Review on Q Fever in Small Ruminants and its Public Health Importance
Q fever is a disease caused by coxiella burnetii which is ubiquitous intracellular bacterial pathogen, with acute and chronic clinical manifestations. This bacterium is able to infect a wide range of animals, but cattle, sheep and goats are the principal reservoirs. Inhalation of contaminated aerosols is the main transmission route for humans. Q fever is a worldwide zoonosis, which may occur in sporadic as well as epidemic forms. Because it is highly infectious for humans, Q fever is an important zoonosis with veterinarian laboraratory workers, farmers and abattoir workers at risk. The spectrum of clinical manifestations in humans and animals are diverse, ranging from seroconversion without any clinical symptoms to fatal consequences. The acute infection in humans manifests as self-limiting febrile illness, pneumonia, or hepatitis, whereas endocarditis is the major manifestation in chronic cases. Infection in domestic animal is usually asymptomatic and remains unrecognized, but it may cause abortion, especially in sheep and goat. In Ethiopia, the existence of antibody against Coxiella burnetii was reported in goats and sheep slaughtered at Addis Ababa abattoir, and its peri-urban .or from milk and urine are the basis of confirmatory diagnosis of C. burnetii infection. Doxycycline and tetracycline is the recommended antibiotic for humans. Cotrimoxazole and rifampin are the drugs of choice for the patients allergic or contradicted to tetracyclines. Oxytetracycline in the last trimester of pregnancy is usually recommended for animals. Control of Q fever in humans is largely dependent upon the control of infection in animals. The risk for transmission can be decreased through attention to proper sanitation when dealing with parturient animals and ensuring proper pasteurization of milk products.
Introduction
Query fever (Q fever) was first observed in 1935 in Queensland, Australia as an outbreak of a febrile illness of unknown origin. It was observed among abattoir workers and that is when Q fever was first acknowledged [1]. However, McDade stated that Queensland was the state in which the disease described first and thus, named as Q fever, where the Q stood for Queensland. Q fever is a widespread disease caused by the bacteria Coxiella burnetii, is a small (0.2-1.0μm long and 0.2-0.4μm wide). The causative agent of Q fever in humans and animals is an obligate gram-negative intracellular bacterium of the family Coxiellaecae [2]. It is able to infect mammal, birds, reptiles and arthropods but cattle, sheep and goats are the principal reservoirs. Q fever is listed in the OIE Terrestrial Animal Health Code and Member Countries and Territories are obligated to report occurrences of the disease to the OIE according to the OIE Terrestrial Animal Health Code.
The etiologic organism of Q fever was first isolated by Burnet and Freeman and named it Rickettsia burnetii. It causes a mild disease in ruminants, but can cause abortions and still births in cattle, sheep and goats. It is also a zoonosis, a disease of animals that can infect humans. Coxiella burnetii infection can produce both acute and chronic forms of the disease in humans. A self- limiting febrile condition is the most frequent manifestation in most cases [3]. Spontaneous abortion, intrauterine foetal death, premature delivery or retarded intrauterine growth may occur in pregnant women [4].
Mortality is a rare outcome of the acute form of the disease. The major clinical manifestation of chronic form of Q fever is endocarditis with case fatality in untreated cases exceeding 10% [5]. Beside zoonotic importance, Coxiella burnetii also produce health and production problems in domestic ruminants including cattle. Infection in cattle usually remains unrecognized but it causes sporadic reproductive problems such as abortion, infertility and mastitis [6, 7].
In Ethiopia, the existence of antibody against Coxiella burnetii was reported in goats and sheep slaughtered at Addis Ababa abattoir, and its peri-urban zone [8]. A seroprevalence of 6.5% was also reported in Addis Ababa abattoir workers [9]. To assess Seroprevalence of Coxiella burnetii in pastoral livestock in southeast Ethiopia, a cross-sectional study was carried out in three livestock species (cattle, camels and goats). The study was conducted from July 2008 to August 2010, and eight pastoral associations from the selected districts were included in the study Sera from a total of 1830 animals, comprising 862 cattle, 458 camels and 510 goats were screened initially Out of sera from total of 1830 animals, 20% were randomly selected (180 cattle, 90 camels and 98 goats) and tested for C. burnetii using ELISA. The seroprevalence of Coxiella burnetii were 31.6% (95% CI, 24.7-39.5), 90.0% (95% CI, 81.8-94.7) and 54.2% (95% CI, 46.1-62.1) in cattle, camels and goats, respectively. The seroprevalence of C. burnetii found in this study is high in all the three animals species studied. Therefore, the objective of this review is to highlight Q fever in the small ruminants and its public health importance.
Etiology
Q fever is caused by obligate intracellular bacteria called Coxiella b_urnetii_ which has a cell membrane similar to Gram negative bacteria [10, 11]. The agent differs from other rickettsiaeinits filterability and high degree of resistance to physical and chemical agents. It has been found to have several different plasmids, the functions of which are not yet understood. Coxiella burnetii can be highly pleomorphic when it reproduces inside the phagolysosomes of an invaded host cell. Two different orms can be distinguished under an electron microscope: one, large and bacilliform and the other coccoid, which develops rom the former and has greater electronic density. A third form appears in the large cells after passage through embryonated eggs or BGM cell cultures when they have been kept in suboptimal temperature conditions or fresh medium has not been added. These small, high-density forms are similar to spores. The morphogenesis is comparable, but not identical to cell differentiation in the formation of endospores. These small forms are responsible for the high resistance of the agent to environmental factors and many disinfectants [12].
Epidemology
Q fever is a worldwide zoonosis, which may occur in sporadic as well asepidemic forms. It may be emerging disease, probably related to climate change Very recently, Dave and others published a review on the impact of climate change on the emergence of human vector borne diseases [13]. Many animals and arthropods act as reservoirs of infection. However, the most commonly identified sources of human infections are farm animals such as cattle, goats, and sheep, Pets, including cats, rabbits, and dogs, have also been demonstrated to be potential sources of urban outbreaks of disease [14].
Source of Infection
Coxiella burnetii_is considered a pathogen with no host specificity and it was shown that infection may occur in a wide range of vertebrates, including wild and domestic mammals, birds and arthropods [2]. Babudieri stated that _Coxiella burnetii was detected in virtually all of the animal kingdom. However, the clinical Q fever is mostly seen in humans. Cattle, sheep and goats are considered to be the most common source of human infection [15].
Method of Transmission
Coxiella burnetii bacteria have unique properties that contribute to their transmission between hosts: (1) unlike other members of the Rickettsiaceae, the life cycle of Coxiella burnetii_is not dependent on arthropods as vectors; and (2) the SCV form is highly resistant in harsh environment. Inhalation of contaminated fomites is the most common mode of transmission to humans. Domestic ruminants serve as the primary source of human infection [5]. However; many other animal species may play a role in _Coxiella burnetii transmission. Parturient cattle, ewes and goats can excrete very high quantities of bacteria through amniotic fluid and foetal membranes [16].
Direct contamination by aerosols may occur from these products of parturition. Abortive animals may continue to shed bacteria for a long period. Infected animals may also shed Coxiella burnetii in milk, urine, faeces and uterine discharge [16]. Milk is the most common shedding route for goats and cattle, whereas ewes shed bacteria most commonly in faeces and vaginal mucus [17]. Excreted bacteria contaminate fomites such as wool, clothing, straw, manure etc., which may serve as vehicles for transmission [18].
Indirect transmission to humans may result from the handling of contaminated farm utensils, straw, manure, or by dust from farm vehicles. Coxiella burnetii may also spread through the air, and therefore, infection may occur in a person without any history of animal contact [5, 18]. However, in some studies it was shown that wind spread is not an important mode of Coxiella burnetii transmission [19].
Ingestion of contaminated milk and milk products could be a potential source of human infection. However, it was not evident in an experimental study. Rare, but sporadic cases of human-to-human transmission of Q fever have occurred to attendants during autopsies and following contact with a pregnant woman [20]. Sexual transmission of Coxiella burnetii infection was also reported in a study.
Dogs and wild carnivores may be infected by ingestion of contaminated ruminant placenta or birth products, or by the aerosol route [2]. Although ticks are not essential for the life cycle of Coxiella burnetii, they may still play an important role in transmission of the infection in wild vertebrates [21].
![Figure 1: Source and transmission of Q fever [22].](/fulltextimages/2740/fig_1.jpeg)
Risk Factors
Agent factor: The severity of the infection depends on the strains of the infecting bacteria. Phase I type bacteria are more virulent than the phase II type [23]. Acute infection in humans is caused by Coxiella burnetii genomic type I- III, whereas type IV and V are responsible for chronic infection. The virulence of type VI is unknown [24]. Host Factor: Age and gender are the two risk factors which are shown to influence the occurrence of Q fever in humans. People aged 30-60 years are the most vulnerable group, and the clinical disease is mostly prevalent in men [25]. People with a previous history of valvulopathy, an immunosuppressive disease like AIDS and pregnant women are the most susceptible [26]. People in certain occupations like veterinarians, animal farm workers, abattoir workers and laboratory personnel are at a higher risk of being infected or seropositive than others; and studies show a comparatively higher prevalence in these groups [27].
A relationship of Coxiella burnetii infection with age and sex was also found in animals, particularly in cattle. Several studies have shown that the prevalence of Coxiella burnetii infection increases with age or with the number of parity in cattle and sheep [28]. Prevalence is higher in dairy cows than in beef cattle. Among the dairy cattle breeds, prevalence was reported to be higher in Holstein [29]. Increasing animal density increases the infection load in the environment, and is therefore, a potential risk factor of Coxiella burnetii infection. Several studies in cattle show that seroprevalence increases with an increasing herd size [29, 30]. Flock size is reported to have a similar effect in sheep [31]. Several management factors such as housing systems, isolation of a newly introduced animal may also contribute to the seroprevalence of Coxiella burnetii infection in animals [30]. Season, Environment and Management Factors: Seasonal variation is observed in the occurrence of human Q fever. This variation, however, varies according to geographical region. But most cases of Q fever have been reported in the spring or early summer [25]. Human Q fever has been shown to have a relationship with rainfall rather than season [19]. A high prevalence of Q fever was observed among people living in close proximity to infected animals or in areas with a high livestock density [32].
Pathogenesis
The pathogenesis of Coxiella burnetii infection in humans and animals is not clearly understood. But, it is believed that bacterial LPS play an important role in the pathogenesis of Q fever in both humans and animals [2].
The organism probably follows the oropharyngeal route as its port of entry into the lungs and intestines of both humans and animals [19]. It is highly infectious, and a very low dose is sufficient to initiate infection [33]. Primary multiplication takes place in the regional lymph nodes after the initial entry, and a transient bacteraemia develops which persists for five to seven days [34].
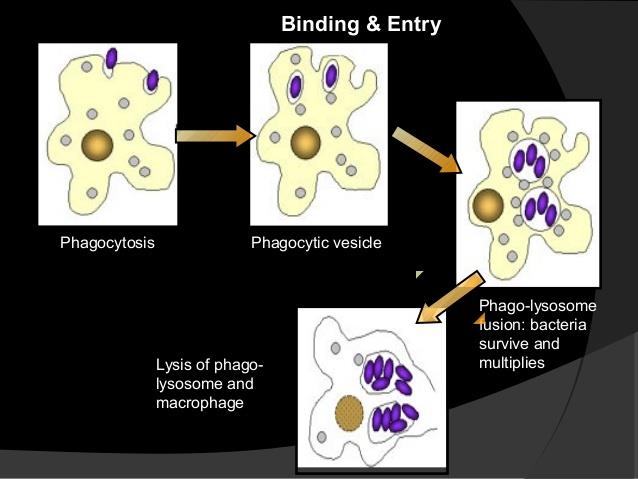
Coxiellaburnetii has two morphologically distinct cell variants; an intracellular and metabolically active large cell variant (LCV) and a spore like small cell variant (SCV) [35]. These two forms are morphologically and functionally distinct. The LCV is larger, elongated less electron-dense bacteria and metabolically active and replicating large bacteria [36]. While, the SCV presents a compact rod-shaped with a very dense central region and it is considered the metabolically dormant and less replicating [37]. The SCV are shed by infected animals. After infection the organism attaches to the cell membrane of phagocytic cell. After phagocytosis, the phagosome containing the SCV fuses with the lysosome. The SCV are metabolically activated in the acidic phagolysosomes and can undergo vegetative growth to form LCV [5].
The LCV and the activated SCV can both divide by binary fission and the LCV can also undergo sporogenic differentiation [2, 35]. The spores that are produced can undergo further development to become metabolically inactive SCV. And both spores and SCV can then be released from the infected host cell by either cell lysis or exocytosis [5].
The acidic environment also protects Coxiella burnetii from the effects of antibiotics, as the efficacy of antibiotics is decreased in the acidic PH [38]. The SCV and spore forms are more difficult to denature than LCV [39].
Coxiella burnetii also has two distinct antigenic phases, Phase I and Phase II, based on changes that occur in the organism during in vitro culture. The primary significance of these two phases is that antibodies to phase II antigens are made during the early stages of the infection, but antibodies to phaseI antigens predominate if the organism persists longer. This switch is used to distinguish acute from chronic infections in people, although it is not currently employed in animals. Phase I bacteria (wild virulent type) with a smooth full length LPS were isolated from infected humans, animals and arthropods [5]. Phase I bacterium converts to an avirulent phase II with rough LPS after several passages in embryonated egg or cell cultures [40]. The virulence and the pathogenicity of the _Coxiella burnetii_are associated with genetic characteristics, plasmid groups and type of strains and also with host factors such as pregnancy [24, 34].
Coxiella burnetii enters monocytes or macrophages; the only known target cells, by phagocytosis in humans [38, 41]. The phagocytotic process differs for phase I and phase II bacteria. Phase II bacteria enter the host’s cells through CR3-receptor mediated phagocytosis by activating the CR3 receptors [38]. On the other hand, the attachment of phase I Coxiella burnetii to a monocyte is aided by leukocyte response integrin (LRI) αvβ3, and integrin-associated protein (IAP) [38]. In spontaneous infections, the phase I Coxiella burnetii survives within the phagocytic cells, as the internalisation of the bacteria by these cells is poor. In contrast, uptake of the phase II C. burnetii by monocyte is rapid [38]. Infection with phase II Coxiella burnetii_induces secretion of both IgG and IgM, whereas phase I _Coxiella burnetii can only induce IgM production [5].
Clinical Signs
Clinical Sign of Q fever in Small Ruminants
Most cases of animal infection are asymptomatic [42]. The organism is found in the blood, lungs, liver and spleen during acute experimental infection, whereas chronically infected animals persistently shed bacteria in their faces and urine. Infection in most domestic animals remains unrecognized. Coxiellosis is considered a cause of abortion and reproductive disorders in domestic animals [2]. There is scientific evidence to support the hypothesis that _Coxiella burnetii_can induce epidemics of reproductive failure in sheep and goats, but not in cattle Reproductive disorders in domestic animals include endometritis, metritis, stillbirth, reduced birth weight and infertility [43].
The herd level prenatal mortality and rate of still birth were not associated with the level of Coxiella burnetii antibodies in bulk tank milk in Danish dairy cattle [44]. Abortion rate is comparatively higher in ewes and goats than in cows. Abortion is usually observed in late pregnancy in both ewes and cattle [42]. In most abortive cases, the aborted foetus appears normal. Discoloured exudate and intracotyledonary fibrous thickening may be observed in an infected placenta. Severe myometrial inflammation and metritis are the frequently observed clinical manifestations in goats and cows, respectively [16].
Clinical Signs of Q fever in Humans
Coxiella burnetii infections produce both acute and chronic forms of clinical manifestations in humans.
However, 60% infection remains asymptomatic with a few patients developing severe illness [16]. The incubation period of Q fever is 2-3 weeks, depending on the route of infection [5]. Clinical signs of acute Q fever are nonspecific and vary among patients. A self-limiting febrile condition is the most frequent manifestation in clinical cases, which is accompanied by severe headaches, myalgia, arthralgia and a cough [3].
A prolonged fever, which may reach 39-40oC, usually stays for 2-4 days and then gradually decreases to a normal level through the following 5-14 days [5]. Atypical pneumonia is another common symptom of acute Q fever. Pneumonia is mild in most cases being characterized by a dry cough, fever, and minimal respiratory distress. Patients may also develop hepatitis with hepatomegaly, but without jaundice, subclinical hepatitis and granulomatous hepatitis with a prolonged fever [5]. Generally, hepatitis develops in young immunosuppressed patients, whilst pneumonia is often seen in older patients [45].
Myocarditis is found in 2% of patients with the acute illness, which may be accompanied by pericarditis [22]. Skin rashes and neurologic disorders such as meningoencephalitis or encephalitis, lymphocytic meningitis and peripheral neuropathy have also been observed in acute Q fever cases [46]. Spontaneous abortion, intrauterine foetal death, premature delivery or retarded intrauterine growth may occur in women that become infected during pregnancy [4]. Pregnant woman may become chronically infected and abort in subsequent pregnancies [5]. Mortality is a rare outcome of the acute form of the disease. However, severe respiratory distress and myocarditis may lead to death [22].
An infection which lasts for more than six months after the onset is defined as chronic Q fever. This happens in less than 5% of cases [25]. The major clinical manifestation of this form of the disease is endocarditis [3]. It occurs in 60-70% of all chronic cases [5]. The case fatality of Q fever endocarditis is less than 10% when patients are treated with antibiotics. The aortic and mitral valves are usually affected [5]. Unspecific signs like intermittent fever, cardiac failure, weakness, fatigue, weight loss or anorexia may be present. Other manifestations are osteomyelitis, osteoarthritis, chronic hepatitis, hepatomegaly, splenomegaly, digital clubbing, purpuric rash and an arterial embolism [3].
Diagnosis
There are no specific clinical sign of Coxiella burnetii infection in human and animals. Therefore, laboratory diagnosis is the only way to confirm the disease. Since Coxiella burnetii is highly infectious, biosafety level 3 laboratories and experienced laboratory personnel are required to handle the contaminated specimens [45]. For laboratory diagnosis in the context of serial abortion or parturition for detection and identification of C.burnetii in animals. If possible, vaginal swabs at the day of parturition (or taken less than 8 day after) should be collected in order to limit the number of false-negative PCR results. Milk from the tank, individual milk or colostrums, vaginal or faecal sample can be taken for investigating bacterial shedding [47].
Isolation of the Agent
Due to the zoonotic nature of the agent, isolation of Coxiella burnetii is not performed for routine diagnosis in veterinary medicine. The main reasons are the high level of expertise required, the time consumed and requirement of the BSL3 laboratories confinement [48]. Therefore, isolation of bacteria is done using the shell-vial cell culture techniques or culture in the yolk sacs of embryonated eggs. Isolation of the Coxiellosis from positive PCR samples was amplified through infection of 6-7 days old specific free Embryonated chicken egg in the yolk sac. The inoculations were carried out in sterile conditions, through the opening in the center of an air chamber. The embryos were incubated at 37˚С with the ovoscopy being carried out on a daily basis during the period of 15 days. In order to detect the coxiellas by light microscope we prepared smears of yolk sacs of CE, The preparations were stained by the classical methodology of Gimenez stain and displayed by light microscopy [49].
Especially, in their yolk sacs, which became a useful indicator of the Coxiellosis infection In diligently stained preparations of yolk sacs, dot-like oval and spherical coxiellae, coloured in different shades of red, or in violet, were observed and located in the cytoplasm of the endodermal cells in the shape of inclusions or with a diffusion distribution.
![Figure 3: Endodermal Cells [49].](/fulltextimages/2740/fig_3.jpeg)
Staining
The routine diagnosis of Coxiellosis in aborted ruminant is to detect the pathogen using staining techniques. Smears are usually stained by stamp, Gimenez, Machiavelloor Giemsastain [2]. The presence of large masses of red-colored coccobacilli will indicate a strong presumptive diagnosis of Coxiella burnetii. However, these diagnostic methods are poorly sensitive and not specific due to possible confusion with the other pathogens such as Brucella sppor Chlamydia spp. [50]. This followed by serological analysis by the complement fixation testor better by ELISA [51]. However stanining techniques cannot be specific and they have reduced sensitivity especially with vaginal swabs, milk and a fecal sample [48].
Serological Tests
Complement Fixation Test (CFT): Although the CF test is prescribed by OIE as a diagnostic method for C.burnetii, its sensitivity is week. Antibodies of Coxiella burnetii in sheep and goat cannot be detected frequently by the antigen of the specific test [52]. However, its use is now infrequent, as it has displayed a lower sensitivity than the ELISA [53]. The advantage of CFT is that it does not require host specie-specific antibodies [54]. This test is highly specific, but weakly sensitive [51, 54]. Moreover, CFT cannot detect early stages of infection as the complement fixing antibodies do not appear in exposed individuals in early stages of the infection [54]. Therefore, samples from both convalescent and acute phases are required to accurately diagnose the infection. It has been shown that the antigens used in CFT often fail to identify seropositive sheep and goats [51]. Immunoflouorescence Assay (IFA): IFA is a species specific test and is not often used for diagnosis of Coxiella burnetii infection in animals. It has been widely used and remains a frequently used method for diagnosis of human infection [5, 18, 27, 55]. The IFA allows for the differentiation between a suspected acute and chronic clinical infection in humans, based on the ratio of phase I and phase II IgG antibodies. If the phase I titer is greater than or equal to phase II, the sample is indicative of chronic exposure and if phase II titer is greater than the phase I titer, the sample is indicative of an acute exposure. There is no yet any commercial kit using IFA for veterinary investigation [16]. Enzyme linked Immunosorbant Assay (ELISA): Several studies in humans have shown that enzyme-linked immunosorbant assay (ELISA) has a higher sensitivity than CFT and IFA [56]. It is recommended as a useful diagnostic tool for sero-epidemiological studies [57]. ELISA can detect antibodies against both phase I and phase II antibodies [25]. This test has a higher sensitivity than the CFT in animal studies [52, 58, 59]. CFT is a quick diagnostic technique it allows the testing of a large number of samples at the same time and is a popular tool for sero-epidemiological studies in animals [59]. Polymerase Chain Reaction (PCR): Recently, several polymerase chain reaction (PCR) techniques have been developed and successfully used to detect Coxiella burnetii DNA in cell cultures and in clinical samples [48, 60]. This technique is highly sensitive and specific, and is a rapid tool for Coxiella burnetii detection [59]. PCR also has improved the diagnosis of Q fever in veterinary science [61].
Differential Diagnosis
In animals the differential diagnosis includes other causes of abortion and infertility like leptospirosis, brucellosis, Listeriosis, and salmonellosis. In case of leptospirosis abortion occurs with or without placental degeneration and encephalitis, Abortion usually occurs 3- 4 weeks later. In coordination, excessive salivation, conjunctivitis and muscular rigidity are the common signs additionally hemoglobinuria, pallor of mucosa and jaundice also seen. Most affected animals are found dead, apparently from septicemia.
Listeriosis has signs like edema, septicemia, encephalitis and meningoencephalitis, called circling disease in its common form. Affected animals circle, in one direction only and display swallowing, fever, blindness and head pressings. Paralysis and death follow in 2 to 3 days and there is also necrosis of the placenta which leads to abortion. Listerial abortion usually Occurs in late gestation. The fetus may be macerated or delivered weak and moribund.
Brucella is a life longer infection it causesorchitis, epididymitis, synovitis generally it will cause sterility in male. Hygromatous swellings, especially of the knees, and nonsuppurative arthritis of the stifle joints may occur and in case of female animals it causes abortion around the 7th month of pregnancy. Retention of the placenta and metritis are also common. Salmonellosis also causes abortion in the last 2 month of gestation followed by fever, dehydration and sever and foul-smelling diarrhea [62].
Public Health Importance
Because it is highly infectious for humans, Q fever is an important zoonosis with veterinarian laboraratory workers, farmers and abattoir workers at risk. Surveys have shown that significance numbers of livestock handlers have antibodies indicating exposure to the organism. Less than half of people infected become ill, and most infections are mild. But affected persons can develop a high fever with headache, muscle pains, sore throat nausea and vomiting, chest and stomach pains. The fever can last for one or two weeks, and lead to pneumonia or affect the liver. Treatment involves long term antibiotic therapy. In a small percentage of cases, a chronic severe debilitating disease occurs. People with suppressed Immune systems and those with pre-existing heart valve problems are at risk of this complication, which is often fatal There is also a post Q fever syndrome of chronic fatigue Q fever is the second most commonly reported laboratory infection with several recorded outbreaks involving 15 or more persons [63].
In humans, initial exposure to Coxiella burnetii may result in asymptomatic or mild infection but also in acute or chronic disease [26]. The clinical diagnosis can be very difficult. The reasons for this high clinical polymorphism are largely unknown, even if risk factors of severity (e.g., pregnancy, immunosuppression, preexisting cardiac valvulopathy, vascular grafts, and aneurysms) have been described. Although rarely fatal, the disease may lead to substantial morbidity and can be highly debilitating, even under treatment. Most human cases result from the inhalation of dust particles contaminated by infected livestock or animal products [2].
Treatment
Treatment of acute Q fever
Acute Q fever is generally self-limited and many patients recover without antimicrobial therapy Treatment for acute Q fever is not routinely recommended for asymptomatic persons or for those whose symptoms have resolved, although it might be considered in those at high risk of developing chronic Q fever (e.g., valvular heart disease, vascular graft, aneurysm, and immunosuppression.
Doxycycline at 200 mg daily for 14 days is the recommended regimen for acute cases of Q fever [25]. Unless patients are allergic to Doxycycline, pregnant, or younger than 8 years (cotrimoxazole) Cotrimoxazole and rifampin are also drugs of choice for patients allergic to or in whom tetracyclines contradicted. Long-term (>5 weeks) use of cotrimoxazole with folinic acid is recommended for pregnant women [4].
Treatment of chronic Q fever
Endocarditis is the most common form of chronic Q fever Combination therapy should be considered standard treatment for patients with Q fever endocarditis. The current recommendation for treatment of Q fever endocarditis is oral Doxycycline (100 mg twice daily) plus hydroxychloroquine (200 mg 3 times daily)1 for at least 18 months; however, therapy may need to be prolonged. For patients unable to tolerate hydroxy chloroquine, an alternative regimen of Doxycycline plus an FQ for a minimum of 3 to 4years has been proposed. Doxycycline plus rifampin has also been suggested as an alternative therapy; however, drug interactions may limit the usefulness of this combination Patients who receive prolonged hydroxychloroquine treatment should have an ophthalmologic examination every 12 months. At-risk populations should be screened for glucose-6-phosphate dehydrogenase deficiency before receiving hydroxychloroquine therapy, and patients who receive treatment with Doxycycline should be reminded about photosensitivity. Endovascular complications are another major group of chronic infections (9%) In a report of 30 cases, surgical treatment (aortic aneurysm repair or graft replacement) at time of Q fevers [64]. Diagnosis was significantly associated with survival (23 of 24 patients who survived underwent surgery; only 2 of 8 patients who died underwent surgery) because a variety of antibiotic regimens were used in this series, the optimal regimen could not be determined. However, most patients were treated with combination Doxycycline- hydroxychloroquine. Two injections of Oxytetracycline (20 mg per kg body weight) in the last trimester of pregnancy are usually recommended for animals, although this may not completely suppress abortions or stop bacterial shedding during parturitions [17].
Control and Prevention
During outbreak, some sanitary measures should be applied to reduce transmission of the disease within the animals. Changes in the farming practices including manure management such as covering and natural composting or ploughing of manure, treating manure lime(or calcium cyanide and the removal of animal birth and abortion products [64, 65]. Disinfection of the infected premises including paths and general environments of holding and the implementation of a farm animal breeding However the effectiveness of different control measures remain uncertain. It has been reported that the prevalence of Coxiella burnetii in an infected herd usually declines overtime, even without taking any control measures. This is probably due to natural immunization of suspected animals [65].
Vaccinations have been shown to reduce abortion, shedding of Coxiella burnetii and the occurrence of infection in animals Outbreak vaccinating herds that are already infected [66]. The inactivated phase I vaccine protects efficiently against abortion and has been shown to prevent bacterial shedding in vaginal mucus, feces, and particularly in milk. Vaccine trials with killed vaccines in animals show a good and persistent antibody response and suggest that vaccination can limit the excretion of the organism. A vaccine inactivated by formaldehyde prepared from the strain of phase I Coxiella burnetii, received the approval of the Australian authorities in1989.Results converge today towards the use of a phase I vaccine, as the phase II vaccines are 100 times less effective against the colonisation of mouse spleen than phase I vaccines [67]. However, vaccination proved more effective in nulliparous animals than in parous animals. Furthermore, vaccination did not clear infection in previously infected goats and cattle [64]. Phase I vaccines are more effective, but vaccination is contraindicated for individuals who had sero converted or had been exposed to Coxiella burnetii prior to immunization. It is preferable to select sero negative herds or animals for immunization, and to continue vaccination over several years in young animals [68, 69, 70, 71, 72, 73, 74, 75, 76, 77, 78, 79, 80, 81, 82, 83].
Conclusion
Q fever is a worldwide zoonosis, which may occur in sporadic as well as epidemic forms. The most commonly identified sources of human infections are farm animals such as cattle, goats, and sheep, Pets, including cats, rabbits, and dogs, have also been demonstrated to be potential sources of urban outbreaks of disease. It is also known to be a cause of reproductive failure in domestic animals, including cattle. Domestic ruminants are considered the main reservoir for Coxiella burnetii. The causative agent is transmitted to humans through direct contact with reproductive products of animals. Aerosol transmission of the disease occurs through the inhalation of contaminated materials, and large human outbreaks have been linked to wind dispersion from sites where infected animals are kept.
Recommendations
Therefore, based on the above conclusion the following recommendations are forwarded:
- There should be give attention to proper sanitation when dealing with parturient animals and ensuring proper pasteurization of milk products.
- Immunization of occupationally exposed persons, such as abattoir workers, livestock handlers, veterinarians etc. is advised.
- It is highly imperative that clinically suspected animals in the farm should be prudently investigated for tracing the source of human infection.
- Serological investigation of wildlife should be conducted to identify the reservoirs of Q fever infection.
References
-
Derrick EH (1983) Q fever, a new Fever entity: Clinical features, diagnosis and laboratory investigation. Review infectious disease 5(4): 790- 800.
-
Angelakis E, Roult D (2010) Q fever. Vet Microbiol 140(3-4): 297-309.
-
Tissot-Dupont H, Raoult D (2007) Clinical aspects, diagnosis and treatment of Q fever. Rickettsial Dis pp: 291-301.
-
Carcopino X, Raoult D, Bretelle F, Boubli L, Stein A (2007) Managing Q fever during pregnancy: The benefits of long-term cotrimoxazole therapy. Clinical Infectious Diseases 45(5): 548-555.
-
Maurin M, Raoult D (1999) Q fever. Clinical Microbiol Rev 12(4): 518-553.
-
Rodolakis A (2009) Q fever in Dairy Animals. Fifth International Conference: Annals of New York Academy of Science 1166(1): 90-93.
-
Barlow J, Rauch B, Welcome F, Kim S, Dubovi E, et al. (2008) Association between _Coxiella_ _burnetii_ shedding in milk and subclinical mastitis in dairy cattle. Vet Res 39(3): 23.
-
Philip C, Hoogstraal H, Reiss-Gutfreund R, Clifford C (1996) Evidence of rickettsial disease agents in ticks from Ethiopian cattle. Bull World Health Organ 35(2): 127-131.
-
Abebe A (1990) Prevalence of Q fever infection in the Addis Ababa abattoir. Ethiopia Medical Journal 28(3): 119-122.
-
Pal M (2006) Coxiellosis: A rickettial zoonosis. Veterinary World 4: 127-128.
-
Kovacova E, Kazar J (2002) Q Fever-still a query and underestimated infectious disease. Acta Virol 46(4): 193-210.
-
Aitken I, Bogel K, Cracea E (2010) Q fever in Europe: Current aspects of etiology, epidemiology, human infection, diagnosis and therapy. Infection 15: 323- 327.
-
Bildfell R, Thomson G, Haines D (2000) _Coxiella_ _burnetii_ infection is associated with placentitis in cases of bovine abortion. J Vet Diagn Invest 12(5): 419-425.
-
Angelakis E, Raoult D (2009) Q fever. Veterinary Microbiology 140: 297-309.
-
Babudieri B (1959) Q fever a zoonosis. Advances in Veterinary Science and Comparative Medicine 5: 81- 181.
-
Arricau-Bouvery N, Souriau A, Bodier C, Dufour P, Rousset E, et al. (2005) Effect of vaccination with phase I and phase II _Coxiella burnetii_ vaccines in pregnant goats. Vaccine 23(35): 4392-4402.
-
Berri M, Rousset E, Champion J, Russo P, Rodolakis A (2007) Goats may experience reproductive failures and shed _Coxiella aburnetii_a t two successive parturitions after a Q fever infection. Res Veterinary Sci 83(1): 47-52.
-
Tissot-Dupont H, Thirion X, Raoult D (1994) Q fever serology cut off determination for micro immune fluorescence. Clin Diag Lab Immunol 1(2): 189-196.
-
Gardon J, Heraud J, Laventure S, Ladam A, Capot P, et al. (2007) Suburban transmission of Q fever in French Guiana: Evidence of a wild reservoir. J Infect Dis 184(3): 278-284.
-
Raoult D, Stein A (1994) Q fever during pregnancy a risk for women, fetuses, and obstetricians. New Eng J Med 330(5): 371.
-
Almeida A, Marcili A, Leite RC, Nieri-Bastos FA, Domingues LN, et al. (2012) Coxiella symbiont in the tick Ornithodoros rostratus. Ticks Tick Borne Disease 3(4): 203-206.
-
Fournier P, Etienne J, Harle J, Habib G, Raoult D (2001) Myocarditis, a rare but severe manifestation of Q fever: Report of 8 cases and review of the literature. Clini Infect Dis 32(10): 1440-1447.
-
Amano K, Williams J (1984) Chemical and immunological characterization of lipopolysaccharides from Phase-I and Phase-II Coxiella burnetii. Journal of Bacteriology 160(3): 994- 1002.
-
Hendrix L, Samuel J, Mallavia L (1991) Differentiation of _Coxiella burnetii_ isolates by analysis of restriction- endonuclease-digested DNA separated by SDS-PAGE. J Gen Microbiol 137(2): 269-276.
-
Raoult D, Marrie T (2010) Q fever. Clinical Infectious Diseases 20: 489-496.
-
Raoult D (2005) Natural history and pathophysiology of Q fever. Lancet Infect Dis 5(4): 219-226.
-
Bosnjak E, Hvass A, Villumsen S, Nielsen H (2010) Emerging evidence for Q fever in humans in Denmark: role of contact with dairy cattle. Clin Microbiol Infec 16(8): 1285-1288.
-
Bottcher J, Vossen A, Janowetz B, Alex M, Gangl A, et al. (2011) Insights into the dynamics of endemic _Coxiellaburnetii_ infection in cattle by application of phase-specific Enzyme linked immunosorbant assay in an infected dairy herd. Vet Microbiol 151(3-4): 291-300.
-
McCaughey C, Murray L, McKenna J, Menzies F, McCullough S, et al. (2010) _Coxiella burnetii_ (Q fever) seroprevalence in cattle. Epidemiol Infect 138(1): 21- 27.
-
Paul S, Agger J, Markussen B, Christoffersen A, Agerholm J (2012) Factors associated with _Coxiellaburnetii_antibody positivity in Danish dairy cows. Preven Vet Med 107(1-2): 57-64.
-
Kennerman E, Rousset E, Golcu E, Dufour P (2010) Seroprevalence of Q fever (coxiellosis) in sheep from the Southern Marmara Region, Turkey. Comp Immunol Microbiol Infect Dis 33(1): 37-45.
-
Smit L, Vander F, Winden A, Hooiveld M, Beekhuizen J, et al. (2012) Q fever and pneumonia in an area with a high livestock density: a large population-based study. PloS One 7(6): e38843.
-
McQuiston J, Childs J, Thompson H (2002) Q fever. J Americ Vet Med Assoc 221:796-799.
-
Woldehiwet Z (2004) Q fever (Coxiellosis) epidemiology and pathogenesis. Res Vet Sci 77(2): 93-100.
-
McCaul T, Williams J (1981) Developmental cycle of _Coxiella burnetii_: Structure and morphogenesis of vegetative and sporogenic differentiations_._ J Bacteriol 147(3): 1063-1076.
-
Bennett M, Banazis M (2014) _Coxiella burnetii._ In: Manual of Security Sensitive Microbes and Toxins, Liu D (Ed.), 29th (Chapter), CRC press USA, pp: 333-350.
-
Deretic V (2006) Autophagy in immunity and infection: A Novellmmune Effector. 1st (Edn.), Wiley- Blackwell, New York, pp: 286.
-
Mege J, Maurin M, Capo C, Raoult D (2008) _Coxiella_ _burnetii_ the query fever bacterium; A model of immune subversion by strictly intracellular microorganism. FEMS Microbiology Rev 19(4): 209- 217.
-
Scott G, Williams J (2010) Susceptibility of Coxiella burnetii to chemical disinfectants. Ann New York Academy Sci 590(1): 291-296.
-
Hotta A, Kawamura M, Andoh H, Yamaguchi M, Fukushi T, et al. (2002) Phase variation analysis of _Coxiella burnetii_ during serial passage in cell culture by use of monoclonal antibodies. Inf Immunity 70(8): 4747-4749.
-
Marrie T, Stein A, Janigan D, Raoult D (1996) Route of infection determines the clinical manifestations of acute Q fever. J Infect Dis 173(2): 484-487.
-
Lang G (1994) Q fever. Cantus Veterinary Journal 35:
-
Agerholm JS (2013) _Coxiella burnetii_ associated reproductive disorders in domestic animals-acritical review. Acta Vet Scandinavia 55: 13.
-
Nielsen K, Nielsen S, Agger J, Christoffersen A, Agerholm J (2011) Association between antibodies to _Coxiella burnetii_ in bulk tank milk and prenatal mortality of Danish dairy calves. Acta Veterinarian Scandinavian 53: 64.
-
Fournier P, Marrie T, Raoult D (1998) Diagnosis of Q fever. J Clin Microbiol 36(7): 1823-1834.
-
Bernit E, Pouget J, Janbon F, Dutronc H, Martinez P, et al. (2002) Neurological involvement in acute Q fever - A report of 29 cases and review of the literature. Archives Internal Med 162(6): 693-700.
-
Sidi-Boumedine K, Rousset E, Henning K, Ziller M, Niemczuk K, et al. (2010) Development of harmonized schemes for the monitoring and reporting of Q fever in animals in the European union. EFSA Scientific Report.
-
Berri M, Laroucau K, Rodolakis A (2000) The detection of _Coxiella burnetii_ from ovine genital swabs, milk and fecal samples by the use of a single touchdown polymerase chain reaction. Veterinary Microbiology 72(3-4): 285-293.
-
Martinov S (2007) Studies on Mastitis in Sheep, Caused by _Coxiella burnetii_. Biotechnol Biotechnol Equip 21(4): 484-490.
-
Berii M, Rekiki A, Boumedine S, Rodolakis A (2009) Simultaneous differential detection of Chlamydophilaabortus, Chlamydophiapecorum and coxiella burnetii from aborted ruminants clinical samples using multiplex PCR. BMC Microbiol 9(130): 1471-2180.
-
Kovacova E, Kazar J, Spanelova D (1998) Suitability of various _Coxiella burnetii_ antigen preparations for detection of serum antibodies by various tests. Acta Virologica 42(6): 365-368.
-
Horigan M, Bell M, Pollard T, Sayers A, Pritchard G (2011) Q fever diagnosis in domestic ruminants: comparison between complement fixation and commercial enzyme-linked immune sorbent assays. J Vet Diagn Invest 23(5): 924-931.
-
Herremans T, Hogema B, Nabuurs M, Peeters, M, Wegadam-Blans M, et al. (2013) Comparison of the performance of IFA, CFA and elisa as says for the serodiagnosis of acute Q fever by quality assessment diagnost. Microbiol Infect Dis 75(1): 16-21.
-
Peter O, Dupuis G, Burgdorfer W, Peacock M (1985) Evaluation of the complement-fixation and indirect immune fluorescence tests in the early diagnosis of primary Qfever. Eur J Clini Microbiol 4(4): 394-396.
-
Nielsen S, Andersen A, Molbak K, Hjollund N, Kantso B, et al. (2013) No excess risk of adverse pregnancy outcomes among women with serological markers of previous infection with _Coxiellaburnetii_: evidence from the Danish National Birth Cohort. BMC Inf Dis 13: 87.
-
Paul S (2013) Seroepidemiology of _Coxiella burnetii_ in Danish Cattle, University of Copenhagen Denmark PhD Thesis.
-
Peter O, Dupuis G, Peacock M, Burgdorfer W (1987) Comparison of enzyme-linked immunosorbant assay and complement fixation and indirect fluorescent- antibody tests for detection of _Coxiella burnetii_ antibody. J Clini Microbiol 25(6): 1063-1067.
-
Emery M, Ostlund E, Schmitt B (2012) Comparison of Q fever serology methods in cattle, goats, and sheep. J Vet Diagnos Inv 24(2): 379-382.
-
Rousset E, Duquesne V, Russo P, Aubert M (2010) Q fever. Manual of diagnostic tests and vaccines for terrestrial animals. World Organization for Animal Health (OIE), Paris, France.
-
Fenollar F, Raoult D (2007) Molecular diagnosis of bloodstream infections caused by non-cultivable bacteria. Int J Antimicro Agents 30: S7-S15.
-
Berri M, Arricau-Bouvery N, Rodolakis A (2003) PCR- based detection of _Coxiella burnetii_ from clinical samples. Methods Molecul Biol 216: 153-161.
-
Philadelphia P (2002) Q fever. 8th (Edn.), In: Mark veterinary manual. National publishing Inc., pp: 486- 487.
-
CFSPH (2017) Q-fever, public health risk.
-
Roest H, Ruuls R, Tilburg J, Nabuurs-Franssen M, Klaassen C, et al. (2011) Molecular epidemiology of _Coxiellaburnetii_from ruminants in Q fever outbreak, the Netherlands. Emerg Inf Dis 17(4): 668-675.
-
Georgiev M, Afonso A, Neubauer H, Needham H, Thiery R, et al. (2013) Q fever in humans and farm animals in four European countries, 1982 to 2010. Euro surveill 18(8): 204-07.
-
Astobiza I, Barandika J, Ruiz-Fons F, Hurtado A, Povedano I, et al. (2011) Four-year evaluation of the effect of vaccination against _Coxiella burnetii_ on reduction of animal infection and environmental contamination in a naturally infected dairy sheep flock. Appl Environ Microbiol 77(20): 7405-7407.
-
Gajdosova E, Kovacova E, Toman R, Skultety L, Lukacova M, et al. (1994) Immunogenicity of _Coxiella_ _burnetii_ whole cells and their outer membrane components. Acta Virol 38(6): 339-344.
-
Krauss H (1989) Clinical aspects and prevention of Q fever in animals. Eur J Epidemiol 5(4): 454-455.
-
Cantas H, Muwonge A, Sareyyupoglu B, Yardimci H, Skjerve E (2011) Q fever abortions in ruminants and associated on-farm risk factors in northern Cyprus. BMC Vet Res 7: 13.
-
Capuano F, Landolfi M, Monetti DM (2001) Influence of three types of farm management on the seroprevalence of Q fever as assessed by an indirect immune fluorescence assay. Vet Rec 149(22): 669- 671.
-
De Bruin A, Van der Plaats J, De Heer L, Paauwe R, Schimmer B (2012) Detection of Coxiella burnetii DNA on small-ruminant farms during a Q fever outbreak in the Netherlands. Appl Environ Microbiol 78(6): 1652-1657.
-
Eldin C, Mahamat A, Demar M, Abboud M, Djossou F, (2014) Q fever in French Guiana. Am J Trop Med Hyg 91(4): 771-776.
-
Garcia-Ispierto I, Lopez-Helguera I, Tutusaus J, Serrano B, Monleon E, et al. (2013) _Coxiella burnetii_ shedding during the peripartum period and subsequent fertility in dairy cattle. Reprod Domest Anim 48(3): 441-446.
-
Hellenbrand W, Breuer T, Petersen L (2001) Changing epidemiology of Q fever in Germany, 1947-1999. Emerg Inf Dis 7(5): 789-796.
-
Hollenbeck B, Gannon S, Qinan Q, Grad Y (2015) Genome sequence and analysis of resistance and virulence determinants in a strain of neisseria mucosa causing native-valve endocarditis. JMM case Report 2(3).
-
Kersh G, Fitzpatrick K, Self J, Priestely R, Kelly AJ, et al. (2013) Presence and persistence of Coxiellaburnetii in the environments of goat farms associated with a Q fever outbreak. Appl Environ Microbiol 79(5): 1697- 1703.
-
Madariaga MG, Rezai K, Trenholme GM, Weinstein RA (2003) Q fever: a biological weapon in your backyard. Lancet Infect Dis 3(11): 709-721.
-
Marrie T (2007) Epidemiology of Q fever. Rickettial Diseases pp: 281-289.
-
Marrie TJ, Pollak PT (1995) Seroepidemiology of Q fever in Nova Scotia: evidence for age dependent cohorts and geographical distribution. Europ J Epidemiol 11(1): 47-54.
-
Philip C, Hoogstraal H, Reiss-Gutfreund R, Clifford C (1996) Evidence of rickettsial disease agents in ticks from Ethiopian cattle. Bull World Health Organ 35(2): 127-131.
-
Roest H (2013) _Coxiella burnetii_ in pregnant goats. Department of Bacteriology Central Veterinary institute of Wageningen, Netherland Ph.D Thesis.
-
Roult D, Vestris G, Enea M (1990) isolation of 16 strains of Coxiella burnetii from patients by using a sensitive centrifugation cell culture system and establishment of the strains in HELcells. J Clinic Microbiol 28(11): 2482-2484.
-
TomanR, Heinzen R, Samet J, Mege J (2012) _CoxiellaBurneti_. Recent Advances and new perspectives in Research of the Q fever bacterium. Springer New York, USA, 13: 406.
- In Situ Evaluation of the Anthelmintic Effect of the Aqueous Extract of Syzygium aromaticum (L) Merr and Perry on Bovine Strongyles
- Successful in Vitro Embryo Production with Oocytes Aspirated from Live White-Tailed Deer (Odocoileus Virginianus Texanus) Donors under Captivity in Northeast Mexico
- Bangladeshi Finches with their Evolutionary Thoughts (Aves: Passeriformes)
- Note on the Survival Status of Przewalski’s Horse, Equus ferus przewalskii (Perissodactyla: Equidae)
- In-Situ and Ex-Situ Protection of White-Breasted Waterhen (Amaurornis Phoenicurus) (Pennant, 1769) (Aves: Rallidae)
- Meat Examination in the Laboratory, the Acceptability and the Human Health