Exploring Adverse Events of Remdesivir in Covid-19 Patients: A Comprehensive Global Analysis
Background: The emergence of COVID-19, stemming from SARS-CoV-2, has triggered a global pandemic, urging rapid therapeutic interventions. Remdesivir, a nucleotide analog prodrug, garnered attention for its potential against COVID-19 due to in vitro efficacy against coronaviruses. This study reviews Remdesivir’s adverse effects in COVID-19 patients. Methodology: While Remdesivir shows promise, recent studies raise efficacy concerns. Adverse drug event (ADE) documentation is vital due to limited pre-pandemic ADE data. WHO VigiBase® analysis (2015-2020) and COVID-19 ADE studies were undertaken, focusing on age, severity, region, and organ impact. 1086 ADEs emerged from 439 case reports by July 19, 2020, in VigiBase®, reducing to 1004 after duplicates were removed. ADEs primarily related to COVID-19 patients (92.5%), notably from the Americas (67.7%). Mainly in males above 45, ADEs were serious (82.5%). Key ADEs encompassed elevated hepatic enzymes (32.1%), renal damage (14.4%), increased creatinine levels (11.2%), and respiratory failure (6.4%). Conclusion: Liver and kidney function deterioration emerged as frequent ADEs, underscoring the need for vigilance during Remdesivir treatment. These findings align with regulatory documents. In sum, COVID-19 has prompted swift therapeutic responses, with Remdesivir being explored as a potential treatment. This study sheds light on associated ADEs, highlighting the importance of monitoring and informed decision-making.
Introduction
The COVID-19 pandemic has spurred a quest for efficacious antiviral remedies. Originally formulated to combat Ebola virus disease, Remdesivir has exhibited potential in mitigating COVID-19 symptoms by impeding viral RNA polymerase. Nonetheless, its utilization in clinical settings has elicited apprehensions regarding potential adverse effects. SARS-CoV-2, a positive-sense, single- stranded RNA virus measuring approximately 30 kilobases in length, possesses a nucleocapsid. It gains entry into infected cells through endocytosis or membrane fusion, potentially leading to respiratory and intestinal disorders, as well as affecting the liver and nervous system in various species, including humans and certain animals [1]. COVID-19 stands as an infectious ailment triggered by SARS-CoV-2, a coronavirus unveiled in December 2019, which has sparked a global pandemic of monumental proportions. The transmission of this disease primarily occurs through the inhalation of droplets released during coughing, sneezing, or conversations with individuals carrying the infection [2, 3, 4, 5]. The coronavirus was initially comprehensively elucidated during the 1960s. Its nomenclature stems from the discernible corona, resembling a “crown,” composed of sugary proteins enveloping the entire structure. Within this family, various genus-species combinations exist: Alpha-coronavirus and Beta-coronavirus, impacting mammals exclusively, including bats, pigs, and humans; Gamma-coronavirus, predominantly affecting avian species; and Delta-coronavirus, with the capacity to infect both birds and mammals [6].
Coronaviruses belong to a family of viruses renowned for inducing grave maladies in both mammals and avian species. While certain viral strains are infrequent, others have gained prominence, such as the Wuhan coronavirus (2019-nCoV), as well as those accountable for severe acute respiratory syndrome (SARS) and Middle East Respiratory Syndrome (MERS). These viruses possess the potential to inflict fatalities upon human hosts [7]. The unparalleled circumstances brought about by the Coronavirus Disease 2019 (COVID-19) pandemic have presented unique challenges, stemming from the absence of established therapies and treatment protocols. While the contagion of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is notably high, its resulting infection appears to exhibit a lower degree of severity in terms of morbidity and mortality compared to Severe Acute Respiratory Syndrome (SARS) and Middle East Respiratory Syndrome (MERS) [8].
Consequently, the management of patients varies contingent upon the severity of the disease and mindful evaluation of preexisting medical conditions. Numerous drugs have arisen as potential contenders for treatment, encompassing nucleotide analogs like remdesivir, along with anti- malarials such as chloroquine and hydroxychloroquine [9]. Protease inhibitors, specifically lopinavir/ritonavir, along with interferon-β, have been incorporated into ongoing clinical trials. However, it’s important to note that these treatments are currently not endorsed for use in treatment [9]. Elevated apprehensions have arisen regarding the plausible heightened vulnerability to SARS-CoV-2 among patients under medication regimens, including nonsteroidal anti-inflammatory drugs (NSAIDs) and renin angiotensin aldosterone system (RAAS) antagonists. These medications are implicated in the upregulation of angiotensin-converting enzyme 2 (ACE2), thereby prompting concerns about potential increased susceptibility to the virus [10].
In a more recent study conducted by Beigel, et al. [10], it was revealed that among individuals hospitalized due to severe COVID-19, a 10-day regimen of remdesivir led to a swifter recovery period. The outcomes were particularly noteworthy for patients requiring oxygen support. The mortality rate observed with remdesivir was 7.1%, as opposed to 11.9% with the placebo, although this disparity did not reach statistical significance [11]. In a more recent study conducted by Goldman et al. (2020), it was demonstrated that there was no notable disparity in outcomes among patients with severe COVID-19 who were administered either a 5 or 10-day regimen of remdesivir. It’s important to note that this study lacked a placebo control group [12]. In light of the recent interim analysis from the WHO Solidarity study, it has been indicated that remdesivir does not appear to offer any discernible advantages in terms of diminishing the need for ventilation initiation, shortening hospitalization duration, or reducing mortality rates [13, 14].
Given these developments, it remains crucial to persist in gathering safety information concerning the repurposed utilization of remdesivir for treating individuals with COVID-19. Simultaneously, it is imperative to accumulate further data to assess its efficacy among patients grappling with moderate to severe disease [15]. This stems from reports highlighting significant adverse effects associated with remdesivir, notably including instances of hepatotoxicity or liver damage [16]. The capacity of SARS- CoV-2 to induce changes in hepatic function introduces a specific concern when considering the prescription of remdesivir [15, 16, 17]. This necessity extends to encompass routine clinical care as well as randomized studies. Notably, the study by Beigel, et al. [10] employed significant exclusion criteria, such as individuals with AST or ALT (Alanine Aminotransferase) levels exceeding five times the upper limit of normal (ULN), along with those experiencing impaired renal function [11, 12, 13, 14, 15, 16, 17].
The United Kingdom’s prescribing guidance, formulated in collaboration with NHS England and the devolved administrations, established analogous exclusion criteria involving ALT levels and impaired renal function. The guidelines stipulated that treatment should be discontinued if there was a rise in ALT accompanied by indications of liver inflammation, an elevation in alkaline phosphatase, conjugated bilirubin, or international-normalized ratios. Additionally, the European Medicines Agency granted authorization for compassionate use of remdesivir, aligning with these considerations [18, 19]. The prevailing adverse drug reactions (ADRs) observed in these studies, as well as in a controlled trial involving patients with Ebola virus disease, encompassed occurrences of phlebitis, constipation, headaches, ecchymosis (bruising), nausea, pain in extremities, and a temporary elevation in liver enzyme levels [19, 20]. Preceding these instances, remdesivir was noted to induce a reversible escalation in liver enzyme levels among healthy volunteers during the preliminary stages of drug development studies.
Notably, a similar elevation in liver enzymes was also observed in patients who received remdesivir through the compassionate use program [21]. As a result, we recognized the urgency of promptly assessing the present status of adverse drug events (ADEs) linked to remdesivir, including those originating from published studies involving COVID-19 patients. This becomes particularly pertinent as even previously rare ADEs assume significance for hospitalized COVID-19 patients, particularly those requiring oxygen support. Furthermore, the potential for drug-disease interactions may diverge due to variations in populations, with COVID-19 patients generally being older and having co- existing medical conditions. In light of these considerations, it becomes imperative to meticulously delineate specific ADEs stemming from the repurposed use of remdesivir for COVID-19. These findings can subsequently offer guidance to physicians and other healthcare professionals in effectively managing COVID-19 patients who are administered remdesivir, thus addressing some of the contentious aspects surrounding its application. This endeavor aligns with the encouragement for physicians across the United States and beyond to report any adverse events related to remdesivir to the FDA’s MedWatch Safety Information and Adverse Event Reporting Program. This proactive approach aims to accumulate a wealth of safety data, particularly as further clinical trials remain indispensable for a comprehensive assessment of remdesivir’s role in managing COVID-19 patients [22, 23].
Remdesivir is an antiviral medication belonging to the nucleoside analogue family, formulated by Gilead Pharmaceuticals initially for the treatment of Ebola and Marburg virus infections. Its antiviral characteristics have also led to its application against other single-stranded RNA viruses, encompassing respiratory syncytial virus, blood virus, lasagna virus, NIPA virus, Hendra virus, as well as the coronavirus family, which includes notable members like Middle East Respiratory Syndrome (MERS) and Severe Acute Respiratory Syndrome (SARS) coronaviruses [24]. Indeed, remdesivir has demonstrated success in treating COVID-19 in numerous cases, garnering substantial attention and research efforts. Its efficacy in mitigating the effects of the disease has prompted extensive studies and investigations aimed at better understanding its potential benefits and limitations in the context of COVID-19 treatment [24]. Remdesivir is a prodrug that is metabolized in the body to its active form, GS-441524. This active form acts as an adenosine analogue, disrupting the function of the RNA- dependent RNA polymerase enzyme, which is crucial for the replication of the virus. Remdesivir interferes with the virus’s ability to replicate by inhibiting the RNA polymerase, which is responsible for copying the virus’s genetic material. This disruption ultimately impedes the virus’s ability to reproduce and proliferate.
The precise mechanism by which remdesivir affects the virus’s RNA chain is not fully understood, and whether it terminates the RNA chain or leads to specific mutations is a subject of ongoing research and investigation. Nonetheless, its interference with the replication process has demonstrated efficacy in reducing virus production and replication, contributing to its potential as a treatment for COVID-19 [24]. Similar to any other medication, Remdesivir has been reported to have associated adverse effects (AEs), some of which are linked to its usage. The prevalent side effects observed in Remdesivir studies for COVID-19 consist of respiratory failure and organ dysfunction. These effects encompass conditions such as decreased levels of albumin, potassium, red blood cells, and platelets (which contribute to clotting). Additionally, an observable yellow discoloration of the skin has also been noted [25]. Reported adverse effects encompass gastrointestinal disturbances, elevated levels of transaminases in the bloodstream (liver enzymes), as well as reactions at the injection site [26].
Additional potential side effects associated with remdesivir administration include injection-related reactions. These reactions, which may manifest during or near the time of remdesivir injection, have been noted to entail symptoms such as low blood pressure, nausea, vomiting, sweating, and chills [26]. Increased levels of liver enzymes, as indicated by abnormal liver blood test results, have been documented. People who have received remdesivir have demonstrated elevated levels of liver enzymes, potentially indicating inflammation or harm to liver cells [26]. Our study was designed to assess the efficacy of the antiviral medication remdesivir in treating individuals with novel COVID‐19 infection, both in cases accompanied by diabetes mellitus and those without. While the discovery of COVID-19 vaccines has undoubtedly overcome several hurdles in the realm of treatment, the need for a potent and rapid response through a dedicated therapeutic agent remains pertinent.
Methodology
We conducted a comprehensive systematic review of the existing literature by utilizing electronic databases such as PubMed, Embase, and Cochrane Library. Our aim was to identify pertinent studies that provided insights into the side effects of Remdesivir in patients afflicted with COVID-19. The scope of our review encompassed studies published from the onset of the pandemic up to the current date. VigiBase®, a comprehensive database, houses an extensive collection of individual case safety reports (ICSRs) documenting adverse events. These reports are gathered from national pharmacovigilance centers spanning across more than 130 countries [27, 28, 29]. An ICSR denotes an anonymized report detailing a solitary individual (patient) administered a suspected drug and encountering one or more adverse drug events (ADEs).
Within VigiBase®, these reports are systematically organized, encompassing a range of information, including patient demographics, drug details (route of administration, purpose of use, start and end dates), suspected ADE particulars (onset date, outcome, seriousness, and causality assessment), along with administrative data (report type and source). For enhanced categorization, medications are coded in alignment with the WHO Drug Dictionary Enhanced, which encompasses the ATC (Anatomical Therapeutic Chemical) classification system [30]. The MedDRA dictionary follows a hierarchical organization structured by System Organ Class (SOC), which is further subdivided into Preferred Terms (PT) and then into the most specific level known as Lowest-Level Terms (LLT).
Remedesivir
Remdesivir functions as a nucleotide analogue, seamlessly integrating itself into the viral RNA chain, ultimately leading to premature termination of the chain [31]. This experimental drug has exhibited antiviral effectiveness against various RNA viruses, including Ebola, SARS, and MERS, both in vitro and in nonhuman primate studies [31, 32]. A recent case report highlighted the treatment of a COVID- 19 patient in the US with remdesivir under compassionate use circumstances. The patient’s clinical condition had been deteriorating, but remarkably improved following the administration of remdesivir [33]. Just 48 hours after commencing treatment, the patient’s need for supplemental oxygen ceased, and he was left with only minor symptoms – a dry cough and mild rhinorrhea [33]. Another case was documented where remdesivir was administered, resulting in the patient’s successful recovery [34]. While the available data are currently confined to case reports, remdesivir emerges as a promising contender for therapy.
Notably, non-human primates afflicted with MERS- CoV and treated using a combination of remdesivir and interferon-β displayed notable enhancements in pulmonary function alongside reduced lung viral loads. This positive outcome contrasts with those treated with lopinavir/ ritonavir and interferon-β [35]. Remdesivir is typically well-tolerated and has not been strongly associated with a substantial number of side effects. However, the potential risks can differ based on individual circumstances. Among the most frequently encountered side effects is nausea. Additionally, it’s not uncommon for lab results to show heightened liver enzymes (proteins). It’s important to note that these liver effects usually manifest as mild, often without symptoms, and tend to resolve spontaneously.
Pharmacologically, remdesivir has been ingeniously formulated to facilitate the intracellular delivery of the monophosphate nucleoside analog GS-441524. Currently, remdesivir is extensively administered intravenously as a straightforward adenosine nucleotide prodrug. Functionally, it combines with the viral gene-associated RNA polymerase, effectively curbing viral replication by diminishing RNA synthesis. Impressively, remdesivir exhibits inhibitory properties against SARS-CoV-2 activity in vitro. In a SARS- CoV-2 model, remdesivir treatment was initiated post- vaccination, yielding promising results. The subjects treated with remdesivir displayed diminished viral infiltration in the lungs and showcased reduced harm in comparison to the control group. This underscores the potential therapeutic value of remdesivir in combatting SARS-CoV-2 infection [36, 37].
The angiotensin-converting enzyme-2 (ACE-2), predominantly located in the lungs, heart, blood vessels, and select other cells, serves as a principal gateway receptor for SARS-CoV-2 within human cells. Symptomatic manifestation in coronavirus patients typically occurs within 5 to 6 days post- infection. Certain individuals, characterized by factors such as advanced age and male gender, face an elevated risk of contracting COVID-19. This risk is often accompanied by various clinical presentations, including cardiovascular diseases (CVD) and diabetes mellitus. A preceding study underscored the pivotal role of concealed CVD and diabetes mellitus as fundamental complications influencing the progression of COVID-19 infection, particularly among patients necessitating care in emergency units [38].
Data and Analysis
This study encompassed an analysis of all suspected adverse events associated with remdesivir, as reported to VigiBase®. Each entry within VigiBase® pertained to a solitary individual who might have experienced one or multiple adverse events concurrently. Consequently, the reported count of adverse events often surpasses the actual number of patients for whom case reports were generated. The adverse events were systematically categorized using the Medical Dictionary for Regulatory Authorities (MedDRA), and this classification was conducted at both the System Organ Classification (SOC) level and the individual Preferred Term (PT) level [39]. The SOC serves as a comprehensive grouping of distinct adverse events, where preferred terms are categorized into various headings based on factors such as etiology (e.g., infections and infestations), manifestation site (e.g., hepatobiliary disorders), purpose (e.g., surgical and medical procedures), product issues, and social circumstances [40].
The examination of these reports entailed a thorough analysis considering several factors. These factors encompassed age, gender, geographical region of reporting, classification at the System Organ Classification (SOC) level, as well as at the individual Preferred Term (PT) level for adverse events. Additionally, the seriousness of the adverse events was evaluated, alongside outcomes, dechallenge- rechallenge actions, and ultimate outcomes. In relation to age, a specific division was established, focusing on individuals aged below and above 64 years. This demarcation was chosen as COVID-19-associated mortality tends to escalate with advancing age. The assessment of seriousness relied on the ICH E2B criteria, which classifies adverse events as serious if they lead to conditions such as death, life-threatening situations, necessitating hospitalization, or resulting in an extended hospital stay leading to disability or congenital anomalies [41, 42].
The database provided to us did not offer a clear delineation of reported deaths. Consequently, we sought clarification on this matter directly from the database administrators. In accordance with the guidance provided by them, instances of death reported under any of the headings including ‘seriousness’, ‘outcome’, and ‘preferred term’ were taken into account for the purpose of calculating fatalities. In addition to cataloging adverse drug events (ADEs) observed in VigiBase® associated with remdesivir, our efforts extended to encompass ADEs detailed in published studies. This comprehensive approach is vital due to a notable apprehension often observed with new medications. Clinical trials typically involve a carefully curated patient group, often comprising individuals who are comparatively younger and possess fewer coexisting medical conditions compared to those encountered in routine clinical practice. This distinction raises concerns about the generalizability of trial results to the broader patient population [43, 44].
Results
We will first summarize reported ADEs in the published studies as well as summaries ADEs reported to VigiBase®.
Reported ADEs Summary
Table 1 this summary encapsulates findings derived from multiple sources, encompassing published studies as well as submissions to diverse regulatory bodies. The objective is to provide a comprehensive overview of the gathered information, allowing for a holistic assessment of the subject matter.
| Categories of Patients | Findings | |
|---|---|---|
| Goldman, et al. [12] | 397 patients with severe COVID-19 randomized to either 5 days treatment (200 patients) or 10 days treatment (197 patients) | 70% of patients in the 5-day group and 74% in the 10-day group experienced ADEs, with 21% in the 5-day group and 35% in the 10-day group experiencing serious ADEs The most common ADEs were: Nausea – 10% in the 5-day group and 9% in the 10-day group Acute respiratory failure – 6% in the 5-day group and 11% in the 10-day group Increased ALT – 6% in the 5-day group and 8% in the 10-day group Constipation – 7% in both groups 4% in the 5-day group discontinued treatment owing to ADEs versus 10% in the 10-day group |
| Beigel, et al. [11] | 1062 hospitalized patients with COVID-19 randomized either to remdesivir or placebo | Serious ADEs occurred in 24.6% of patients in the remdesivir group vs. 31.6% in the placebo group 8.8% of patients in the remdesivir group had serious respiratory failure AEs including acute respiratory failure and the need for endotracheal intubation. No deaths were considered by the investigators to be related to treatment assignment The most common nonserious ADEs occurring in at least 5% of all patients included decreased glomerular filtration rate, decreased haemoglobin levels and lymphocyte counts, respiratory failure, anaemia, pyrexia, and hyperglycaemia as well as increased blood creatinine levels and blood glucose levels. The incidence of AEs was generally similar between the remdesivir and placebo groups |
| Spinner, et al. [45] | Study of 596 patients with moderate COVID-19 randomized to either 5 or 10 days of treatment with remdesivir vs. standard care | AEs were experienced by 51% of patients in the 5-day remdesivir group vs. 59% in the 10-day remdesivir group and 47% in the standard care group Differences between the 5-day remdesivir group and standard care was not statistically significant but the difference between the 10-day remdesivir group and standard care were AEs more common in the remdesivir groups vs. standard care included nausea (10% 5-day and 9% 10-day groups), hypokalaemia (5% 5-day and 7% 10-day), and headaches (5% both groups). Diarrhea also occurred but 6% in 5-day group, 5% in 10-day group and 7% in standard care group Serious AEs were less common in the remdesivir groups (5% in both) vs. standard care (9%) |
| Studied 208 patients from 11 Finnish Hospitals. | Exertional dyspnea (at least a need to walk more slowly than usual) occurred in 5% in remdesivir and in 8% in SoC (RR 0.61, 95% CI 0.20–1.85; absolute difference –3.3%, 95% CI –12–4.4%). Median EQ-VAS was 75.5 (IQR 67.8–85.0) in the remdesivir and 80 (IQR 67.5–86.5) in SoC group (ordered logistic regression or 0.83, 95% CI 0.49–1.40) | |
| Mulangu, et al. [20] | Randomized trial of 681 patients testing positive for Ebola virus the on reverse- transcriptase-polymerase-chain-reaction assay | 29 serious AEs were determined by trial investigators to be potentially related to the trial drugs After adjudication by an independent panel, 4 events in 3 patients, all resulting in death, were possibly related to trial drugs. This included one patient in the remdesivir group who had hypotension that resulted in cessation of a loading dose of remdesivir followed rapidly by cardiac arrest – however, could not be readily distinguishable from underlying Ebola Typically, the safety profile was generally consistent with Phase 1 data |
Table 1: summarizes the findings from published data. ADE: Adverse Drug Event ; RR: Relative Risk; SoC: Standard of care CI: Card
Summary of Findings from Vigibase®
A total of 1087 adverse drug events (ADEs) were documented from 439 case information reports. It’s important to note that each case information report corresponds to an individual who received remdesivir. After eliminating duplicate ADEs that were reported using different terminologies within each case information report, a total of 1004 unique ADEs were available for analysis, as outlined in Table 2. Considering that multiple ADEs were frequently reported for each patient, the total count of ADEs was notably higher than the number of individuals. Overall, the analysis revealed that 1004 ADEs originated from 439 individuals, resulting in an average of 2.28 ADEs per person. Geographically, the distribution of individuals was as follows: 145 (33%) from Europe, 288 (65%) from the Americas, and 6 (1.3%) from the western Pacific region. In terms of gender, 267 (61%) were males, 163 (37.1%) were females, and gender was not reported for 9 (2%) individuals.
| Parameter | Categories | Frequency (%) |
|---|---|---|
| Age | <18 years | 2.1 |
| 18-64 years | 46.7 | |
| >65 years | 41.5 | |
| Not Reported | 9.7 | |
| Gender | Male | 58.9 |
| Female | 39.7 | |
| Not Reported | 1.4 | |
| Seriousness of AE | Serious | 82.5 |
| Non-serious | 17.5 | |
| Route of Administration | Intravenous | 80.2 |
| Iontophoresis | 0.8 | |
| Respiratory | 0.3 | |
| Other | 0.1 | |
| Unknown | 5.3 | |
| Not Reported | 13.4 | |
| Indications | Covid-19 treatment | 92.6 |
| Acinetobacter infection | 0.2 | |
| ARDS | 0.1 | |
| Drug use for unknown indication | 0.5 | |
| Not reported | 6.5 | |
| Dose not changed | 12.2 | |
| Drug withdrawn | 22 | |
| Not applicable | 2.5 | |
| Unknown | 3.5 | |
| Not reported | 59.9 | |
| Fatal | 5.7 | |
| No effect observed | 12 | |
| Reaction abated | 13.2 | |
| Unknown effect | 9.3 | |
| Not reported | 60 | |
| Rechallenge | 13.2 | |
| Not Reported | 86.8 | |
| Unknown effect | 10.6 | |
| No recurrence | 2.7 | |
| Not reported | 86.8 | |
| Fatal | 5.8 | |
| Not recovered/not resolved | 12.2 | |
| Recovered/resolved | 10.1 | |
| Recovered/resolved with squeal | 0.1 | |
| Recovering/resolving | 3 | |
| Unknown | 9.7 | |
| Not Reported | 59.7 |
Table 2: Summarization of ADR reported in VigiBase®. ® For registered website % out of 100 Significantly, a substantial portion o
Table 2: Summarization of ADR reported in VigiBase®. ® For registered website % out of 100 Significantly, a substantial portion of the reported ADEs, amounting to 680 (67.7%), stemmed from individuals in the Americas. Table 2 encapsulates the attributes of the 1004 unique adverse drug events (ADEs) that were recorded in the WHO database. These ADEs originated from 439 distinct individuals. Notably, approximately half of these ADEs were documented within the age range of 18 to 64 years. In terms of gender distribution, ADEs were more frequently reported in males, accounting for 58.9% of the total. Moreover, a notable proportion of the reported ADEs were classified as serious. An overwhelming 92.6% of the ADEs were associated with the use of remdesivir for the treatment of COVID-19 infection. Furthermore, a fraction of these ADEs, approximately 5.8%, resulted in a fatal outcome. Assessment of causality was conducted based on parameters such as dechallenge action, dechallenge outcome, rechallenge action, and rechallenge outcome, but such comprehensive data was only available for a minority of the ADEs. Unfortunately, due to the incomplete nature of the available data, a thorough evaluation of causality could not be feasibly accomplished.
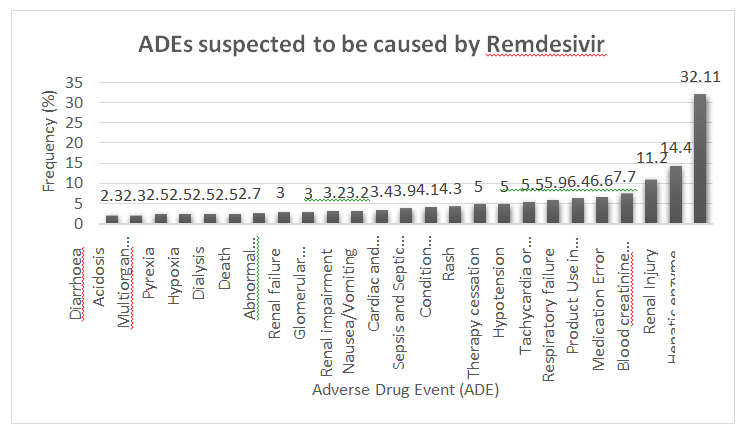
The prevailing adverse drug event (ADE) attributed to remdesivir was an elevation in liver enzymes. This occurrence constituted the most frequent ADE, with approximately one- third of the patients administered remdesivir reporting such an effect, as detailed in Figure 1. Unfortunately, the specific liver enzyme that experienced the highest increase could not be accurately determined due to data limitations in many of the case information reports.
The patient distribution across the two groups was carefully balanced with respect to disease characteristics. Among the participants, 48% were identified as diabetic individuals, of whom 42% exhibited comorbid hypertension. In contrast, the nondiabetic cohort constituted 52% of the patients, with 30% of them presenting hypertension. Moreover, gender distribution within both groups demonstrated a near parity between male and female participants. Furthermore, the patient categorization was extended to encompass oxygen requirements, revealing a consistent ratio between diabetic and nondiabetic patients. These findings are systematically presented in Table 3 for reference.
| Diabetic Patients (48%) | Nondiabetic Patients (52%) | |
|---|---|---|
| Age | 18-58 | 20-62 |
| Male | 64% | 65% |
| Female | 36% | 35% |
| Hypertension | 42% | 30% |
| Not requiring oxygen | 13% | 12% |
| Requiring oxygen | 39% | 41% |
| Median time from symptoms onset to randomization (days) | 6-12 | 6-12 |
Table 3: Randomized studies of remdesivir in COVID‐19 patients.
Kidney-related ADEs were also observed with notable frequency. Reports encompassed renal injury (14.4%), elevated blood creatinine levels (11.2%), renal impairment, and a reduction in glomerular filtration rate (3.2%).
Additionally, respiratory failure, arrhythmia, hypotension, and rash were among the commonly reported ADEs, as outlined in Table No. 2.
Discussion
We posit that our study stands as a pioneering endeavor in the aftermath of the COVID-19 pandemic, aimed at comprehensively evaluating the occurrence and scope of adverse drug events (ADEs) associated with remdesivir. This research delves into the World Health Organization (WHO) database, following the repurposing of remdesivir for COVID-19 treatment, and extends its analysis beyond the insights presented in previously published studies (as detailed in Table No. 1). Our undertaking assumes significance due to the prevailing uncertainties and debates surrounding therapeutic approaches for COVID-19 patients, which extend to the utilization of remdesivir. Furthermore, it acknowledges the distinctiveness inherent in the COVID-19 patient population, diverging from the demographics of individuals conventionally administered remdesivir prior to the emergence of the pandemic [13, 45].
An intriguing observation emerged from our analysis, revealing that a predominant share of adverse drug events (ADEs) were documented among male individuals and those aged 45 years or above, as detailed in Table No. 2. Notably, the focal point of these occurrences was predominantly concentrated within the American continent, with health professionals being the primary contributors to the spontaneous reporting, as depicted in the same table. This pattern seems to be a direct consequence of several factors that interplay. The bulk of ADEs can be attributed to their involvement in the management of patients afflicted with COVID-19, which constituted a significant proportion (92.6%). This correlation gains further insight from influential sources, such as the prominent NIH study advocating remdesivir usage, coupled with the endorsement granted by the US FDA. Additionally, the strategic stockpiling efforts by the US government, potentially at the expense of supply availability in other nations during the initial stages, could also account for these trends [46, 47].
Nevertheless, it is imperative to emphasize that our conclusions should be approached with caution, as additional research is warranted to establish definitive assertions. It is crucial to acknowledge that certain reservations persist, particularly regarding the comprehensiveness of adverse drug event (ADE) reporting across various nations. This concern is notably pronounced in lower and middle income countries (LMICs) in recent times, and this potential disparity could potentially influence the volume of reported cases beyond the confines of Europe and the United States. In essence, while our findings offer valuable insights, the broader context of global ADE reporting dynamics, especially in regions with resource limitations, must be taken into consideration before drawing final conclusions. Subsequent investigations are vital to augment our understanding and to corroborate or refine the patterns we have delineated [48, 49, 50].
Elevated hepatic enzymes represent a notable apprehension associated with the usage of remdesivir. In response to this concern, the official product information for remdesivir outlines a set of recommendations aimed at managing this potential risk. Specifically, the guidance advises that prior to initiating remdesivir treatment, comprehensive liver function tests should be conducted. Furthermore, the product information underscores the importance of exercising caution in administering remdesivir to patients whose alanine aminotransferase (ALT) levels exceed five times the standard reference range. This caution is particularly relevant in cases where ALT elevation is accompanied by discernible indications of liver inflammation or concurrent elevation of other liver enzymes. In essence, these guidelines underscore a proactive approach to patient safety, ensuring thorough monitoring and appropriate decision-making to mitigate the potential adverse effects on hepatic function that may arise with the administration of remdesivir [21].
Henceforth, we hold the view that diligent vigilance over a patient’s liver function throughout the course of remdesivir treatment remains a pivotal consideration. This stance aligns harmoniously with the recommendations outlined in the product summary information, underlining the necessity for physicians to remain steadfast in monitoring hepatic markers. Nevertheless, it is worth noting that our present knowledge base lacks explicit directives regarding the necessity for dose adjustments of remdesivir in the context of patients with hepatic impairment. In this regard, the decision-making process inevitably rests with the attending physicians, who must judiciously weigh the potential risks against the anticipated benefits. The pivotal task before physicians, therefore, lies in orchestrating a finely balanced evaluation of the risk-benefit calculus. In the absence of specific guidelines, the medical community’s prudence shall guide them in determining whether to initiate or sustain the use of remdesivir within the subset of patients displaying hepatic impairment. This deliberative approach, rooted in clinical acumen, encapsulates the essence of medical practice as a blend of science and art.
While the majority of side effects stemming from remdesivir administration are typically manageable, a subset of more severe adverse events has been documented, warranting heightened attention. Notably, reports have surfaced detailing instances of acute kidney injury, hypotension, and respiratory failure. These occurrences seem to be more prevalent among patients harboring underlying comorbidities. It’s worth highlighting that discerning between the direct impact of remdesivir and the natural course of severe COVID-19 disease presents a complex challenge. This intricacy underscores the need for a nuanced approach in evaluating the interplay between these factors. The extensive landscape of clinical trials and case reports has substantiated a gamut of side effects linked to remdesivir administration. These encompass a spectrum of manifestations, ranging from nausea, vomiting, and diarrhea to elevated liver enzymes and rash. It is imperative to acknowledge that this list is not exhaustive. Importantly, the majority of these side effects tend to be of mild to moderate intensity and often exhibit a self-resolving trajectory. This characteristic aligns with the reassuring observation that, in many instances, these adverse effects alleviate spontaneously without necessitating substantial medical intervention.
While no definitive therapies targeting SARS-CoV-2 are presently accessible, a number of pharmaceuticals have emerged as plausible contenders for treatment. Notably, given its cost-effectiveness, widespread availability, and the absence of viable alternatives, a regimen involving both hydroxychloroquine and azithromycin is frequently contemplated for managing hospitalized individuals grappling with moderate to severe COVID-19. However, it’s imperative to underscore that the adoption of this anti- malarial approach for COVID-19 is rooted in the findings of a solitary study. This study is characterized by its reliance on a relatively limited sample size, the absence of randomized control groups, and notable attrition within the treatment arm. As such, while the utilization of hydroxychloroquine and azithromycin has garnered attention, the validity and generalizability of this approach warrant circumspection. Prudent clinical decision-making necessitates a comprehensive appreciation of the current limitations in the available evidence, prompting a judicious evaluation of the potential benefits and risks associated with this therapeutic strategy [51].
The efficacy of this treatment approach remains uncertain, underscoring the need to weigh the potential for significant adverse effects before embarking on therapy with these drugs. Within the realm of antiviral options, remdesivir emerges as a promising contender, with prospects for wider availability in the coming weeks. Past successes in passive immunization have kindled hope, yet the precise efficacy of convalescent plasma in treating critically ill COVID-19 patients remains largely uncharted. Many institutions are beginning to embrace this treatment avenue, capitalizing on the increasing pool of individuals convalescing from the disease and the subsequent availability of convalescent plasma. Notably, the utilization of medications such as ibuprofen and RAAS antagonists in the context of COVID-19 sparked significant concerns. However, current guidelines stipulate the admissibility of ibuprofen and discourage the discontinuation of ACE inhibitors and ARBs.
The dynamic landscape of treatment mandates vigilant recalibration in response to emerging data. It is imperative to discourage unwarranted prescription practices and the unnecessary accumulation of medications. Simultaneously, parallel endeavours are laser focused on vaccine development, stringent infection control measures, and optimizing respiratory and supportive care. In summary, the path forward necessitates a balance between embracing evolving treatment insights and fostering a holistic approach, encompassing vaccine advancement, robust infection containment strategies, and comprehensive patient care.
Conclusion
This study aimed to conduct a comprehensive descriptive analysis of adverse drug events (ADEs) reported thus far concerning remdesivir. This effort seeks to contribute additional insights to the existing safety information derived from published clinical trials involving COVID-19 patients, thus addressing potential concerns. Notably, the analysis underscores the prominence of certain ADEs, particularly the elevation of liver enzymes and those stemming from kidney injury. Remarkably, these findings are congruent with the guidance provided by the FDA in the product information for remdesivir. These results underscore the imperative for heightened vigilance in monitoring liver enzyme levels throughout the course of treatment. This monitoring approach should be fortified based on existing recommendations, potentially extending to dose adjustments when indicated. Additionally, prudently assessing renal function prior to and during remdesivir treatment is advocated.
As our understanding of remdesivir’s safety profile continues to burgeon, the regulatory authorities have a pivotal role in furnishing augmented guidance as new insights emerge. This includes delineating potential remdesivir dosages tailored to COVID-19 patients grappling with pre-existing hepatic impairment or compromised renal function. While remdesivir holds promise as a therapeutic intervention for COVID-19 patients, its usage is intertwined with a gamut of side effects, encompassing mild gastrointestinal symptoms as well as more consequential complications. In light of this evolving comprehension of remdesivir’s safety landscape, the confluence of ongoing surveillance and comprehensive research is indispensable. These efforts coalesce to furnish clinicians with a robust compass, enabling informed decisions regarding remdesivir administration across diverse patient demographics.
Decleration
Ethics Approval and Consent to Participate
Ethical approval not required.
Consent for Publication
All authors have consent to publish this manuscript.
Availability of Data and Material
Access to these resources will enable fellow researchers to validate our findings, replicate the experiments, and extend the study’s scope. We encourage readers to use these materials responsibly and provide appropriate attribution.
Competing Interests
The authors declare that they have no competing interests.
Funding
No specific grant was received for this study.
Acknowledgements
The completion of this research would not have been possible without the collective efforts and encouragement of these individuals and organizations. While we take responsibility for any errors or omissions, their contributions have undoubtedly enriched the outcome of this study.
References
-
Cascella M, Rajnik M, Cuomo A, Dulebohn SC, Di NR (2020) Features evaluation and treatment coronavirus COVID 19. Statpearls, pp: 1-17.
-
Aria A, Forouharnejad K, Mortazavi M, Omidi A, Askari M, et al. (2020) COVID 19 with neurological symptoms, rhabdomyolysis and brain death a case report. Am J Clin Exp Immunol 9: 114.
-
Yuki K, Fujiogi M, Koutsogiannaki S (2020) COVID-19 pathophysiology a review. Clin Immunol 215: 108427.
-
Chen Y, Guo Y, Pan Y, Zhao ZJ (2020) Structure analysis of the receptor binding of 2019-nCoV. Biochem Biophys Res Commun 525(1): 135-140.
-
Stobbe M (2020) Wuhan coronavirus 2019 nCoV naming a new disease. Health coronavirus.
-
Mayur SB, Someshwar D, Mankar PV, Malvade PV, Waghule GS (2020) A Novel Coronavirus 2019 Ncov Associated With Human Respiratory Diseases A Review. World Journal of Pharmaceutical Research 9(5): 2482- 2503.
-
Guo YR, Cao QD, Hong ZS (2020) The origin transmission and clinical therapies on coronavirus disease 2019 COVID-19 outbreak an update on the status. Mil Med Res 7(1): 11.
-
Centers for Disease Control and Prevention (2020) Information for clinicians on therapeutic options for COVID-19 patients.
-
Fang L, Karakiulakis G, Roth M (2020) Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection. Lancet Respir Med 8(4): 21.
-
WHO STC (2021) Repurposed antiviral drugs for COVID-19 interim WHO solidarity trial results. N Engl J Med.
-
Beigel JH, Tomashek KM, Dodd LE, Meehta AK, Zingman BS, et al. (2020) Remdesivir for the treatment of Covid-19 final report. N Engl J Med 383: 1813-1826.
-
Goldman JD, Lye DCB, Hui DS, Marks KM, Bruno R, et al. (2020) Remdesivir for 5 or 10 days in patients with severe Covid 19. N Engl J Med 383: 1827-1837.
-
Dyer O (2020) Covid-19 remdesivir has little or no impact on survival WHO trial shows. BMJ 371: m4057.
-
Jorgensen SCJ, Kebriaei R, Dresser LD (2020) Remdesivir review of pharmacology pre clinical data and emerging clinical experience for COVID-19. Pharmacotherapy 40(7): 659-671.
-
Lam S, Lombardi A, Ouanounou A (2020) COVID 19 A review of the proposed pharmacological treatments. Eur J Pharmacol 886: 173451.
-
Frega G, Palloni A, Di PG, Saccoccio G, Alessandro R, et al. (2020) Challenges in repurposing drugs in COVID-19 pandemic Debating on potential new refinements. Front Pharmacol 11: 559996.
-
NHS UK (2022) Interim clinical commissioning policy remdesivir for patients hospitalised with COVID-19.
-
EMA (2020) Summary on compassionate use remdesivir gilead international non-proprietary name remdesivir. Science medicines health, pp: 2-45.
-
US FDA (2020) Fact sheet for health care providers emergency use authorization eua of veklury remdesivir.
-
Mulangu S, Dodd LE, Davey RT, Mbaya OT, Proschan M, et al. (2019) A randomized controlled trial of ebola virus disease therapeutics. N Engl J Med 381(24): 2293-2303.
-
Mc CEK, Angus DC (2020) Efficacy of remdesivir in COVID-19. Jama 324(11): 1041-1042.
-
Clinical Oncology News (2020) FDA warns of remdesivir drug interaction.
-
Yang CJ, Wei YJ, Chang HL, Chang PY, Tsai CC, et al. (2021) Remdesivir use in the coronavirus disease 2019 pandemic: a minireview. J Microbiol Immunol Infect 54: 27-36.
-
Fan Q, Zhang B, Ma J, Zhang S (2020) Safety profile of the antiviral drug remdesivir an update. Biomed Pharmacother 130: 110532.
-
Dolladille C, Ederhy S, Sassier M (2020) immune checkpoint inhibitor rechallenge after immune related adverse events in patients with cancer. JAMA Oncol 6(6): 1-7.
-
Vollmer O, Felten R, Mertz P, Bénédicte LV, Joe ES (2020) Characterization of auto immune hepatitis associated with the use of anti TNFα agents: an analysis of 389 cases in VigiBase. Autoimmun Rev 19(3): 102460.
-
Chrétien B, Lelong BV, Chantepie S, Sassier M, Bertho M, et al. (2021) Haematologic malignancies associated with clozapine v all other antipsychotic agents a pharmacovigilance study in VigiBase. Psychol Med 51(9): 1459-1466.
-
Sharikabad MN (1982) WHO collaborating centre for drug statistics methodology.
-
Wang M, Cao R, Zhang L, Yang X, Liu J, et al. (2020) Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus 2019-nCoV in vitro. Cell Res 30(3): 269-271.
-
Guo YR, Cao QD, Hong ZS, Tan YY, Chen SD, et al. (2020) The origin transmission and clinical therapies on coronavirus disease 2019 COVID-19 outbreak an update on the status. Mil Med Res 7(1): 11
-
Holshue ML, Debolt C, Lindquist S, Lofy KH, Wiesman J, et al. (2020) First case of 2019 novel coronavirus in the United States. N Engl J Med 382(10): 929-936.
-
Sanville B, Corbett R, Pidcock W, Hardin K, Sebat C, et al. (2020) A community transmitted case of severe acute respiratory distress syndrome due to SARS CoV2 in the United States. Clin Infect Dis 71(16): 2222-2226.
-
Sheahan TP, Sims AC, Leist SR, Schäfer A, Won J, et al. (2020) Comparative therapeutic efficacy of remdesivir and combination lopinavir, ritonavir, and interferon beta against MERS- CoV. Nat Commun 11(1).
-
FDA U (2020) Coronavirus (COVID‐19) update: FDA issues emergency use authorization for potential COVID‐19 treatment. Press Announc, pp: 3‐5.
-
Grein J, Ohmagari N, Shin D, Diaz G, Asperges E, et al. (2020) Compassionate use of remdesivir for patients with severe Covid‐19. N Engl J Med 382(24): 2327‐2336.
-
Cummings MJ, Baldwin MR, Abrams D, Jacobson SD, Meyer BJ, et al. (2020) Epidemiology clinical course and outcomes of critically ill adults with COVID‐19 in New York City a prospective cohort study. Lancet 395(10239): 1763‐1770.
-
Zhou F, Yu T, Du R, Fan G, Liu Y, et al. (2020) Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan China a retrospective cohort study. Lancet 395(10229): 1054-1062.
-
Mikami T, Miyashita H, Yamada T, Harrington M, Steinberg D, et al. (2021) Risk factors for mortality in patients with COVID 19 in New York city. J Gen Intern Med 36(1): 17-26.
-
(2012) Individual case safety reports and VigiBase the vital importance of quality. Uppsala Monitoring Centre, pp: 3-7.
-
Singh J (2015) International conference on harmonisation of technical requirements for registration of pharmaceuticals for human use. J Pharmacol Pharmacother 6(3): 185-187.
-
ICH harmonised tripartite guideline (2021) Maintenance of the ICH guideline on clinical safety data management. Data elements for transmission of individual case safety reports, pp: 1-25.
-
Malmstrom RE, Godman BB, Diogene E, Baumgärtel C, Bennie M, et al. (2013) Dabigatran a case history demonstrating the need for comprehensive approaches to optimize the use of new drugs. Front Pharmacol 4: 39.
-
Joppi R, Cinconze E, Mezzalira L, Pase D, Poggiani C, et al. (2013) Hospitalized patients with atrial fibrillation compared to those included in recent trials on novel oral anticoagulants a population based study. Eur J Intern Med 24(4): 318-323.
-
Spinner CD, Gottlieb RL, Criner GJ, Lopez JRA, Cattelan AM, et al. (2020) Effect of remdesivir vs standard care on clinical status at 11 days in patients with moderate COVID-19 a randomized clinical trial. Jama 324(11): 1048-1057.
-
Boseley. US secures world stock of key Covid-19 drug remdesivir.
-
(2020) Coronavirus COVID-19 update FDA issues emergency use authorization for potential COVID19 treatment. FDA US food and drug administration.
-
Lopez GE, Herdeiro MT, Pineiro LM, Figueiras A, Group G (2015) Effect of an educational intervention to improve adverse drug reaction reporting in physicians a cluster randomized controlled trial. Drug Saf 38(2): 189-196.
-
Haines HM, Meyer JC, Summers RS, Godman BB (2020) Knowledge attitudes and practices of health care professionals towards adverse drug reaction reporting in public sector primary health care facilities in a South African district. Eur J Clin Pharmacol. 76(7): 991-1001.
-
Adisa R, Omitogun TI (2019) Awareness knowledge attitude and practice of adverse drug reaction reporting among health workers and patients in selected primary healthcare centres in Ibadan southwestern Nigeria. BMC Health Serv Res 19(1): 926.
-
Gautret P, Lagiera JC, Parola P, Hoang VT, Meddeb L, et al. (2020) Hydroxychloroquine and azithromycin as a treatment of COVID 19 results of an open label non randomized clinical trial. Int J Antimicrob Agents 56(1): 105949.
-
Nevalainen OPO, Horstia S, Laakkonen S, Rutanen J, Mustonen JMJ, et al. (2022) Effect of remdesivir post hospitalization for COVID-19 infection from the randomized solidarity Finland trial. Nat Commun 13(1): 6152.
- Potential Medicinal Herbs and Secondary Metabolites in Combating Corona Virus
- Monkeypox and its Clinical Implications in Pregnancy
- Pharmacognostical Analysis of the Leaves of Important Nervine Medicinal Plant: Strychnos Nux-Vomica L
- Assessment of Antibacterial Activity of Various Solvent Extracts of Dictyota Dichotoma Against Multidrug Resistant Bacterial Strain
- An Insights of Bioactive Elements on Malignancy: Mechanistic Avenues
- Advances and Future Directions in Pharmacognosy and Chinese Medicine