A Case Report of Periodontal Disease in a Dog
Periodontal disease is the most common condition affecting the oral cavity of dogs, characterized by gingivitis and periodontitis, caused by the presence of aerobic bacteria that accumulate on the surface of tooth in form of biofilm, subsequently favoring the colonization and growth of anaerobic bacteria with pathogenic potential. In gingivitis, inflammation of gums occurs, and in periodontitis, loss of epithelial adhesion, progressive bone loss and tooth mobility occur. Numerous factors are associated with periodontal disease, such as race, age, dental arch occlusion disorders, retention of deciduous teeth and dental crowding. The most common clinical signs of periodontal disease are halitosis and gum inflammation. The diagnosis is made through direct visual examination, which can identify the presence of dental calculus deposition and gingival inflammation, and the use of imaging tests such as radiography and computed tomography is essential. Surgical treatment consists of complete removal of dental calculus, removal of unstable teeth and polishing of teeth. In this study, a report of periodontal disease was carried out in a Cavalier King Charles Spaniel dog, which presented a large amount of supragingival dental calculus on all teeth. The diagnosis was made through clinical signs, physical examination and computed tomography with 3D imaging. The treatment was carried out by extraction of mobile teeth, removal of dental calculus and polishing of the teeth.
Introduction
Periodontal disease is characterized by the inflammation of periodontal structures (gums, periodontal ligament, cementum or alveolar bone), and is classified as gingivitis or periodontitis according to the injured structure [1]. Bacterial plaque is considered the primary etiological agent of the disease, and the organic matrix responsible for plaque deposition is called dental biofilm, caused particularly by Gram- negative anaerobic bacteria. Periodontal disease is observed in dogs over three years of age with a frequency of up to 85% [2, 3, 4]. Periodontal disease is the most prevalent condition in the dental clinic of dogs and cats, being characterized by the presence of an inflammatory response triggered by the presence of organized bacterial plaque called dental calculus, which is deposited on the intra or extra-sulcular tooth surface, the color of which varies from yellow to dark brown [3, 4]. The most common clinical sign associated with disease is halitosis and gingivitis [5]. Numerous factors contribute to the development of periodontal disease, such as anatomical anomalies, persistent deciduous teeth, crowding (crooked teeth) and occlusion disorders [6, 7]. Insidious infection of periodontium components causes a chronic infection whose local immune response leads to the production of cytokines and other chemical mediators of inflammation that alter epithelial integrity, making the environment favorable for the entry of bacterial endotoxins into the bloodstream [8, 9].
The diagnosis of periodontal disease can be made through a specific physical examination and the use of imaging tests, such as intraoral radiographs and cone beam computed tomography, in which the X-ray tube-detector system captures images around the animal’s head, in a 360º rotation. These images below are read in specific software to create an image in three-dimensional format. This technique allows the identification of furcation exposure (loss of bone filling in the region between the roots), increased pericemental space and bone loss, with advantage that the animal absorbs lower doses of radiation [10, 11, 12].
After periodontal disease is diagnosed, the recommended treatment consists of removing dental calculus, smoothing and polishing the teeth [13]. General anesthesia is essential for carrying out the treatment, avoiding discomfort to the patient, especially in severe cases of the disease that require multiple tooth extractions [14].
Case Report
In October 2024, an 8-year-old male Cavalier King Charles Spaniel was seen, whose tutor main complaint was halitosis, the presence of dental calculus and oral bleeding after brushing of dog’s teeth. The tutor reported that the animal had never undergone dental treatment and that he brushed the dog’s teeth sporadically. During the clinical examination of the oral cavity, it was possible to observe accumulation of dental calculus and associated gingivitis, which was more evident in the upper and lower incisor teeth, and lower premolars on left side (Figure 1).

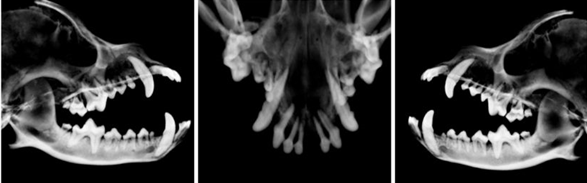
Tooth mobility was observed in the lower and upper incisor teeth, the first upper left premolar and the third lower left premolar, indicating the presence of advanced periodontal disease in some of these teeth. Routine preoperative exams were requested, such as blood count, serum biochemistry, type I urine, electrocardiogram, chest x-ray and abdominal ultrasound, and all the results of these exams were within normal parameters for the species. Cone beam computed tomography (Figure 2) was performed with 3D image reconstruction (Figure 3) to diagnose root fractures and resorptions, which are not always visible on intraoral radiography and are not detectable clinically.

Based on the findings of clinical evaluation and tomography, teeth with bone loss of supporting tissue were identified. The animal was anesthetized to remove the dental calculus and extract teeth that were mobile. Suture was then performed with absorbable 4-0 polyglactin thread in a simple discontinuous suture pattern and a mucogingival flap was used to close the gums. All affected teeth were also polished to remove stains (Figure 4).

During the transoperative period, meloxicam (0.2 mg/kg) and dipyrone (25 mg/kg) were administered subcutaneously for analgesia. As postoperative medication, dipyrone (25mg/kg) was prescribed orally every eight hours for three days, meloxicam (0.1 mg/kg) orally, every 24 hours, for three days, and commercial association of antibiotic containing metronidazole (dose = 12.5 mg/kg) and spiramycin (dose = 75,000 IU/kg) once a day orally, 3 days before and 7 days after surgical treatment. A diet according to the dog’s preference was also recommended, in the form of homemade food, dry or wet food and water ad libitum, and cleaning of gums after meals with an antiseptic solution containing 0.2% chlorhexidine in aqueous form. As absorbable thread was used for sutures, there was no need for a specific return to remove the stitches. The tutor was advised on the importance of brushing and annual monitoring with a specialized veterinarian to control and prevent recurrence of periodontal disease.
Discussion
The periodontal disease associated with bacterial plaque causes a chronic inflammatory response in protective and supporting periodontium [2]. Bacterial plaque is composed by bacteria on an organic matrix of glycoproteins and extracellular polysaccharides from saliva. The most common Gram negative bacteria describe is Neisseria, Veillonella, Haemophilus, Actinobacillus, Eikenella, Capnocytophaga, Porphyromonas, Prevotella, Fusobacterium and Escherichia; and Gram positive bacteria such as Streptococcus, Micrococcus, Staphylococcus, Peptoniphilus, Actinomyces, Propionibacterium, Enterococcus and Lactobacillus [2, 3, 4, 7]. Initially, the bacteria present in plaque are commensal microorganisms of oral cavity, which accumulate close in gingival margin, causing inflammation of tooth’s supporting tissues, leading to appearance of gingivitis and periodontitis [4]. Gingivitis is an inflammatory process that affects only the soft tissue, while periodontitis corresponds to inflammation that involves the alveolar bone, periodontal ligament and cementum [3]. With the continuous accumulation of bacterial plaque, the gingival sulcus region becomes the ideal environment for the proliferation of anaerobic and gram- negative bacteria, affecting the gums. The gum is the first structure to be damaged and become inflamed, giving rise to mild periodontal disease, which is reversible with removal of bacterial plaque [3].
If the bacterial plaque is not removed, the clinical picture progresses to moderate periodontal disease, characterized by inflammation of periodontium, such as observed in our case report. In this situation, an inorganic matrix forms above the gum, which adheres to the tooth, composed of saliva and mineralized food content, called dental calculus, whose color varies from yellow to brown [1].
The assessment of the patient’s dental status should be preceded by anamnesis and general physical examination, as described in our case report. Halitosis is a very common complaint and a finding commonly described on physical examination. When there is presence of dental calculus or periodontal disease, these odors are commonly altered or aggravated [5].
Periodontal assessment consists of identifying periodontal disease and differentiating between gingivitis and periodontitis. The degree of gingivitis is assessed based on redness, edema, and presence or absence of bleeding when probing the gingival sulcus. Tooth mobility is a consequence of periodontal disease, assessed in terms of horizontal and vertical movement by pressure exerted with handle of millimeter-sized periodontal probe on tooth during probing of periodontium [8], fact described in our case report for some teeth. In humans, periodontitis is categorized according to a multidimensional staging and classification system, which depends on the stage, severity of the disease at presentation and complexity of treatment. This classification includes necrotizing periodontal diseases (papillary necrosis, bleeding and pain) associated with deficiencies in the host’s immune response; endodontic-periodontal lesions, defined by a pathological communication between the pulp and periodontal tissues; and periodontal abscesses characterized by the localized accumulation of pus within the gingival wall of the periodontal pocket/sulcus, and which are associated with the risk of systemic dissemination [15].
Periodontal disease is characterized by edema and inflammation of gums, accumulation of debris around teeth, formation of bacterial plaque and deposition of calculus, purulent exudate, halitosis, ulcers, bleeding gums before or after probing, tooth mobility, tooth migration and formation of diastemas (space that forms between the teeth), extrusion and tooth loss [16].
The diagnosis is made through clinical examination, and the animal may also present dysphagia, excessive salivation and oral discomfort [13], facts not mentioned by animal’s tutor in this case report.
There are four stages of periodontal disease. Stage I is characterized by inflammation at the attached gingival margin. Stage II consists of mild periodontitis, where all the gums attached to the teeth are inflamed. The third stage is characterized by the presence of moderate periodontitis, with possible bleeding gums and presence of a large amount of dental calculus on the teeth. At this stage, the animal presents changes in behavior and eating habits, and the condition may be irreversible. The last stage presents a picture of chronic bacterial infection, with destruction of gums, teeth and periodontal bones [17, 18]. The progression of periodontal disease is related to the development of diseases such as bacterial endocarditis, liver, kidney, respiratory, and joint diseases [1, 2, 3, 4, 8].
Radiography is a fundamental diagnostic tool for veterinary dentistry, being useful in the evaluation of periodontal disease. There are several viable radiographic techniques for veterinary dentistry. The intraoral radiographic technique is more sensitive in detecting periodontal changes and is therefore more indicated than the extraoral technique for visualizing bone structures not visualized during the clinical inspection examination, assisting in the conduct during surgical treatment [19, 20].
Cone beam computed tomography is a diagnostic tool in which an X-ray tube-detector system captures images around the animal’s head, in a 360º rotation, which are read in specific software in three-dimensional format. This imaging technique allows the identification of furcation exposure, increased pericemental space and bone loss [21, 22]. In this case report, computed tomography was chosen instead of intraoral radiography technique due to the dog’s exposure to lower doses of radiation.
The treatment of periodontal disease consists of a set of procedures that involve subgingival curettage, crown polishing, and root planing. Tooth extraction is indicated in cases where there is exposure of grade III furcation and moderate or severe mobility [23, 24]. In this case report, treatment of periodontal disease consisted of scaling and removal of dental calculus, root planing, and subgingival curettage to remove dental calculus and plaque above and below the gum line using a closed method that does not require gingival incision. The crowns were polished using prophylactic toothpaste, removing pits in the enamel and making it difficult for new plaque to form. During the surgical procedure, one upper and one lower incisor tooth, and one upper and one lower premolar tooth were removed due to dental instability and associated bone loss. The gingiva was sutured with synthetic absorbable suture using a discontinuous suture pattern. Antibiotic therapy is an adjunctive treatment for periodontal disease and should not be used as the sole therapy. The antibiotics clindamycin, metronidazole and spiramycin are normally used [25, 26]. Antibiotic therapy should begin three days before the surgical procedure and must be continued for next seven days after the procedure. In this case report, a combination of antibiotics metronidazole and spiramycin was used, three days before and seven days after surgery, obtaining a good clinical result. Antibiotic therapy brings several benefits, such as reducing local inflammatory response, reducing bleeding caused by scraping, reducing halitosis and reducing of oral microbial load associated with the formation of biofilm and dental calculus [27, 28, 29].
Conclusion
The early identification of periodontal disease in dogs and its rapid resolution are decisive factors for successful treatment and a good prognosis. Correct referral of the dog for appropriate treatment by a veterinary specialist has a great influence on the prognosis, preventing systemic diseases such as endocarditis and pyelonephritis caused by the accumulation of bacteria. Therefore, proper cleaning of the oral cavity of dogs is extremely important to avoid bacterial proliferation, preventing the formation of dental calculus, periodontal disease, tooth loss and systemic diseases.
References
-
Wallis C, Holcombe LJ (2020) A review of the frequency and impact of periodontal disease in dogs. J Small Anim Pract 61(9): 529-540.
-
Rosan B, Lamont RJ (2000) Dental plaque formation. Microbes Infect 2(13): 1599-1607.
-
Niemiec BA (2008) Periodontal disease. Top Companion Anim Med 23(2): 72-80.
-
Kinane DF, Stathopoulou PG, Papapanou PN (2017) Periodontal diseases. Nat Rev Dis Primers 3: 17038.
-
Wang L, Liu X, Tang Y, Cai S, Zheng Z, et al. (2024) Effect of dental chew on reducing dental plaque, dental calculus and halitosis in beagle dogs. Res Vet Sci 174: 105304.
-
Wallis C, Ivanova A, Holcombe LJ (2024) Persistent deciduous teeth: Association of prevalence with breed, breed size and body weight in pure-bred cliente-owned dogs in the United States. Res Vet Sci 169: 1-8.
-
Sakarnyte L, Mockeliunas R, Siugzdiniene R, Merkeviciene L, Virgailis M, et al. (2024) Microbial composition of extracted dental alveoli in dogs with advanced periodontitis. Microorganisms 12(7): 1-13.
-
McFadden T, Marretta SM (2013) Consequences of untreated periodontal disease in dogs and cats. J Vet Dent 30(4): 266-275.
-
Harvey C (2022) The relationship between periodontal infection and systemic and distant organ disease in dogs. Vet Clin North Am Small Anim Pract 52(1): 121-137.
-
Martinez LA, Gioso MA, Lobos CM, Pinto AC (2009) Localization of the mandibular canal in brachycephalic dogs using computed tomography. J Vet Dent 26(3): 156- 163.
-
López FU, Kopper PM, Cucco C, Della Bona A, de Figueiredo JÁ, et al. (2014) Accuray of cone-beam computed tomography and periapical radiography in apical periodontitis diagnosis. J Endod 40(12): 2057- 2060.
-
Lee S, Lee K, Kim H, Na J, Lee T, et al. (2020) Comparison of dental radiography and computed tomography: measurement of dentoalveolar structures in healthy, small-sized dogs and cats. J Vet Sci 21(5): 1-8.
-
Niemiec BA (2008) Peridontal therapy. Top Companion Anim Med 23(2): 81-90.
-
Gengler B (2013) Exodontics: extraction of theeth in the dog and cat. Vet Clin North Am Small Pract 43(3): 573- 585.
-
Papapanou PN, Sanz M, Buduneli N, Dietrich T, Feres M, et al. (2018) Periodontitis; Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of periodontal and peri-implant diseases and conditions. J Periodontol 89: S173-S182.
-
Hajishengallis G (2014) The inflammophilic character of the periodontitis associated microbiota. Mol Oral Microbiol 29(6): 248-257.
-
Zacher A, Marreta SM (2022) Diagnosis and management of furcation lesions in dogs-A review. J Vet Dent 39(2): 151-172.
-
Albuquerque C, Morinha F, Requicha J, Martins T, Dias I, et al. (2012) Canine periodontitis: the dog as an important model for periodontal studies. Vet J 191(3): 299-305.
-
Peralta S, Verstraete FJ, Kass PH (2010) Radiographic evaluation of the types of thooth resorption in dogs. Am J Vet Res 71(7): 784-793.
-
Bannon KM (2013) Clinical canine dental radiography. Vet Clin North Am Small Anim Pract 43(3): 507-532.
-
Huang YH, Lee B, Chuy JÁ, Goldschnidt SL (2022) 3D printing for surgical planning of canine oral and maxillofacial surgeries. 3D Print Med 8(1): 1-7.
-
Linder K, MacGee S, Schultz L (2023) Prevalence of root fusion in canine maxillary second molar teeth using cone-bean computed tomography. Front Vet Sci 10: 1-5.
-
Golub LM, Lee HM (2000) Periodontal therapeutic: Current host-modulation agents and future directions. Periodontol 82(1): 186-204.
-
Niemiec BA (2008) Periodontal therapy. Top Companion Anim Med 23(2): 81-90.
-
Cunha E, Tavares L, Oliveira M (2022) Revisiting periodontal disease in dogs: How to manage this new old problem? Antibiotics (Basel) 11(12): 1-13.
-
Ljungquist D, Andersson M, Areskog M, Andersson AM (2024) Antibiotic use in dental care of dogs, cats, and rabbits in Sweden. J Vet Dent 41(3): 192-196.
-
Nielsen D, Walser C, Kodan G, Chaney RD, Yonkers T, et al. (2000) Effects of treatment with clindamycin hydrochloride on progression of canine periodontal disease after ultrasonic scaling. Vet Ther 1(3):150-158.
-
Khazandi M, Bird OS, Owens J, Wilson G, Meyer JN (2014) In vitro efficacy of cefovecin against anaerobic bacteria isolated from subgingival plaque of dogs and cats with periodontal disease. Anaerobe 28: 104-108.
-
Miyaji H, Mayumi K, Kanemoto Y, Okamoto I, Hamamoto A, et al. (2022) Ultrasonic irrigation of periodontal pocket with surface pre-reacted glass-ionomer (S-PRG) nanofiller dispersion improves periodontal parameters in beagle dogs. Oral Biosci 64(2): 222-228.
- Mitochondrial Bio-Logistics: Steering Co-Enzyme Q10 and Lycopene Synergies within the Science 4.0 Bio-OS Framework
- Hymenoptera Specimens from the Caño Negro Wetland, of the National Museum Collection, Costa Rica
- Science 4.0: Comprehensive Architecture of the Biological Operating System (Bio-OS) A Framework for Systemic Resilience and Industrialized Bio-Governance
- Rabbit on, or Hare Back? Understanding Climate Change
- Clinical Validation of Science 4.0: Flow Steering and Epigenetic Drift Inversion on a 76-Year-Old Hybrid System
- Seeds Planted by another Mind