A Case Report of Discoid Lupus Erythematosus in a Siberian Husky
The discoid lupus erythematosus is a canine autoimmune disease that presents clinically in the form of erythema, depigmentation, scaling, erosions/ulcers and scars on the nasal plane and proximal dorsal region of muzzle. A six-year-old Siberian Husky with a history of pruritus, erythema, ulceration and depigmentation in the nasal region was served at a veterinary service specializing in dermatology. A complete blood count and serum biochemistry, serology for canine leishmaniasis, imaging tests (chest x-ray and abdominal ultrasound), and histopathology were requested. Hematobiochemical tests showed results within normal standards for specie, and serological test for canine leishmaniasis was considered negative. The imaging tests did not accused any changes in canine specie. The histopathological examination revealed the presence of interface dermatitis, irregularly thickened epidermis and inflammatory infiltration at dermo-epidermal junction and interstitial edema. Laboratory and imaging findings together with histopathological results contributed to the diagnostic definition of discoid lupus erythematosus, an autoimmune skin disease rarely present in the routine of small animal veterinary clinics. The results obtained in the study highlight the importance of identifying discoid lupus erythematosus in dogs to ensure correct treatment.
Introduction
The canine discoid lupus erythematosus is a chronic autoimmune disease, classified as a variant form of systemic lupus erythematosus [1]. Discoid lupus erythematosus has as its main characteristics the presence of predominantly nasal dermatitis, associated with microscopic focal dermatitis of the interface, thickening of the basement membrane and superficial lymphocytic and plasmacytic dermatitis [2]. Initial skin lesions consist of erythema, depigmentation and scaling that progress to erosions and ulcerations with atrophy and loss of nasal planar architecture. Crusts may be present if epithelial integrity is damaged. The skin lesions usually affect the nasal plane, but may involve the nostrils [3].
The etiopathogenesis of canine discoid lupus erythematosus is considered multifactorial, involving genetic factors, breakdown of immune tolerance and the participation of environmental triggers [4]. The sun exposure worsens the clinical manifestation of the disease in 50% of cases, since photosensitivity plays an important environmental role in pathogenesis of disease [5]. Therefore, the clinical manifestation of discoid lupus erythematosus may be more severe in the summer or in areas with sunny climates [6], such as Brazil. The exposure to ultraviolet light leads to the development of an inflammatory cascade with production of cytokines that cause apoptosis of skin cells, that contribute to worsening of skin lesions [7].
In some Latin American countries, discoid lupus erythematosus is still commonly underreported and underdiagnosed due to its low incidence and lack of knowledge of veterinarians about the disease, although it is the second most common disease among autoimmune dermatopathies in dogs [3].
Case Report
In July 2024, a six-year-old male Siberian Husky was attended at the specialized veterinary dermatology service, presenting itch, erythema, ulcers and depigmentation of the skin in the nasal region (Figure 1A). The dog had a previous history of corticosteroid therapy, which improved the appearance of skin lesions. According with tutor, when the use of corticosteroids was suspended, there was a recurrence of skin lesion. During general clinical evaluation, no noteworthy changes were found in other parts of body.

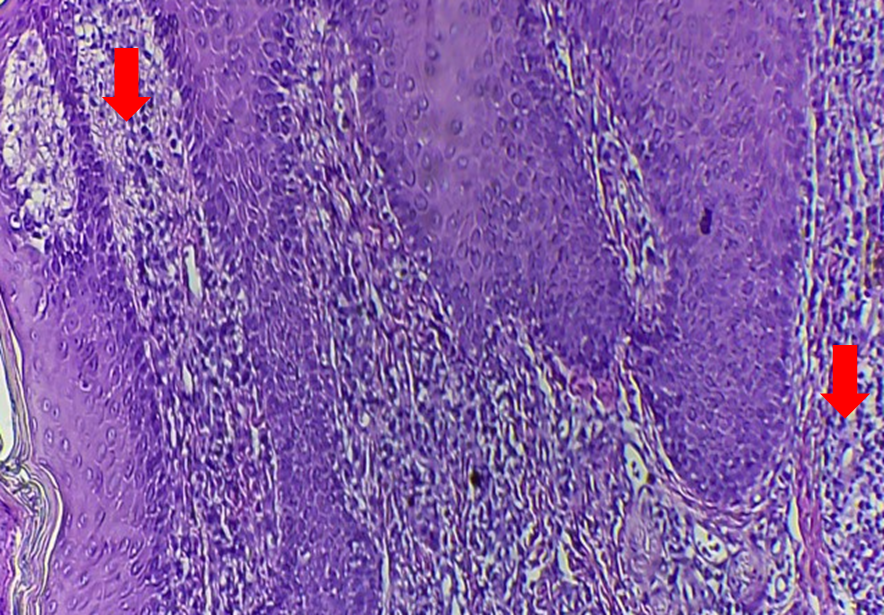
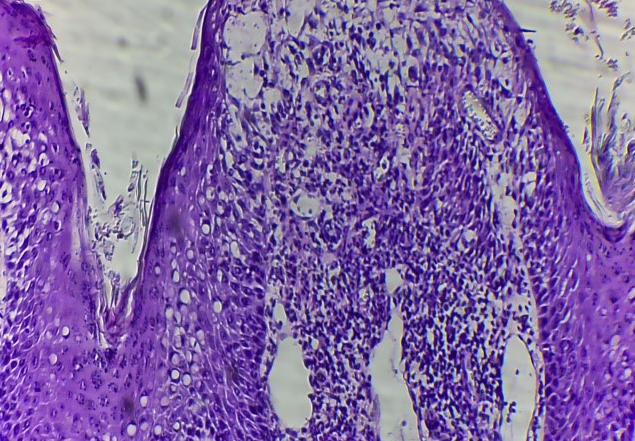
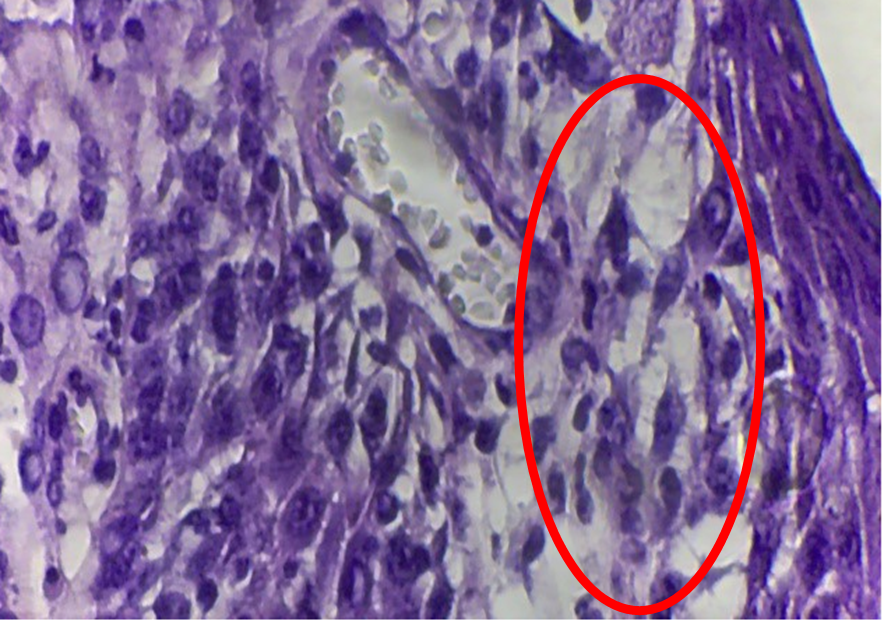
Complete blood count and serum levels of urea, creatinine, blood glucose, alanine aminotransferase, aspartate aminotransferase and alkaline phosphatase were performed, and also serology for canine leishmaniasis, chest x-ray and abdominal ultrasound. A biopsy of the nasal skin was performed for histopathological analysis. No changes were observed in the blood count or in analyses involving serum biochemistry. The chest X-ray did not identify lung lesions, and abdominal ultrasound did not indicate the presence of intra-abdominal masses. The result of histopathological analysis of samples obtained from the nasal skin was compatible with discoid lupus erythematosus by the presence of hyperkeratosis and parakeratosis of stratum corneum and vacuolar basal layer with marked separation of interphase (Figure 2), presence of lymphocytic inflammatory infiltrate in dermis (Figure 3), epidermal damage with interstitial edema (Figure 4) and vacuolization of basal layer with diffusion in dermoepidermal junction (Figure 5).
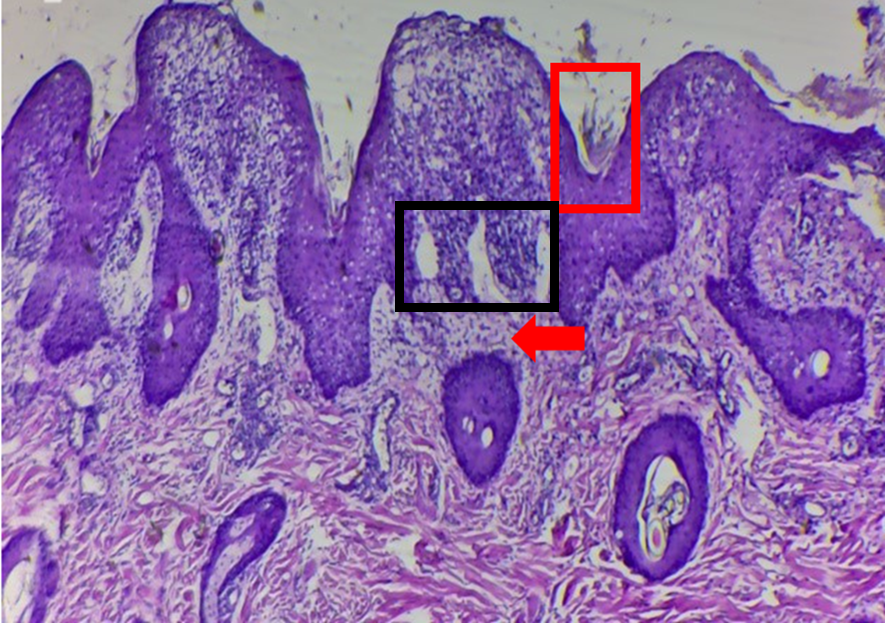
Figure 2: Histopathological analysis of nasal skin biopsy. Presence of hyperkeratosis and parakeratosis of stratum corneum and vacuolated basal layer (red square), with sharp separation of interphase (black square). Presence of inflammatory focus located in the dermis (red arrow) and edema of papillary plexus (Magnification 10X). Hematoxylin-Eosin (H&E) and Periodic Acid-Schiff (PAS) staining.
Discussion
The canine discoid lupus erythematosus is a chronic autoimmune disease, and can be suclassificated in facial discoid lupus erythematosus and generalized discoid lupus erythematosus [1]. The most common clinical presentation of discoid lupus erythematosus in dogs consists of a single chronic skin lesion, as observed in the dog of this study, considered typical for facial discoid lupus erythematosus, affecting the nasal plane. The skin lesions associated with facial discoid lupus erythematosus consist of erythema, depigmentation, ulceration, crusting, and partial or complete loss of normal nasal plane [2]. In generalized discoid lupus erythematosus, lesions may be generalized or multifocal, being distributed along the neck, back and lateral and ventral thorax [8]. This case describes the disease in a purebred dog, where these animals are described as the most affected [9]. The definitive diagnosis of autoimmune skin disease was confirmed through histopathological examination, which revealed the presence of dermo-epidermal changes. In the epidermis, the presence of acanthosis, orthokeratosis, vacuolization of basal cells, presence of apoptotic cells and lymphocytic exocytosis were observed. These findings are commonly present in cutaneous histopathological studies in canine discoid lupus erythematosus [2], being exacerbated by prolonged exposure to ultraviolet radiation. Ultraviolet A and B wavelengths (UVA and UVB) are capable of penetrating the epidermis and reaching the basal layer, triggering apoptosis, exposure of nuclear material and worsening inflammatory process [6, 10].
The inflammation affects the basal cells, destabilizing the basement membrane area. This layer’s function is to support the epidermal tissue and, when damaged, can create a fissure that can be seen in histopathological examination [1, 3], histological alteration described in this case report. The progression of inflammatory process culminates with disorganization and dysfunction of collagen fibers, which are responsible for maintaining the tissue structure [3, 11].
The discoid lupus erythematosus is the most common clinical form of lupus, representing, among the lupus variants, the one with the lowest risk for the development of systemic lupus erythematosus [1, 10]. Differential diagnosis was made for canine leishmaniasis due to the similarity of dermatological signs, since skin changes such as alopecic, hyperemic lesions and occurrence of hyperkeratosis in nasal plane are common signs of canine leishmaniasis and discoid lupus erythematosus [11]. In the dog in this case report, thoracic imaging was requested to rule out pulmonary fungal infection or metastasis in case of infectious or neoplastic disease, respectively. Similarly, abdominal ultrasound did not reveal the presence of an abdominal mass that could suggest paraneoplastic syndrome [12]. Since hematological and biochemical evaluations were within normal parameters for the species, and no changes were observed in imaging tests, it was defined that dog under study presented a clinical picture restricted to the tegument.
Histopathology is considered the gold standard examination for diagnostic definition, and the correlation between clinical signs and characteristic histological findings is necessary to confirmatory diagnosis of canine discoid lupus erythematosus [1, 3, 12]. Consistent with what has been described in literature, histopathology of dog’s skin in this case report demonstrated the presence of a band- like lichenoid infiltrate at the dermoepidermal junction and vacuolization of cells in the basal layer, histologic changes typically seen in facial discoid lupus erythematosus [1, 2, 3, 13]. Thus, the diagnosis of discoid lupus erythematosus was considered sufficient based on anamnesis, clinical examination, laboratory, imaging and histopathological findings.
Conclusion
Discoid lupus erythematosus is an autoimmune disease present in the clinical routine of small animals, requiring greater attention from the veterinarian to the use of different diagnostic methods, especially histopathology for diagnostic confirmation and clinical decision-making. This study highlights the importance of interdisciplinary communication between the clinical veterinarian and the pathologist to confirm consistent microscopic findings for confirmation of clinical findings and definitive diagnosis.
References
-
Olivry T, Linder KE, Banovic F (2018) Cutaneous lupus erythematosus in dogs: a comprehensive review. BMC Vet Res 14(1): 132.
-
Banovic F, Linder KE, Uri M, Rossi MA, Olivry T, et al. (2016) Clinical and microscopic features of generalized discoid lupus erythematosus in dogs (10 cases). Vet Dermatol 27(6): 488-e131.
-
De León-Robles E, Colmenares M, Calderón GM (2024) Case report of canine discoid lupus erythematosus in Guatemala. Vet Med Sci 10: 1-8.
-
Garelli CJ, Wong NB, Piedra-Mora C, Wrijil LM, Scarglia G, et al. (2021) Shared inflammatory and skin-specific gene signatures reveal common drivers of discoid lupus erythematosus in canines, humans and mice. Curr Res Immunol 2: 41-51.
-
Yang F, Li J, Jiang X (2024) Evidence for no genetic causal association between skin response to sun exposure and systemic lupus erythematosus: A Mendelian randomization study in Europeans and East Asians. Eur Acad Dermatol Venereol 38(8):e680-e682.
-
Jackson HA (2004) Eleven cases of vesicular cutaneous lupus erythematosus in Shetland sheepdogs and rough collies: clinical management and prognosis. Vet Dermatol 15: 37-41.
-
Kurz B, Klein B, Berneburg M, Meller S (2024) Ultraviolet radiation in the pathogenesis of lupus erythematosus. Dermatologie (Heidelb) 75(7): 528-538.
-
Banovic F (2019) Canine cutaneous lupus erythematosus: Newly discovered variants. Vet Clin North Am Small Anim Pract 49: 37-45.
-
Dumitrache MO, Ursache AL, Toma C, Negoescu A, Rietmann SJ, et al. (2024) Canine exfoliative cutaneous lupus erythematosus in two mixed breed littermates. Vet Dermatol.
-
Hejazi EZ, Werth VP (2016) Cutaneous lupus erythematosus: An update on pathogenesis, diagnosis and treatment. J Clin Dermatol 17(2): 135-146.
-
De Lucia M, Mezzalira G, Bardagí M, Fondevila DM, Fabbri E, et al. (2017) A retrospective study comparing histopathological and immunopathological features of nasal planum dermatitis in 20 dogs with discoid lupus erythematosus or leishmaniosis. Vet Dermatol 28(2): e200-e246.
-
Wiemelt SP, Goldschmidt MH, Greek JS, Jeffers JG, Wiemelt AP, et al. (2004) A retrospective study comparing the histopathological features and response to treatment in two canine nasal dermatoses, DLE and MCP. Vet Dermatol 15: 341-348.
-
Outerbridge CA (2013) Cutaneous manifestations of internal diseases. Vet Clin North Am Small Anim Pract 43(1): 135-152.
- Mitochondrial Bio-Logistics: Steering Co-Enzyme Q10 and Lycopene Synergies within the Science 4.0 Bio-OS Framework
- Hymenoptera Specimens from the Caño Negro Wetland, of the National Museum Collection, Costa Rica
- Science 4.0: Comprehensive Architecture of the Biological Operating System (Bio-OS) A Framework for Systemic Resilience and Industrialized Bio-Governance
- Rabbit on, or Hare Back? Understanding Climate Change
- Clinical Validation of Science 4.0: Flow Steering and Epigenetic Drift Inversion on a 76-Year-Old Hybrid System
- Seeds Planted by another Mind