amniotic graft will have a better cosmetic outcome than the defect closed by SI and collagen powder, however we believe that ATT will be superior to both methods. This study is limited by sample size and the results should be compared again once the one year post-op results from the defect treated with the amniotic graft become available. More studies are needed to compare the methods of reconstruction further, however our case report suggests that adjacent tissue transfer produces superior cosmetic results on facial defects after Mohs surgery when compared to SI with collagen powder and amniotic grafts.
Consent
The consent for publication was obtained from the patient.
References
-
Bradford PT (2009) Skin Cancer in Skin of Color. Dermatol Nurs 21(4): 170-178.
-
Rogers HW, Weinstock MA, Feldman SR, Coldiron BM (2015) Incidence Estimate of Nonmelanoma Skin Cancer (Keratinocyte Carcinomas) in the U.S. Population, JAMA Dermatol 151(10): 1081-1086.
-
Lukowiak TM, Aizman L, Perz A, Miller CJ, Sobanko JF, et al. (2020) Association of Age, Sex, Race, and Geographic Region With Variation of the Ratio of Basal Cell to Cutaneous Squamous Cell Carcinomas in the United States. JAMA Dermatol. 156(11): 1192-1198.
-
Ciążyńska M, Lange D, Lewandowski B, Reich A, Sławińska M, Pabianek M, et al. (2021) The Incidence and Clinical Analysis of Non-melanoma Skin Cancer. Sci Rep 11(1): 4337.
-
Wollina U, Bennewitz A, Langner D (2014) Basal Cell Carcinoma of the Outer Nose: Overview on Surgical Techniques and Analysis Of 312 Patients. J Cutan Aesthet Surg 7(3): 143-150.
-
Lewin JM, Carucci JA (2015) Advances in the Management of Basal Cell Carcinoma. F1000Prime Rep 12(7): 53.
-
Kimyai-Asadi A, Alam M, Goldberg LH, Peterson SR, Silapunt S, et al. (2005) Efficacy of Narrow-margin Excision of Well-demarcated Primary Facial Basal Cell Carcinomas. J Am Acad Dermatol 53(3): 464-468.
-
Bittner GC, Cerci FB, Kubo EM, Tolkachjov SN (2021) Mohs micrographic surgery: a review of indications, technique, outcomes, and considerations. An Bras Dermatol 96(3): 263-277.
-
Prickett KA, Ramsey ML (2023) Mohs Micrographic Surgery. In: StatPearls. StatPearls Publishing, Treasure Island, Florida, USA.
-
Visconti MJ, Archibald LK, Shahwan KT, Kimyon RS, Bakker C, et al. (2023) Nasal reconstructive techniques following Mohs surgery or excisions: a systematic review. Arch Dermatol Res 315(3): 333-337.
-
Cason RW, Shammas RL, Pyfer BJ, Glener AD, Marcus JR, et al. (2021) Cutaneous Reconstruction of the Nasal Distal Third: Alternative Local Flaps for a Complex Region. Plastic and reconstructive surgery. Global open 9(5): e3444.
-
Mole RJ, Hohman MH, Sebes N (2023) Bilobed Flaps. In: StatPearls. StatPearls Publishing, Treasure Island, Florida, USA.
-
Bednarek RS, Sequeira Campos M, Hohman MH, Ramsey ML (2023) Transposition Flaps. In: StatPearls. StatPearls Publishing, Treasure Island, Florida, USA.
-
Horeman T, Meijer Ej, Harlaar JJ, Lange JF, van den Dobbelsteen JJ, et al. (2013) Force Sensing in Surgical Sutures. PLOS ONE 8(12): e84466.
-
Fronek LF, Dorton D (2022). Surgical Outcomes Following Mohs Micrographic Surgery for Basal Cell Carcinoma on the Distal Third of the Nose. J Clin Aesthet Dermatol 15(6): 32-36.
-
Jacobs MA, Christenson LJ, Weaver AL, Appert DL, Phillips PK, et al. (2010) Clinical outcome of cutaneous flaps versus full-thickness skin grafts after Mohs surgery on the nose. Dermatol Surg 36(1): 23-30.
-
Ramsey ML, Walker B, Patel BC (2023) Full-Thickness Skin Grafts. In: StatPearls. StatPearls Publishing. Treasure Island, Florida, USA.
-
Weathers WM, Bhadkamkar M, Wolfswinkel EM, Thornton JF (2013) Full-thickness skin grafting in nasal reconstruction. Seminars in plastic surgery 27(2): 90- 95.
-
Davis M, Baird D, Hill D, Layher H, Akin R (2021) Management of full-thickness skin grafts. Proc (Bayl Univ Med Cent) 34(6): 683-686.
-
Prohaska J, Cook C (2023) Skin Grafting. In: StatPearls. StatPearls Publishing, Treasure Island, Florida, USA.
-
Pedersen SJ, Paoli J, Gniadecki R, Glud M (2023) Repair of Defects of the Nasal Tip After Mohs Surgery. Dermatology practical & conceptual 13(4): e2023228.
-
Liu KY, Silvestri B, Marquez J, Huston TL (2020) Secondary Intention Healing After Mohs Surgical Excision as an Alternative to Surgical Repair: Evaluation of Wound Characteristics and Esthetic Outcomes. Annals of plastic surgery 85(S1): S28-S32.
-
Alhajj M, Goyal A (2022) Physiology, Granulation Tissue. In StatPearls. StatPearls Publishing, Treasure Island, Florida, USA.
-
Sorg H, Sorg CGG (2023) Skin Wound Healing: Of Players, Patterns, and Processes. Eur Surg Res 64(2): 141-157.
-
Vliet AVD, Janssen-Heininger YM (2014). Hydrogen peroxide as a damage signal in tissue injury and inflammation: murderer, mediator, or messenger?. Journal of cellular biochemistry 115(3): 427-435.
-
Caley MP, Martins VL, O’Toole EA (2015) Metalloproteinases and Wound Healing. Advances in wound care 4(4): 225-234.
-
Amadeu T, Braune A, Mandarim-de-Lacerda C, Porto LC, Desmoulière A, et al. (2003) Vascularization pattern in hypertrophic scars and keloids: a stereological analysis. Pathology, research and practice 199(7): 469-473.
-
Telgenhoff D, Shroot B (2005) Cellular senescence mechanisms in chronic wound healing. Cell death and differentiation 12(7): 695-698.
-
Yates CC, Krishna P, Whaley D, Bodnar R, Turner T, et al. (2010) Lack of CXC chemokine receptor 3 signaling leads to hypertrophic and hypercellular scarring. The American journal of pathology 176(4): 1743-1755.
-
Seaton K, Mullens D, Barr J, Hull E, Averitte R (2021) Use of Amniotic Tissue-Derived Allografts Post-Mohs Micrographic Surgery: A Preliminary Study Assessing Wound Closure Rate. Wounds 33(7): 185-191.
-
Dadkhah Tehrani F, Firouzeh A, Shabani I, Shabani A (2021) A Review on Modifications of Amniotic Membrane for Biomedical Applications. Front Bioeng Biotechnol 8: 606982.
-
Silini AR, Cargnoni A, Magatti M, Pianta S, Parolini O (2015) The Long Path of Human Placenta, and Its Derivatives, in Regenerative Medicine. Front Bioeng Biotechnol 3: 162.
-
Zelen CM, Serena TE, Snyder RJ (2014) A prospective, randomised comparative study of weekly versus biweekly application of dehydrated human amnion/ chorion membrane allograft in the management of diabetic foot ulcers. Int Wound J 11(2): 122-128.
-
ElHeneidy H, Omran E, Halwagy A, Al-Inany H, Al-Ansary M, et al. (2016) Amniotic membrane can be a valid source for wound healing. Int J Womens Health 8: 225-231.
-
Munoyath SK, Sathishwaran J, Prasad K (2015) Efficacy of human amniotic membrane and collagen in maxillofacial soft tissue defects – A comparative clinical study. Journal of Oral and Maxillofacial Surgery Medicine and Pathology 27(6): 786-790
-
Oh EM, Chung YS, Lee YD (2013) Assessment of Postoperative Scar Using Modified Vancouver Scar Scale of 283 Patients Who Underwent Open Thyroidectomy in a Single Institution. Korean J Endocrine Surg 13: 25-31.
-
Kolenik SA 3rd, McGovern TW, Leffell DJ (1999) Use of a lyophilized bovine collagen matrix in postoperative wound healing. Dermatol Surg 25(4): 303-307.
- Reconstruction of Nasal Defect Using a Local Flap Based in the Nanoperforants Concept: A Case Report
- Transplant Tourism in Japan: Insights from Nationwide Surveys and Emerging Ethical Challenges
- The Challenge of Peritoneal Vaginoplasty in Transgender Women: Review Literature and Personal Perspectives
- Algorithmic Paternalism: Autonomy Versus Automation
- Dermatoscopy in Gorlin Syndrome: Avoiding the Disfigurement in Patients
- How Artificial Intelligence is Ushering in a New Era of Innovation in General and Plastic Surgery: A Short Communication